Digital Attention-Related Augmented-Reality Game: Significant Correlation between Student Game Performance and Validated Clinical Measures of Attention-Deficit/Hyperactivity Disorder (ADHD)


Abstract
:1. Introduction
2. Methodology
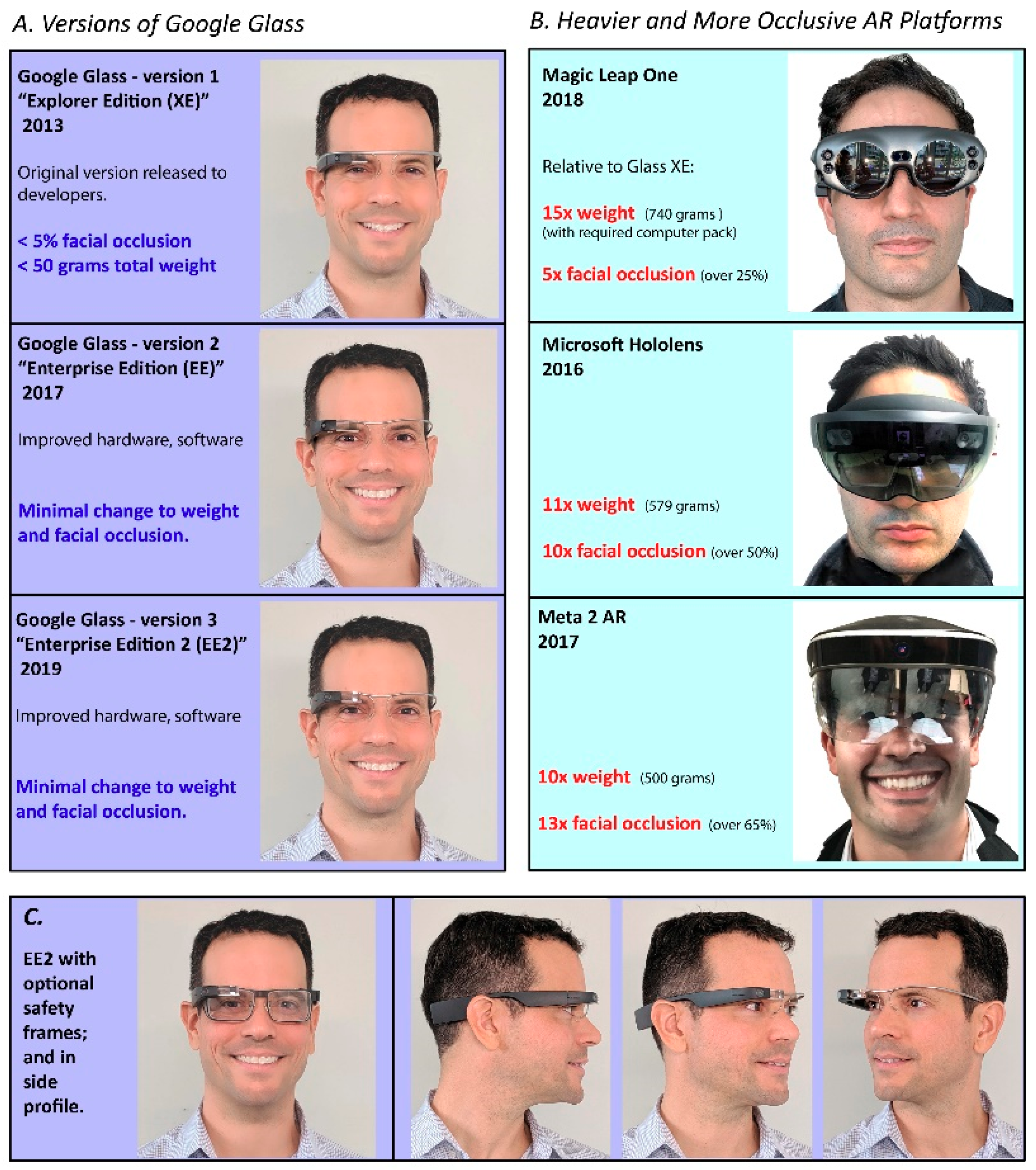
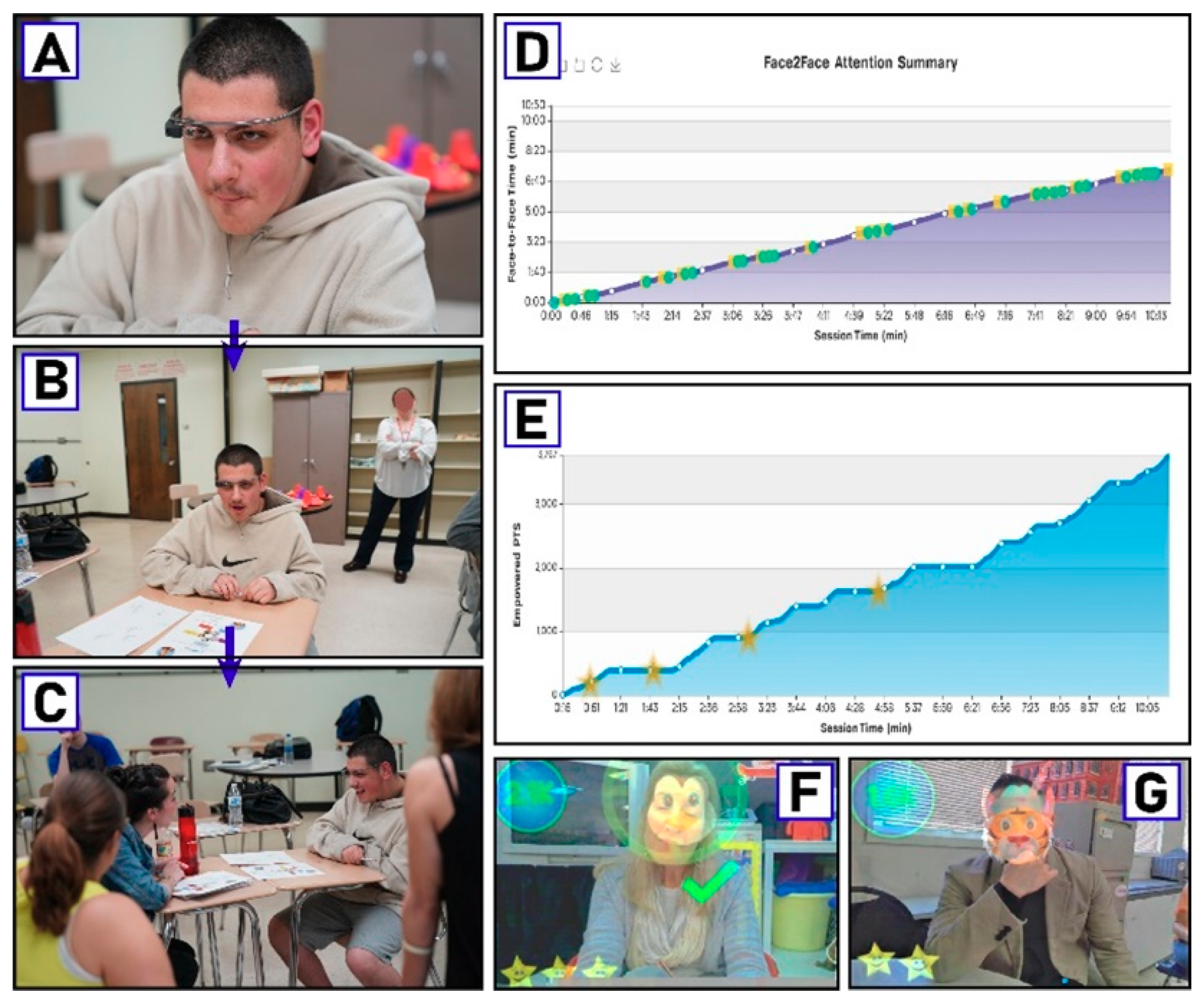
2.1. Technological Background
2.2. Study Design
2.3. Outcome Measures
2.4. Participants and Setting
2.5. Consent and Institutional Review Board Status
3. Results
4. Discussion
5. Conclusion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); APA Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Shattuck, P.T.; Narendorf, S.C.; Cooper, B.; Sterzing, P.R.; Wagner, M.; Taylor, J.L. Postsecondary education and employment among youth with an autism spectrum disorder. Pediatrics 2012, 129, 1042–1049. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.L.; Mailick, M.R. A longitudinal examination of 10-year change in vocational and educational activities for adults with autism spectrum disorders. Dev. Psychol. 2014, 50, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Kohane, I.S.; McMurry, A.; Weber, G.; MacFadden, D.; Rappaport, L.; Kunkel, L.; Bickel, J.; Wattanasin, N.; Spence, S.; Murphy, S.; et al. The co-morbidity burden of children and young adults with autism spectrum disorders. PLoS ONE 2012, 7, e33224. [Google Scholar] [CrossRef] [PubMed]
- Eaves, L.C.; Ho, H.H. Young adult outcome of autism spectrum disorders. J. Autism Dev. Disord. 2008, 38, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Roux, A.M.; Shattuck, P.T.; Cooper, B.P.; Anderson, K.A.; Wagner, M.; Narendorf, S.C. Postsecondary employment experiences among young adults with an autism spectrum disorder. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Leyfer, O.T.; Folstein, S.E.; Bacalman, S.; Davis, N.O.; Dinh, E.; Morgan, J.; Tager-Flusberg, H.; Lainhart, J.E. Comorbid psychiatric disorders in children with autism: Interview development and rates of disorders. J. Autism Dev. Disord. 2006, 36, 849–861. [Google Scholar] [CrossRef] [PubMed]
- Simonoff, E.; Pickles, A.; Charman, T.; Chandler, S.; Loucas, T.; Baird, G. Psychiatric disorders in children with autism spectrum disorders: Prevalence, comorbidity, and associated factors in a population-derived sample. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Chiang, H.L.; Kao, W.C.; Chou, M.C.; Chou, W.J.; Chiu, Y.N.; Wu, Y.Y.; Gau, S.S. School dysfunction in youth with autistic spectrum disorder in Taiwan: The effect of subtype and ADHD. Autism Res. 2018, 11, 857–869. [Google Scholar] [CrossRef] [PubMed]
- Loe, I.M.; Feldman, H.M. Academic and educational outcomes of children with ADHD. J. Pediatr. Psychol. 2007, 32, 643–654. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.J. Attention-deficit/hyperactivity disorder in the context of autism spectrum disorders. Curr. Psychiatry Rep. 2010, 12, 382–388. [Google Scholar] [CrossRef]
- Joshi, G.; Faraone, S.V.; Wozniak, J.; Tarko, L.; Fried, R.; Galdo, M.; Furtak, S.L.; Biederman, J. Symptom profile of ADHD in Youth with high-functioning autism spectrum disorder: A comparative study in psychiatrically referred populations. J. Atten. Disord. 2017, 21, 846–855. [Google Scholar] [CrossRef] [PubMed]
- Research Units on Pediatric Psychopharmacology Autism Network. Randomized, controlled, crossover trial of methylphenidate in pervasive developmental disorders with hyperactivity. Arch. Gen. Psychiatry 2005, 62, 1266–1274. [Google Scholar] [CrossRef] [PubMed]
- Erickson, C.A.; Posey, D.J.; Stigler, K.A.; Mullett, J.; Katschke, A.R.; McDougle, C.J. A retrospective study of memantine in children and adolescents with pervasive developmental disorders. Psychopharmacology 2007, 191, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Collett, B.R.; Ohan, J.L.; Myers, K.M. Ten-year review of rating scales. V: Scales assessing attention-deficit/hyperactivity disorder. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 1015–1037. [Google Scholar] [CrossRef] [PubMed]
- Bied, A.; Biederman, J.; Faraone, S. Parent-based diagnosis of ADHD is as accurate as a teacher-based diagnosis of ADHD. Postgrad. Med. 2017, 129, 375–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogundele, M.O.; Ayyash, H.F.; Banerjee, S. Role of computerised continuous performance task tests in ADHD. Prog. Neurol. Psychiatry 2011, 15, 8–13. [Google Scholar] [CrossRef]
- Hall, C.L.; Valentine, A.Z.; Groom, M.J.; Walker, G.M.; Sayal, K.; Daley, D.; Hollis, C. The clinical utility of the continuous performance test and objective measures of activity for diagnosing and monitoring ADHD in children: A systematic review. Eur. Child Adolesc. Psychiatr. 2016, 25, 677–699. [Google Scholar] [CrossRef] [PubMed]
- Jarow, J.P.; LaVange, L.; Woodcock, J. Multidimensional evidence generation and FDA regulatory decision making: Defining and using “real-world” data. JAMA 2017, 318, 703–704. [Google Scholar] [CrossRef]
- Lovejoy, M.C.; Rasmussen, N.H. The validity of vigilance tasks in differential diagnosis of children referred for attention and learning problems. J. Abnorm. Child Psychol. 1990, 18, 671–681. [Google Scholar] [CrossRef]
- Trommer, B.L.; Hoeppner, J.-A.B.; Lorber, R.; Armstrong, K. Pitfalls in the use of a continuous performance test as a diagnostic tool in attention deficit disorder. J. Dev. Behav. Pediatr. 1988, 9, 339–345. [Google Scholar] [CrossRef]
- Constantino, J.N.; Gruber, C.P. Social Responsiveness Scale (SRS); Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Achenbach, T.M. Child Behavior Checklist and Related Instruments. In The Use of Psychological Testing for Treatment Planning and Outcome Assessment; Maruish, M.E., Ed.; Lawrence Erlbaum Associates, Inc.: Hillsdale, NJ, USA, 1994; pp. 517–549. [Google Scholar]
- Young, T.; Palta, M.; Dempsey, J.; Skatrud, J.; Weber, S.; Badr, S. The occurrence of sleep-disordered breathing among middle-aged adults. N. Engl. J. Med. 1993, 328, 1230–1235. [Google Scholar] [CrossRef] [PubMed]
- Kinsella, B.G.; Chow, S.; Kushki, A. Evaluating the usability of a wearable social skills training technology for children with autism spectrum disorder. Front. Robot. AI 2017, 4, 31. [Google Scholar] [CrossRef]
- Furfaro, H. Meet the “Bad Boy” of Autism Research. Scientific American. 2018. Available online: www.scientificamerican.com/article/meet-the-bad-boy-of-autism-research/ (accessed on 15 January 2019).
- Liu, R.; Salisbury, J.P.; Vahabzadeh, A.; Sahin, N.T. Feasibility of an autism-focused augmented reality smartglasses system for social communication and behavioral coaching. Front. Pediatr. 2017, 5, 145. [Google Scholar] [CrossRef] [PubMed]
- Sahin, N.T.; Abdus-Sabur, R.; Keshav, N.U.; Liu, R.; Salisbury, J.P.; Vahabzadeh, A. (Eds.) Case study of a digital augmented reality intervention for autism in school classrooms: Associated with improved social communication, cognition, and motivation as rated by educators and parents. Front. Educat. 2018, 3, 57. [Google Scholar] [CrossRef]
- Keshav, N.; Vahabzadeh, A.; Abdus-Sabur, R.; Huey, K.; Salisbury, J.; Liu, R.; Sahin, N. Longitudinal socio-emotional learning intervention for autism via smartglasses: Qualitative school teacher descriptions of practicality, usability, and efficacy in general and special education classroom settings. Educ. Sci. 2018, 8, 107. [Google Scholar] [CrossRef]
- Keshav, N.U.; Salisbury, J.P.; Vahabzadeh, A.; Sahin, N.T. Social communication coaching smartglasses: Well tolerated in a diverse sample of children and adults with autism. JMIR Mhealth Uhealth 2017, 5, e140. [Google Scholar] [CrossRef] [PubMed]
- Vahabzadeh, A.; Keshav, N.U.; Salisbury, J.P.; Sahin, N.T. Improvement of attention-deficit/hyperactivity disorder symptoms in school-aged children, adolescents, and young adults with autism via a digital smartglasses-based socioemotional coaching aid: Short-term, uncontrolled pilot study. JMIR Ment. Health 2018, 5, e25. [Google Scholar] [CrossRef]
- Vahabzadeh, A.; Keshav, N.U.; Abdus-Sabur, R.; Huey, K.; Liu, R.; Sahin, N.T. Improved socio-emotional and behavioral functioning in students with autism following school-based smartglasses intervention: Multi-stage feasibility and controlled efficacy study. Behav. Sci. 2018, 8, E85. [Google Scholar] [CrossRef]
- Sahin, N.T.; Keshav, N.U.; Salisbury, J.P.; Vahabzadeh, A. Safety and lack of negative effects of wearable augmented-reality social communication aid for children and adults with autism. J. Clin. Med. 2018, 7, E188. [Google Scholar] [CrossRef]
- Salisbury, J.P.; Keshav, N.U.; Sossong, A.D.; Sahin, N.T. Concussion assessment with smartglasses: Validation study of balance measurement toward a lightweight, multimodal, field-ready platform. JMIR Mhealth Uhealth 2018, 6, e15. [Google Scholar] [CrossRef]
- Sahin, N.T.; Keshav, N.U.; Salisbury, J.P.; Vahabzadeh, A. second version of google glass as a wearable socio-affective aid: Positive school desirability, high usability, and theoretical framework in a sample of children with autism. JMIR Hum. Factors 2018, 5, e1. [Google Scholar] [CrossRef] [PubMed]
- Aman, M.G.; Singh, N.N.; Stewart, A.W.; Field, C.J. The aberrant behavior checklist: a behavior rating scale for the assessment of treatment effects. Am. J. Ment. Defic. 1985, 89, 485–491. [Google Scholar]
- Rescorla, L.A.; Achenbach, T.M. The Achenbach System of Empirically Based Assessment (ASEBA) for Ages 18 to 90 Years. In The Use of Psychological Testing for Treatment Planning and Outcomes Assessment: Instruments for Adults; Maruish, M.E., Ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2004; pp. 115–152. [Google Scholar]
- Lyall, K.; Schweitzer, J.B.; Schmidt, R.J.; Hertz-Picciotto, I.; Solomon, M. Inattention and hyperactivity in association with autism spectrum disorders in the CHARGE study. Res. Autism Spectr. Disord. 2017, 35, 1–12. [Google Scholar] [CrossRef]
- King, B.H.; Wright, D.M.; Handen, B.L.; Sikich, L.; Zimmerman, A.W.; McMahon, W.; Cantwell, E.; Davanzo, P.A.; Dourish, C.T.; Dykens, E.M.; et al. Double-blind, placebo-controlled study of amantadine hydrochloride in the treatment of children with autistic disorder. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 658–665. [Google Scholar] [CrossRef]
- Arnold, L.E.; Aman, M.G.; Cook, A.M.; Witwer, A.N.; Hall, K.L.; Thompson, S.; Ramadan, Y. Atomoxetine for hyperactivity in autism spectrum disorders: placebo-controlled crossover pilot trial. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 1196–1205. [Google Scholar] [CrossRef] [PubMed]
- Bent, S.; Hendren, R.L.; Zandi, T.; Law, K.; Choi, J.E.; Widjaja, F.; Kalb, L.; Nestle, J.; Law, P. Internet-based, randomized, controlled trial of omega-3 fatty acids for hyperactivity in autism. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 658–666. [Google Scholar] [CrossRef] [PubMed]
- McCracken, J.T.; Badashova, K.K.; Posey, D.J.; Aman, M.G.; Scahill, L.; Tierney, E.; Arnold, L.E.; Vitiello, B.; Whelan, F.; Chuang, S.Z.; et al. Positive effects of methylphenidate on hyperactivity are moderated by monoaminergic gene variants in children with autism spectrum disorders. Pharmacogenomics J. 2014, 14, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Achenbach, T.M.; Rescorla, L. ASEBA School-Age Forms & Profiles; ASEBA: Burlington, VT, USA, 2001. [Google Scholar]
- Ivanova, M.Y.; Achenbach, T.M.; Rescorla, L.A.; Dumenci, L.; Almqvist, F.; Bathiche, M.; Bilenberg, N.; Bird, H.; Domuta, A.; Erol, N. Testing the teacher’s report form syndromes in 20 societies. Sch. Psychol. Rev. 2007, 36, 468–483. [Google Scholar]
- Sasser, T.R.; Kalvin, C.B.; Bierman, K.L. Developmental trajectories of clinically significant attention-deficit/hyperactivity disorder (ADHD) symptoms from grade 3 through 12 in a high-risk sample: Predictors and outcomes. J. Abnorm. Psychol. 2016, 125, 207–219. [Google Scholar] [CrossRef]
- Visser, S.N.; Danielson, M.L.; Bitsko, R.H.; Holbrook, J.R.; Kogan, M.D.; Ghandour, R.M.; Perou, R.; Blumberg, S.J. Trends in the parent-report of health care provider-diagnosed and medicated attention-deficit/hyperactivity disorder: United States, 2003–2011. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 34–46.e2. [Google Scholar] [CrossRef]
- Kessler, R.C.; Berglund, P.; Chiu, W.T.; Demler, O.; Heeringa, S.; Hiripi, E.; Jin, R.; Pennell, B.E.; Walters, E.E.; Zaslavsky, A.; et al. The US national comorbidity survey replication (NCS-R): Design and field procedures. Int. J. Methods Psychiatr. Res. 2004, 13, 69–92. [Google Scholar] [CrossRef] [PubMed]
- Onnela, J.P.; Rauch, S.L. Harnessing smartphone-based digital phenotyping to enhance behavioral and mental health. Neuropsychopharmacology 2016, 41, 1691–1696. [Google Scholar] [CrossRef] [PubMed]
- Vahabzadeh, A.; Sahin, N.; Kalali, A. Digital suicide prevention: Can technology become a game-changer? Innov. Clin. Neurosci. 2016, 13, 16–20. [Google Scholar] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Age | Gender | Ethnicity | Grade | Educatior-Rated Verbal Ability |
|---|---|---|---|---|---|
| 1 | 15 | M | White | 9th | Full |
| 2 | 15 | F | Black/African American | 9th | Minimal |
| 3 | 14 | M | Hispanic/Latino | 9th | Non-verbal |
| 4 | 15 | M | White | 9th | Full |
| 5 | 16 | M | White | 10th | Full |
| 6 | 18 | M | White | 10th | Full |
| 7 | 16 | M | White | 10th | Full |
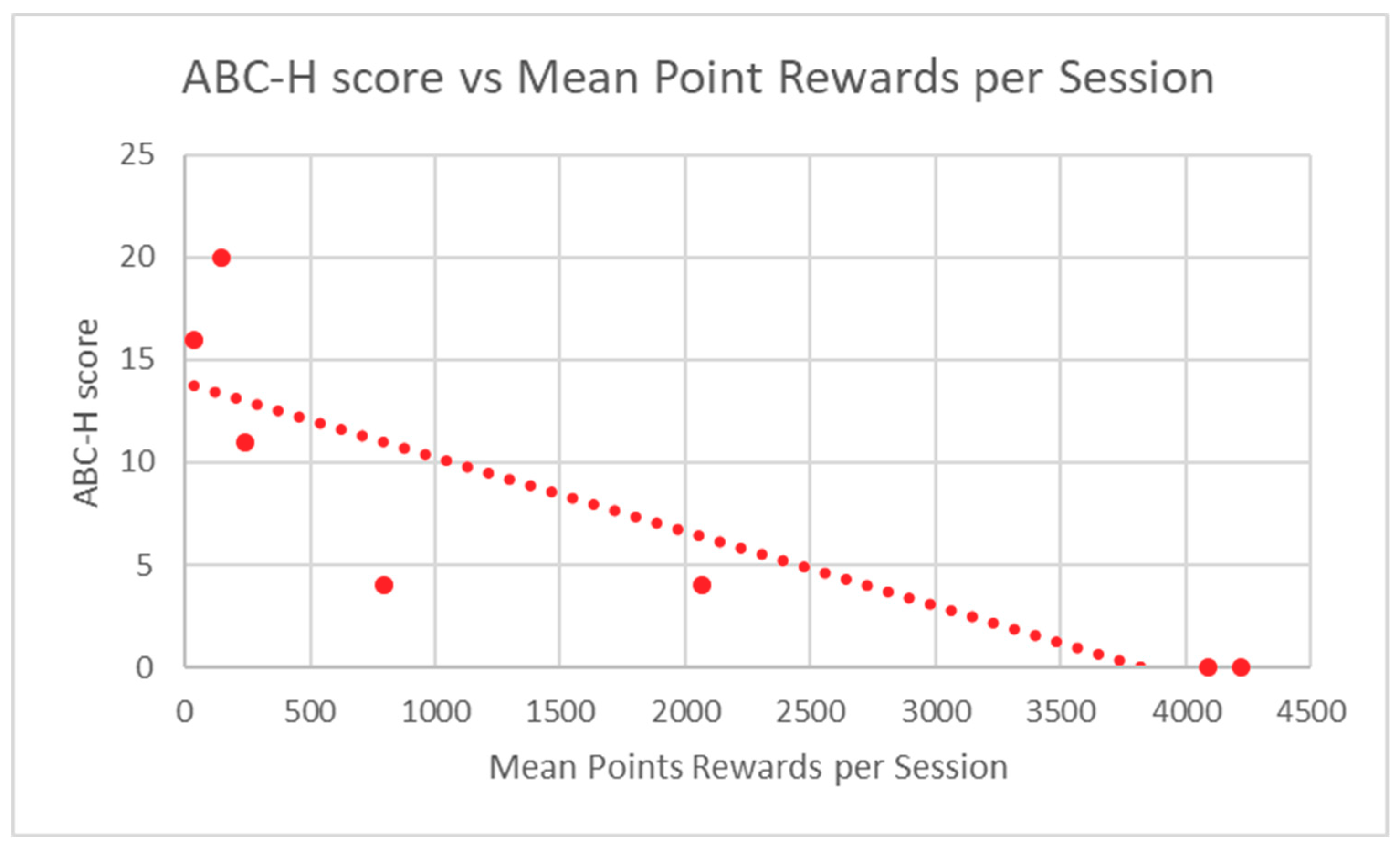
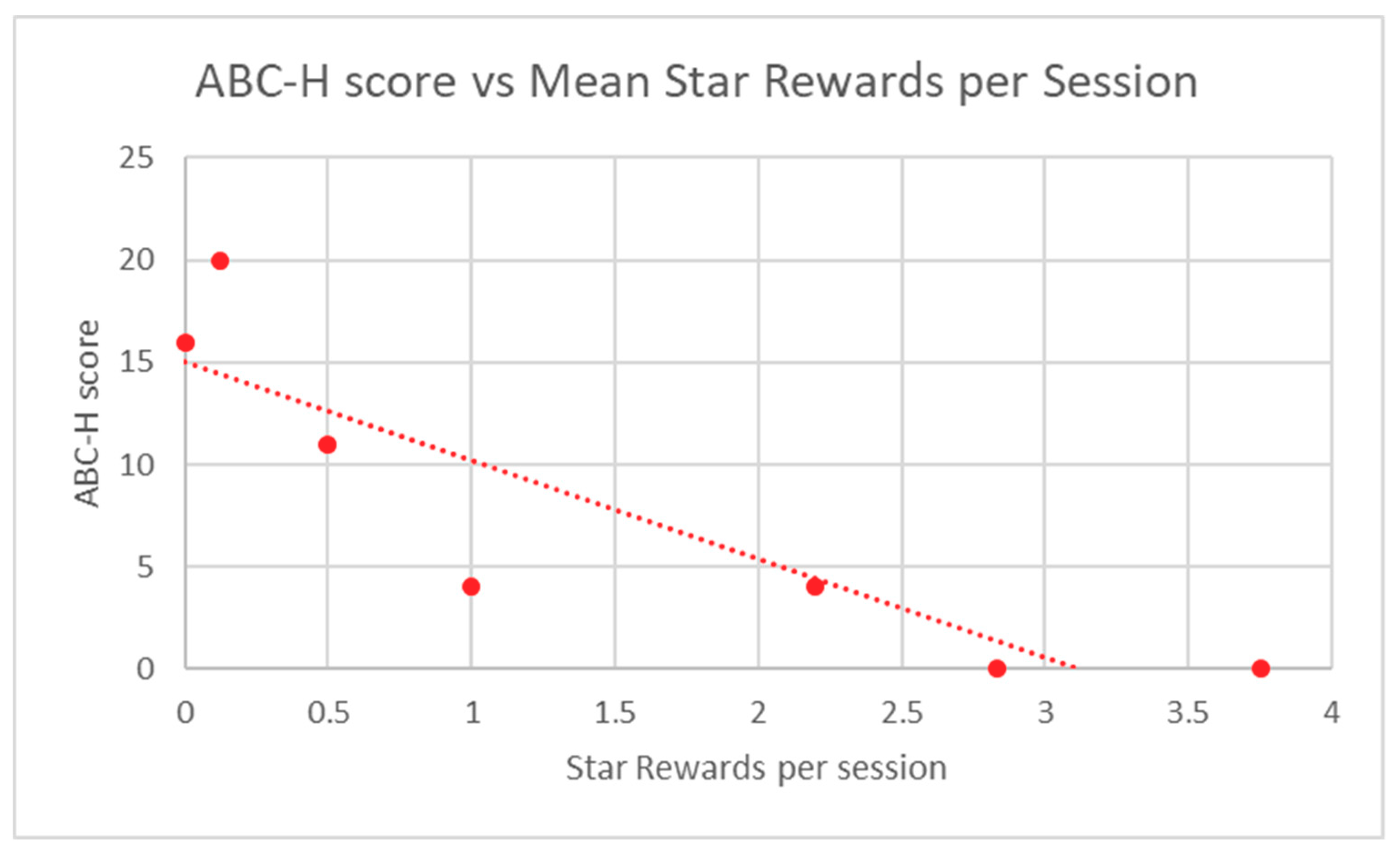
| Participant | ABC-H Score | Mean Points | Mean Stars |
|---|---|---|---|
| 1 | 20 | 143.4 | 0.125 |
| 2 | 0 | 4089.3 | 2.83 |
| 3 | 11 | 240 | 0.5 |
| 4 | 4 | 2067 | 2.2 |
| 5 | 4 | 797.6 | 1 |
| 6 | 16 | 33.5 | 0 |
| 7 | 0 | 4222 | 3.75 |
| Spearman Rho | −0.95 | −0.95 | |
| P-Value | 0.0013 ** | 0.0013 ** |
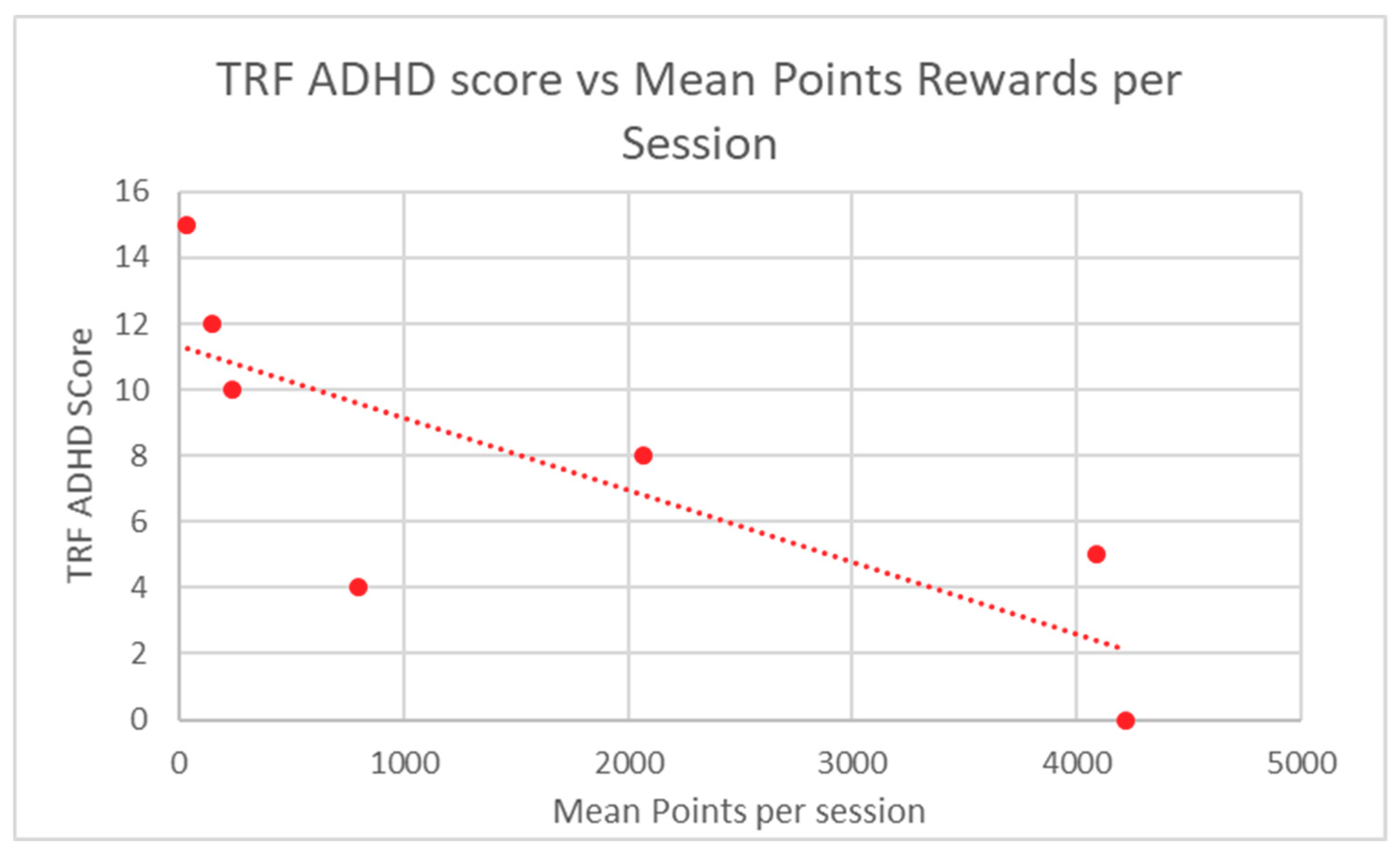
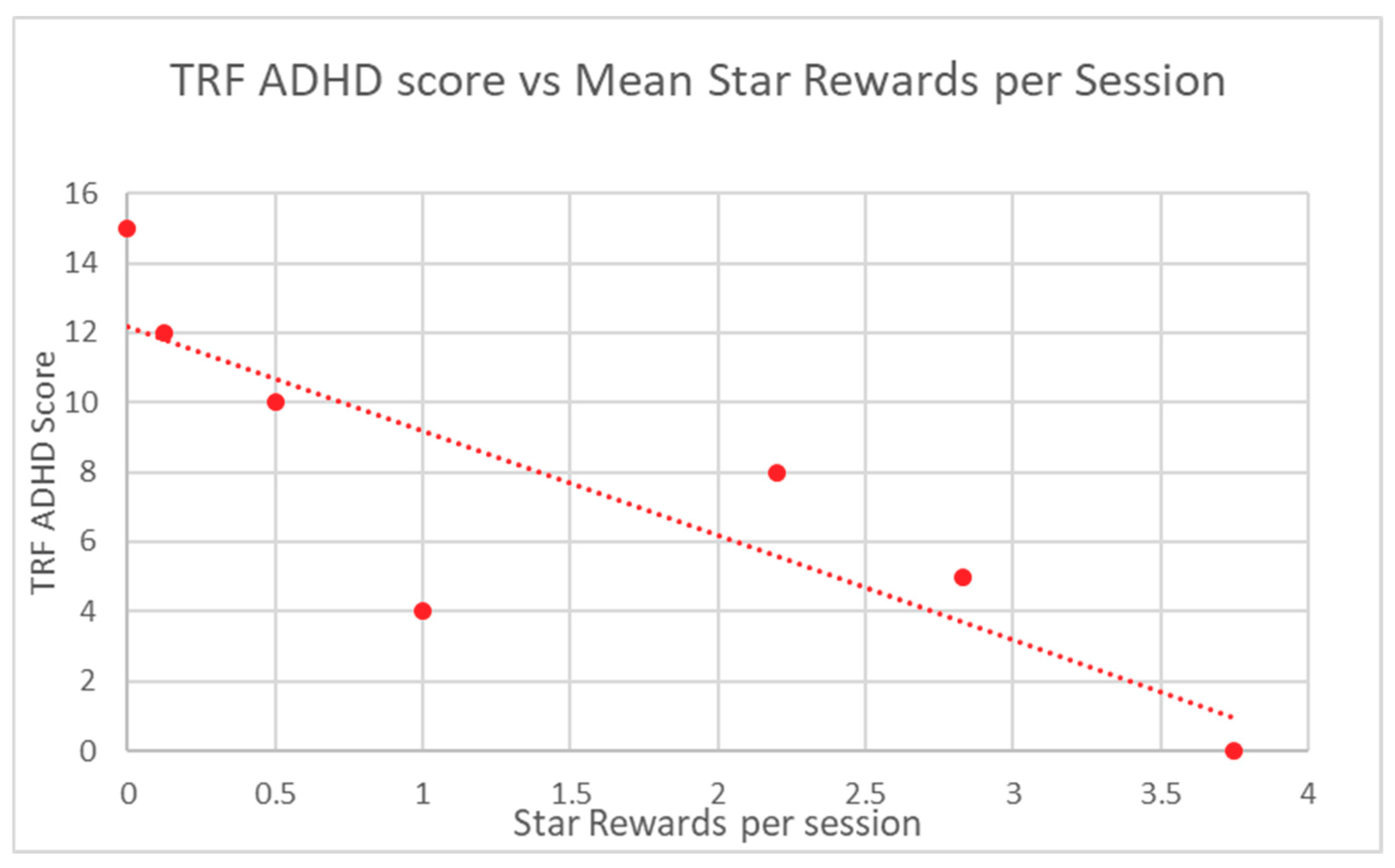
| Participant | TRF ADHD Raw Score | Mean Points | Mean Stars |
|---|---|---|---|
| 1 | 12 | 143.4 | 0.125 |
| 2 | 5 | 4089.3 | 2.83 |
| 3 | 10 | 240 | 0.5 |
| 4 | 8 | 2067 | 2.2 |
| 5 | 4 | 797.6 | 1 |
| 6 | 15 | 33.5 | 0 |
| 7 | 0 | 4222 | 3.75 |
| Spearman Rho | −0.89 | −0.89 | |
| P-Value | 0.012 * | 0.012 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keshav, N.U.; Vogt-Lowell, K.; Vahabzadeh, A.; Sahin, N.T. Digital Attention-Related Augmented-Reality Game: Significant Correlation between Student Game Performance and Validated Clinical Measures of Attention-Deficit/Hyperactivity Disorder (ADHD). Children 2019, 6, 72. https://0-doi-org.brum.beds.ac.uk/10.3390/children6060072
Keshav NU, Vogt-Lowell K, Vahabzadeh A, Sahin NT. Digital Attention-Related Augmented-Reality Game: Significant Correlation between Student Game Performance and Validated Clinical Measures of Attention-Deficit/Hyperactivity Disorder (ADHD). Children. 2019; 6(6):72. https://0-doi-org.brum.beds.ac.uk/10.3390/children6060072
Chicago/Turabian StyleKeshav, Neha U., Kevin Vogt-Lowell, Arshya Vahabzadeh, and Ned T. Sahin. 2019. "Digital Attention-Related Augmented-Reality Game: Significant Correlation between Student Game Performance and Validated Clinical Measures of Attention-Deficit/Hyperactivity Disorder (ADHD)" Children 6, no. 6: 72. https://0-doi-org.brum.beds.ac.uk/10.3390/children6060072