Increased Incidence of Kawasaki Disease in Taiwan in Recent Years: A 15 Years Nationwide Population-Based Cohort Study
 Ying-Hsien Huang
Ying-Hsien Huang Kuan-Miao Lin3†
Kuan-Miao Lin3†  Ho-Chang Kuo
Ho-Chang Kuo- 1Department of Pediatrics, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Kaohsiung, Taiwan
- 2Kawasaki Disease Center, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
- 3Department of Pediatrics, Chiayi Chang Gung Memorial Hospital, Chiayi, Taiwan
- 4Department of Public Health, College of Health Sciences, Kaohsiung Medical University, Kaohsiung, Taiwan
Background: Kawasaki disease (KD) is diagnosed in children suffering from fever for more than five days and five clinical characteristic symptoms. The aim of this article was to research the clinical characteristics among KD children in Taiwan in recent years through a population-based cohort study.
Materials and Methods: We carried out a nationwide retrospective cohort study by analyzing the data of KD patients (ICD-9-CM code 4461) from Taiwan's National Health Insurance Research Database (NHIRD) during the period of 1996-2011.
Results: Among all the insured children in the NHIRD, insurance claims data were reported for 13,260 patients diagnosed with KD, with 8394 (63.30%) subjects being administered IVIG for treatment. Of the patients diagnosed with KD, 94% were under the age of 5 years old, and the majority of cases occurred in May. Furthermore, the incidence of KD more than doubled (28.58–60.08 per 100,000) during this period in Taiwan.
Conclusion: We developed a five-based mnemonic device for parents and first-line clinicians to easily use in order to diagnose KD. We also observed an increased incidence of KD in Taiwan during the study period. In addition, we develop a five-based mnemonic device for parents and first-line clinicians in clinical diagnosis of KD can easily remember: Fever> 5 days, 5 clinical criteria, predominantly in children <5 years of age, and peak seasonal clustering in the 5th month, May (April–June) in Taiwan.
Introduction
Kawasaki disease (KD) is an acute febrile vasculitis syndrome that affects various systems, has an unknown etiology, and generally occurs in children under the age of 5 years old (1). KD is diagnosed in children who have a prolonged fever for more than 5 days, and five major clinical signs (2). The vascular involvement of KD occurs in both small and medium-sized blood vessels, particularly the coronary arteries (3). The most serious complication of KD is a coronary artery lesion (CAL), including myocardial infarction, and coronary artery aneurysms (CAA) (4). Approximately 20% of untreated children developed a sequelae of vasculitis with a coronary artery aneurysm (5). A U.S. multicenter study determined that a single high-dose of 2 g/kg intravenous immunoglobulin (IVIG) plus aspirin can lower the incidence of CAA from 20–25% to 3–5%, as well as reduce fever duration (6).
The global prevalence of KD in children is highest (218/105) in Japan and the lowest (4.7/105) in children of European descent, while Taiwan has an incidence of 66/105 (2). However, a larger population-based cohort study is required to confirm these observations and determine the clinical characteristics of KD children. Therefore, in the present study, we aimed to examine both the incidence and clinical characteristics of KD patients in a nationwide KD dataset obtained from the health care database of Taiwan's National Health Insurance (NHI).
Methods
In this study, we used data from the medical claims database of Taiwan's National Health Institute (NHI) program. Implemented in Taiwan on March 1, 1995, the NHI program provides compulsory universal health insurance and has information about nearly 99% of the 23.74 million residents of Taiwan based on ethical democratic principles (7). Previous studies have described in detail the National Health Insurance Research Database (NHIRD) (8, 9), which contains such medical information as insured individuals' inpatient and outpatient care facilities, prescriptions, gender, date of birth, date of visit or hospitalization, and diagnosis. All diagnoses are coded using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) format. Information from the NHIRD database has been shown to be complete, reliable, and accurate for use in epidemiological studies (7).
Children diagnosed with KD (ICD-9: 4461) under the age of 20 years old include untreated KD, KD with aspirin administration, and KD with IVIG administration. Coronary artery aneurysm (CAA) was coded as 414.11 in the ICD-9-CM. We defined KD recurrence as a period of >1 month between two hospitalizations.
We identified and enrolled a cohort of 13,260 KD patients between January 1997 and December 2011 in this study. All patients were categorized into one of the following three groups: ICD-9+Aspirin, which was defined as patients with two visits within 60 days that received aspirin therapy; ICD-9+IVIG, which was defined as inpatients that received IVIG treatment at diagnosis; and ICD-9 without IVIG, which was defined as inpatients that did not receive IVIG or aspirin treatment. The ICD-9+IVIG group was a specific indicator of KD in the acute stage, while the ICD-9+Aspirin group was a specific indicator of KD in the afebrile stage upon diagnosis. The present study was exempt from full review by Chang Gung Memorial Hospital's Institution Review Board (IRB No.102-0364B) because the patients' identification numbers in the database were encrypted to protect their privacy (10).
Statistical Analysis
The differences between these three KD groups of sex, age group (<1, ≥1~ <2, ≥2~ <3, ≥3~ <4, ≥4~ <5, and ≥5 years-old), and CAA were analyzed by the Pearson chi-square test. The year-specific incidence rates (per 1000 person-y) of KD were calculated by dividing the number of newly diagnosed KD by the total number of children below 5 years of age in Taiwan each year. The annual incidence rate of KD was calculated as the number of KD per 100,000 children <5 years of age. We performed all analyses using the SAS statistical package (version 9.3; SAS Institute Inc., Cary, NC, USA). Significance was assigned for p < 0.05.
Results
Clinical Characteristic of KD
The purpose of this study was to analyze the general characteristics and annual incidence of KD by collecting patients' data from the ICD-9+IVIG and ICD-9+Aspirin groups. The study participants' general characteristics are summarized in Table 1. We analyzed 13,260 children diagnosed with KD (ICD-9) under 20 years old in the period between January 1997 and December 2011. Of those, 4614 (35%) were categorized as KD alone (ICD-9), 8394 (63%) as KD with IVIG administration (ICD-9+ IVIG), and 252 (2%) as KD with only aspirin administration (ICD-9+ Aspirin). Of the 8646 patients in the ICD-9+IVIG and ICD-9+ Aspirin groups, the male-to-female ratio was approximately 1.32 (4918/3728), and 8113 (94%) were <5 years old. The incidence of coronary artery aneurysm (CAA) was 10–12%, with a recurrence rate of 2% in ICD-9+ IVIG and ICD-9+ Aspirin groups and 8% with a recurrence rate of 1% in ICD-9+ IVIG and ICD-9 alone groups. Interestingly, patients in the ICD-9 group without IVIG or aspirin treatment demonstrated no significant gender difference (male-to-female ratio = 1.03), which may indicate that this group was not in the acute stage, was not used for the coronary arteries survey, or was the result of overdiagnosis or misdiagnosis (11).
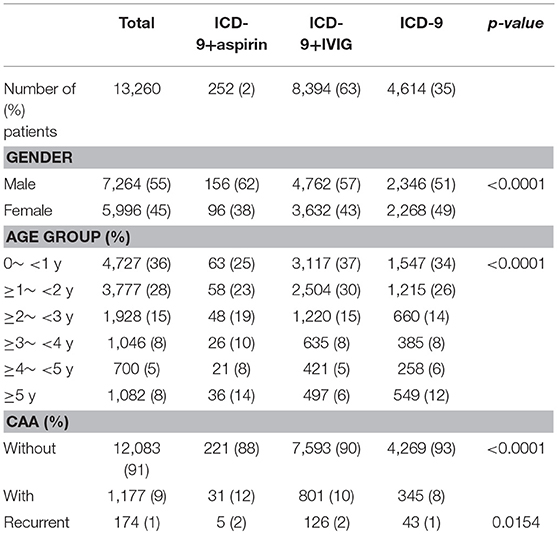
Table 1. General characteristics of study participants.
The Seasonality of Kawasaki Disease in Taiwan
Table 2 shows KD patient distributions by month. In the ICD-9 + IVIG group, the peak months of distribution were April-June, while patient distributions decreased in the winter months (November–February). The monthly distribution trends were similar in children <5 years old (Table 3, Figure 1). The annual incidence rates per 100,000 children <5 years old are shown in Table 4.
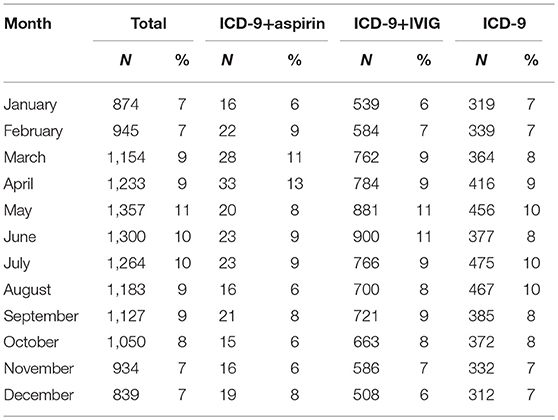
Table 2. Patient distribution by month of study participants under the age of 20 years old.
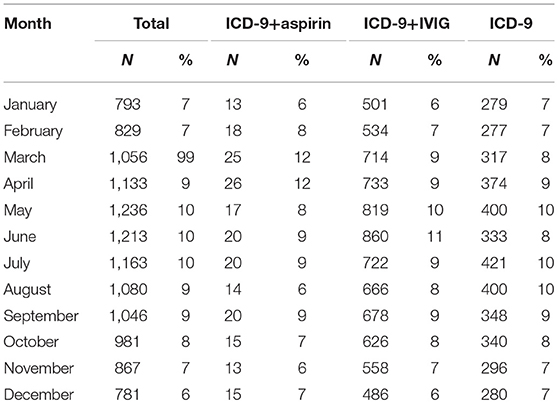
Table 3. Patient distribution by month of study participants under the age of 5 years old.

Figure 1. The seasonality of Kawasaki disease in Taiwan.
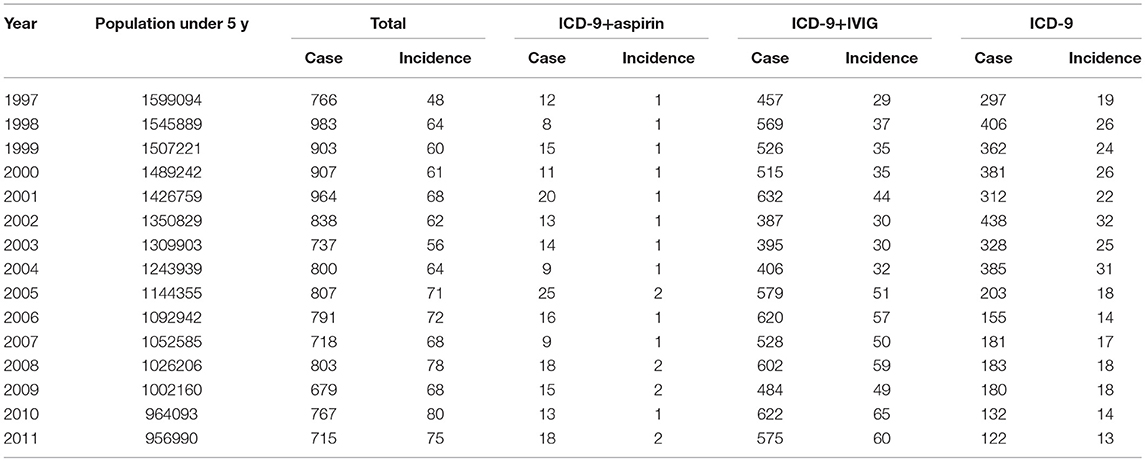
Table 4. Incidence of study participants under the age of 5 years old.
The increased incidence of KD in recent years in Taiwan
Since the ICD-9+ IVIG and ICD-9+Aspirin groups were diagnosed with KD more accurately in Taiwan's NHI health care database, we found that the incidence ranged from 29.3 to 62.0 per 100,000 children from 1997 to 2011 among these patients. The average incidence from 1997 to 2011 was 45.2 per 100,000 children under the age of 5 years old. Overall, the incidence of KD in Taiwan has significantly increased in recent years. We also found that the incidences decreased from 18.6 to 12.8 per 100,000 children from 1997 to 2011 in the ICD-9 alone group, indicating that both the increased accuracy of KD diagnosis and the incidence discrepancy between the two groups were also significant (Figure 2).
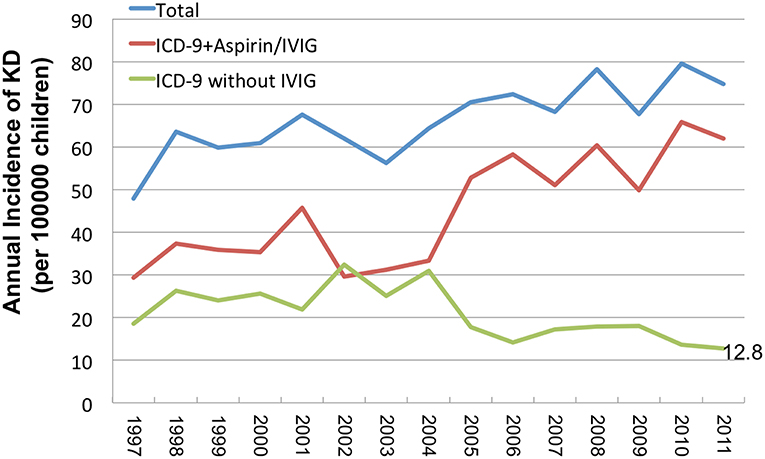
Figure 2. The increased incidence of KD in recent years in Taiwan.
Discussion
Today, KD is commonly diagnosed and reported in global populations, especially in Asia (12). We have observed that the incidence of KD has increased in recent years in Taiwan, as well as in Beijing and Japan (13, 14). Determining whether this observation is the result of increased diagnosis due to improved awareness and/or access to specialist medical services or reflective of an actual increase in incidence is difficult (15). Both factors likely play a role in many countries, particularly in those countries where KD has been described more recently (16).
With regard to age, KD generally occurs in children <5 years old, which represents the turning point of the host's immune maturation (15). Therefore, KD may be associated with the maturing immune system of young children (11). Furthermore, with regard to gender, our study showed that KD occurs more commonly in the male gender (17). Overall, KD incidence has increased considerably (18) with the increased incidence of allergic diseases worldwide (19). In previous studies, we also discovered that children with KD were at a higher risk of developing atopic dermatitis during the 5 year follow-up period than the control group (10), as well as for allergic diseases in a population-based matched cohort study (8).
According to pathologic studies and climatologic studies, the seasonality of KD may be associated with such triggers as environmental factors or infectious pathogens (20). Our results indicate that the peak months of KD in Taiwan are April, May, and June, which is in line with a previous study that observed an increased incidence of KD in Taiwan during the summer (21). However, Japan and Korea have been found to have two peaks of seasonal incidence- winter and summer, while the peak incidence of KD in China was observed as spring and summer (22), with results that resemble those of our study. A global prospective study found that KD case numbers were greater in January through March in the extra-tropic region of the Northern Hemisphere but showed weak significance in seasonal variation in the tropic and the Southern Hemisphere extra-tropics region due to scarce data collection (23). To explain seasonal variations, Abrams et al. reviewed KD cases from 1991 to 2004 in Japan and suggested that the increased incidence was associated with higher precipitation and lower temperatures in the 2 months prior to disease onset (24). The hypothesized “tropospheric wind pattern” mechanism helps explain the three major KD epidemic occurrences in Japan, which occurred in 1979, 1982, and 1986. Said seasonal wind may bring the supposed KD agent across the Northern Hemisphere and has allowed scientists to observe the relationship to KD seasonality (25).
The key to preventing CAL in KD patients is timing the diagnosis and administration of IVIG. In our study, we combined clinical presentations with KD characteristics to develop a five-based mnemonic device for KD that parents and first-line clinicians in clinical diagnosis of KD can easily remember: Fever >5 days, 5 clinical criteria, predominantly in children <5 years of age, and peak seasonal clustering in the 5th month, May (April–June). Clinical diagnosis criteria (Kuo Mnemonic: 1-2-3-4-5) include diffuse mucosal inflammation with strawberry tongue and fissure lips (1 mouth), bilateral non-purulent conjunctivitis (2 eyes), unilateral cervical lymphadenopathy (3 fingers check lymph node), indurative angioedema over the hands and feet (4 limbs), dysmorphic skin rashes (5 or more skin rashes) as our previous report (3).
Our study has some limitations that should be mentioned at this point. First, our study was a single-country study, but the seasonality of epidemiology should be discussed throughout the climate zone. Second, the climate has changed considerably in recent years due to global warming, which may affect seasonal clustering. Furthermore, we did not perform an in-depth analysis of atypical temperature changes, which may have increased the incidence in other months in recent years. Third, data from years ago may under-estimate the incidence of KD due to clinicians' insufficient education or pediatric medication being less popularized. In the future, we need additional worldwide studies to analyze the epidemiology and seasonal effects of KD.
Conclusion
We have observed an increased incidence of KD in recent years, with a higher incidence in children under the age of 5 years old and a seasonal peak during April–June. Based on our clinical presentation, we developed a five-based mnemonic for KD that parents and first-line clinicians in the clinical diagnosis of KD can easily remember: Fever >5 days, 5 clinical criteria, predominantly in children <5 years of age, and peak seasonal clustering in the 5th month, May (April–June) in Taiwan.
Author Contributions
Y-HH and K-ML wrote the manuscript. S-CH calculated data. J-HY and M-HL collected data. H-CK final proof check before submission.
Funding
This study was funded by the following grants: MOST: 105-2314-B-182-050-MY3 and MOST 103-2410-H-264-004 from the Ministry of Science and Technology of Taiwan and CMRPG8F1911, 1921, 1931, and 1941, and 8E0212 from Chang Gung Memorial Hospital in Taiwan. While these institutes provided financial support, they had no influence on the way we collected, analyzed, or interpreted the data or wrote this manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Kawasaki T, Kosaki F, Okawa S, Shigematsu I, Yanagawa H. A new infantile acute febrile mucocutaneous lymph node syndrome (MLNS) prevailing in Japan. Pediatrics. (1974) 54:271–6.
2. Wang CL, Wu YT, Liu CA, Kuo HC, Yang KD. Kawasaki disease: infection, immunity and genetics. Pediatr Infect Dis J. (2005) 24:998–1004. doi: 10.1097/01.inf.0000183786.70519.fa
3. Kuo HC. Preventing coronary artery lesions in Kawasaki disease. Biomed J. (2017) 40:141–6. doi: 10.1016/j.bj.2017.04.002
4. Liang CD, Kuo HC, Yang KD, Wang CL, Ko SF. Coronary artery fistula associated with Kawasaki disease. Am Heart J. (2009) 157:584–8. doi: 10.1016/j.ahj.2008.11.020
5. Newburger JW, Takahashi M, Burns JC, Beiser AS, Chung KJ, Duffy CE, et al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N Engl J Med. (1986) 315:341–7. doi: 10.1056/NEJM198608073150601
6. Newburger JW, Takahashi M, Beiser AS, Burns JC, Bastian J, Chung KJ, et al. A single intravenous infusion of gamma globulin as compared with four infusions in the treatment of acute Kawasaki syndrome. N Engl J Med. (1991) 324:1633–9. doi: 10.1056/NEJM199106063242305
7. Cheng TM. Reflections on the 20th anniversary of Taiwan's single-payer national health insurance system. Health Aff. (2015) 34:502–10. doi: 10.1377/hlthaff.2014.1332
8. Kuo HC, Chang WC, Yang KD, Yu HR, Wang CL, Ho SC, et al. Kawasaki disease and subsequent risk of allergic diseases: a population-based matched cohort study. BMC Pediatr. (2013) 13:38. doi: 10.1186/1471-2431-13-38
9. Chang WP, Wu SJ, Chang WC, Kuo HC. Population-based study of the association between urbanization and Kawasaki disease in Taiwan. ScientificWorldJournal. (2013) 2013:169365. doi: 10.1155/2013/169365
10. Woon PY, Chang WC, Liang CC, Hsu CH, Klahan S, Huang YH, et al. Increased risk of atopic dermatitis in preschool children with kawasaki disease: a population-based study in taiwan. Evid Based Complement Alternat Med. (2013) 2013:605123. doi: 10.1155/2013/605123
11. Lee KY, Han JW, Lee JS. Kawasaki disease may be a hyperimmune reaction of genetically susceptible children to variants of normal environmental flora. Med Hypotheses. (2007) 69:642–51. doi: 10.1016/j.mehy.2006.12.051
12. Rowley AH, Shulman ST. The epidemiology and pathogenesis of Kawasaki disease. Front Pediatr. (2018) 6:374. doi: 10.3389/fped.2018.00374
13. Du ZD, Zhao D, Du J, Zhang YL, Lin Y, Liu C, et al. epidemiologic study on Kawasaki disease in Beijing from 2000 through 2004. Pediatr Infect Dis J. (2007) 26:449–51. doi: 10.1097/01.inf.0000261196.79223.18
14. Makino N, Nakamura Y, Yashiro M, Sano T, Ae R, Kosami K, et al. Epidemiological observations of Kawasaki disease in Japan, 2013-2014. Pediatr Int. (2018) 60:581–7. doi: 10.1111/ped.13544
15. Looman KIM, Jansen MAE, Voortman T, van den Heuvel D, Jaddoe VWV, Franco OH, et al. The role of vitamin D on circulating memory T cells in children: the generation R study. Pediatr Allergy Immunol. (2017) 28:579–87. doi: 10.1111/pai.12754
16. Liu YC, Lin MT, Wang JK, Wu MH. State-of-the-art acute phase management of Kawasaki disease after 2017 scientific statement from the American Heart Association. Pediatr Neonatol. (2018) 59:543–52. doi: 10.1016/j.pedneo.2018.03.005
17. Saundankar J, Yim D, Itotoh B, Payne R, Maslin K, Jape G, et al. The epidemiology and clinical features of Kawasaki Disease in Australia. Pediatrics. (2014) 133:e1009–e14. doi: 10.1542/peds.2013-2936
18. Harnden A, Mayon-White R, Perera R, Yeates D, Goldacre M, Burgner D. Kawasaki disease in England: ethnicity, deprivation, and respiratory pathogens. Pediatr Infect Dis J. (2009) 28:21–4. doi: 10.1097/INF.0b013e3181812ca4
19. Peden DB. The epidemiology and genetics of asthma risk associated with air pollution. J Allergy Clin Immunol. (2005) 115:213–9; quiz 220. doi: 10.1016/j.jaci.2004.12.003
20. Burns JC, Cayan DR, Tong G, Bainto EV, Turner CL, Shike H, et al. Seasonality and temporal clustering of Kawasaki syndrome. Epidemiology. (2005) 16:220–5. doi: 10.1097/01.ede.0000152901.06689.d4
21. Huang WC, Huang LM, Chang IS, Chang LY, Chiang BL, Chen PJ, et al. Epidemiologic features of Kawasaki disease in Taiwan, 2003-2006. Pediatrics. (2009) 123:e401–5. doi: 10.1542/peds.2008-2187
22. Uehara R, Belay ED. Epidemiology of Kawasaki disease in Asia, Europe, and the United States. J Epidemiol. (2012) 22:79–85. doi: 10.2188/jea.JE20110131
23. Burns JC, Herzog L, Fabri O, Tremoulet AH, Rodo X, Uehara R, et al. Seasonality of Kawasaki disease: a global perspective. PLoS ONE. (2013) 8:e74529. doi: 10.1371/journal.pone.0074529
24. Abrams JY, Blase JL, Belay ED, Uehara R, Maddox RA, Schonberger LB, et al. Increased Kawasaki Disease incidence associated with higher precipitation and lower temperatures, Japan, 1991-2004. Pediatr Infect Dis J. (2018) 37:526–30. doi: 10.1097/INF.0000000000001838
Keywords: Kawasaki disease, incidence, cohort study, Taiwan's National Health Insurance Research Database, seasonality
Citation: Huang Y-H, Lin K-M, Ho S-C, Yan J-H, Lo M-H and Kuo H-C (2019) Increased Incidence of Kawasaki Disease in Taiwan in Recent Years: A 15 Years Nationwide Population-Based Cohort Study. Front. Pediatr. 7:121. doi: 10.3389/fped.2019.00121
Received: 28 January 2019; Accepted: 12 March 2019;
Published: 29 March 2019.
Edited by:
Maurice Beghetti, Geneva University Hospitals (HUG), SwitzerlandReviewed by:
Brian McCrindle, Hospital for Sick Children, CanadaNicole Sekarski, Lausanne University Hospital (CHUV), Switzerland
Copyright © 2019 Huang, Lin, Ho, Yan, Lo and Kuo.This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ho-Chang Kuo, erickuo48@yahoo.com.tw
†These authors have contributed equally to this work