Influence of Workload on Primary Care Nurses’ Health and Burnout, Patients’ Safety, and Quality of Care: Integrative Review

 ,
, 
Abstract
:1. Introduction
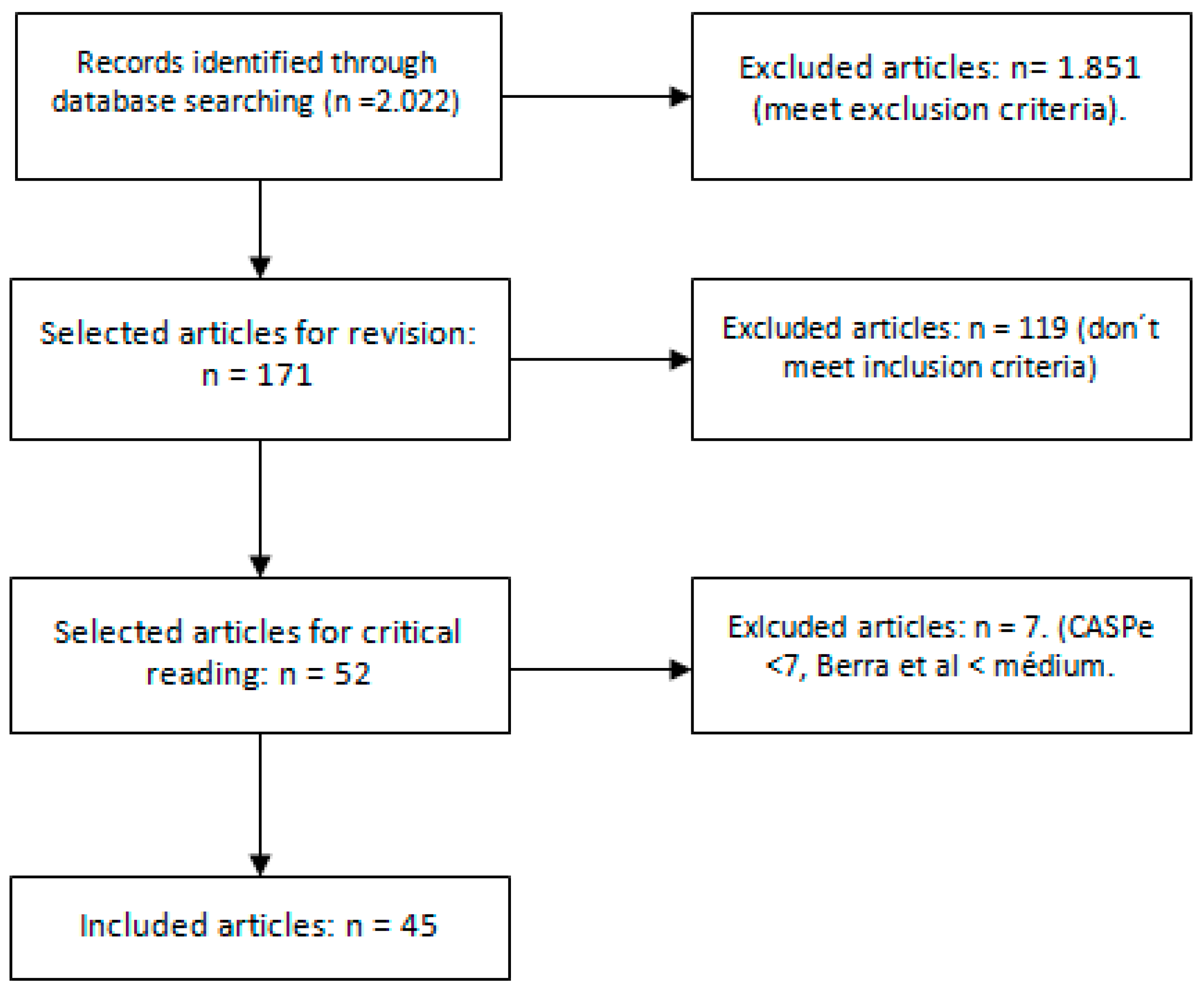
2. Materials and Methods
2.1. Search Limits
- Articles published in the last 10 years.
- In English, Spanish, or Portuguese.
- Full-text available at the time of search.
- Primary care related works that correspond to the search topic.
- Hospital care works that correspond to the subject of search: only reviews or clinical trials, prominent authors, and large samples.
- Assistance to healthy and non-healthy adults.
- Studies on physicians’ burnout where nurses are not included.
- Works in which the methodology is not described, the subjects of the study are not clear, or the inclusion criteria in the case of the reviews are not described.
2.2. Structure and Analysis
2.3. Assessment Tools
3. Results
- Methods of study.
- Instruments used in the studies.
- Interventions that improve burnout, patient safety, and quality of care.
- Relationship between workload and burnout, patient safety and quality.
3.1. Methods of Studys
3.2. Instruments Used in the Studies
3.3. Interventions That Improve Burnout, Patient Safety, and Quality of Care
3.4. Relationship between Workload and Burnout, Patient Safety and Quality
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Karanikolos, M.; Mladovsky, P.; Cylus, J.; Thomson, S.; Basu, S.; Stuckler, S.; Mackenbach, J.P.; McKee, M. Financial crisis, austerity, and health in Europe. Lancet 2013, 381, 1323–1331. [Google Scholar] [CrossRef]
- Montgomery, K.L. Health care at the crossroads, strategies for addressing the evolving nursing crisis. Nurs. Educ. Perspect. 2003, 24, 98. [Google Scholar]
- Corrêa Daubermann, D.; Pamplona Tonete, V.L. Qualidade de vida no trabalho do efermeiro da Atenção Básica à Saúde. Acta Paulista Enfermagem 2012, 25, 277–283. [Google Scholar] [CrossRef] [Green Version]
- Dall, T.M.; Chen, Y.J.; Seifert, R.F.; Maddox, P.J.; Hogan, P.F. The Economic Value of Professional Nursing. Med. Care 2009, 47, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Kane, R.L.; Shamliyan, T.A.; Mueller, C.; Duval, S.; Wilt, T.J. The Association of Registered Nurse Staffing Levels and Patient Outcomes. Med. Care 2007, 45, 1195–1204. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.H.; Clarke, S.P.; Sloane, D.M.; Sochalski, J.; Silber, J.H. Hospital nurse staffing and patient mortality, nurse burnout and job dissatisfaction. JAMA 2002, 288, 1987–1993. [Google Scholar] [CrossRef] [Green Version]
- Needleman, J.; Buerhaus, P.; Mattke, S.; Stewart, M.; Zelevinsky, K. Nurse-staffing levels and the quality of care in hospitals. N. Engl. J. Med. 2002, 346, 1715–1722. [Google Scholar] [CrossRef]
- Aiken, L.H.; Sloane, D.M.; Bruyneel, L.; Van den Heede, K.; Griffiths, P.; Busse, R.; Diomidous, M.; Kinnunen, J.; Kózka, M.; Lesaffre, E.; et al. Nurse staffing and education and hospital mortality in nine European countries: A retrospective observational study. Lancet 2014, 383, 1824–1830. [Google Scholar] [CrossRef]
- Kinnersley, P.; Anderson, E.; Parry, K.; Clemen, J.; Archard, L.; Turton, P. Randomised controlled trial of nurse practitioner versus general practitioner care for patients requesting “same day” consultations in primary care. BMJ 2000, 320, 1043–1048. [Google Scholar] [CrossRef] [Green Version]
- Scherlowski Leal David, H.M.; Chaves Mauro, M.Y.; Gomes Silva, V.; de Souza Pinheiro, M.A.; Henriques da Silva, F. Organização do trabalho de enfermagem na atenção básica: Uma questão para a saúde do trabalhador. Texto Contexto Enfermagem 2009, 18, 206–214. [Google Scholar] [CrossRef]
- Pérez-Ciordia, I.; Guillén-Grima, F.; Brugos, A.; Aguinaga Ontoso, I. Satisfacción laboral y factores de mejora en profesionales de atención primaria. Anales Sistema Sanitario Navarra 2013, 36, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Cesar-Vaz, M.R.; Soares, J.F.S.; Figueiredo, P.P.; Azambuja, E.P.; Sant’Anna, C.F.; Costa, V.Z. Percepción del riesgo en el trabajo en salud. Revista Latino-Americana Enfermagem 2009, 17, 1–8. [Google Scholar]
- Batista Gil Nunes, M.; do Carmo Cruz Robazzi, M.L.; de Souza Terra, F.; Chaves Mauro, M.Y.; Gollner Zeitoune, R.C.; de Oliveira Secco, I.A. Riscos ocupacionais dos enfermeiros atuantes na atenção à saúde da famílía. Revista Enfermagem UERJ 2010, 18, 204–209. [Google Scholar]
- Bonfim, D.; Rapone-Gaidzinski, R.; Monique Santos, F.; de Souza Gonçales, C.; Togeiro Fugulin, F.M. Identificação das intervenções de enfermagem na Atenção Primária à Saúde: Parâmetro para o dimensionamento de trabalhadores. Revista Escola Enfermagem USP 2012, 46, 1462–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gené Badia, J.; Borràs Santos, A.; Contel Segura, J.C.; Camprubí Casellas, M.D.; Cegri Lombardo, F.; Heras Tebar, A. Nursing workload predictors in Catalonia (Spain): A home care cohort study. Gaceta Sanitaria 2011, 25, 308–313. [Google Scholar] [CrossRef] [Green Version]
- Reyes Revuelta, J.F. Presentismo en Enfermería. Implicaciones en seguridad del paciente. Posibilidades de control y reducción. Enfermería Global 2014, 113, 362–373. [Google Scholar] [CrossRef] [Green Version]
- Joyce, K.; Pabayo, R.; Critchley, J.A.; Bambra, C. Flexibilización laboral y sus efectos sobre la salud y el bienestar de los empleados. Biblioteca Cochrane Plus 2010, 2. [Google Scholar] [CrossRef]
- González-Esteban, M.P.; Ballesteros-Álvaro, A.M.; Crespo-de las Heras, M.I.; Pérez-Alonso, J. Teleenfermería: Nuevo Enfoque de Intervenciones Eficaces en Atención Primaria; SACyL: Palencia, Spain, 2015. [Google Scholar]
- Echevarría-Zamanillo, M.M.; Fraile-Caviedes, C.; Diez-Sánchez, T.J.; Rodríguez-Ferrer, C.; Gamarra-Llousa, M.; Chicote-Aylagas, P.N. Organizamos de Forma Adecuada el Tiempo en Las Consultas de Enfermería en Atención Primaria. 2009. Available online: https://www.saludcastillayleon.es/investigacion/es/banco-evidencias-cuidados (accessed on 2 February 2017).
- Fernández Merino, C.; Yañez Gallardo, R. Describiendo el engagement en profesionales de enfermería de atención primaria de salud. Ciencia Enfermería 2014, 20, 131–140. [Google Scholar] [CrossRef] [Green Version]
- da Silveira Maissiar, D.; Lauter, L.; Del Pai, D.; Petri Tavares, J. Contexto de trabalho, prazer e sofrimento na atenção básica em saúde. Revista Gaúcha Enfermagem 2015, 36, 42–49. [Google Scholar]
- Guedes dos Santos, J.L.; Vierira, M.; Cardoso Assuitii, L.F.; Gomes, D.; Schlindwein Meirelles, B.H.; de Azevedo dos Santos, S.M. Risco e vulnerabilidades nas práticas nos proffisionais de saúde. Revista Gaúcha Enfermagem 2012, 33, 205–212. [Google Scholar] [CrossRef]
- Elaine Tomasi, E.; Augusto Facchini, L.; Xavier Piccini, R.; Elaine Thumé, E.; Silva da Silveira, D.; Vinholes Siqueira, F. Perfil sócio-demográfico e epidemiológico dos trabalhadores da atenção básica à saúde nas regiões Sul e Nordeste do Brasil. Cadernos Saúde Pública 2008, 24, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Elaine Tomasi, E.; Castro Sant’Anna, G.; Oppelt, A.M.; Magalhães Petrini, R.; Vianna Pereira, I.; Tomasi Sassi, B. Condições de trabalho e automedicação em profissionais da rede básica de saúde da zona urbana de Pelotas, RS. Revista Brasileira Epidemiologia 2007, 10, 66–74. [Google Scholar] [CrossRef]
- Silva Fernandes, J.; de Souza Castro Miranzi, S.; Hemiko Iwamoto, H.; dos Santos Tavares, D.M.; dos Santos, C.B. Relação dos aspectos profissionais na qualidade de vida dos enfermeiros das equipes Saúde da Família. Revista Escola Enfermagem USP 2012, 46, 404–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shihundla, R.C.; Lebese, R.T.; Maputle, M.S. Effects of increased nurses’ workload on quality documentation of patient information at selected Primary Health Care facilities in Vhembe District, Limpopo Province. Curationis 2016, 39, 1545. [Google Scholar] [CrossRef] [Green Version]
- Makeham, M.; Dovey, S.; Runciman, W.; Larizgoitia, I. Methods and Measures Used in Primary Care Patient Safety Research; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Martínez Ques, A.A.; Hueso Montoro, C.; Gálvez González, M. Fortalezas y amenazas en torno a la seguridad del paciente según la opinión de los profesionales de enfermería. Revista Latino-Americana Enfermagem 2010, 18, 339–345. [Google Scholar]
- Agra Varela, Y.; Casado Durández, P.; Palanca Sánchez, I.; García Díaz, M.J.; Álvarez González, C.; Castrodez Sanz, J.J. Estrategia de Seguridad del Paciente del Sistema Nacional de Salud. Ministerio de Sanidad; Servicios Sociales e Igualdad: Madrid, Spain, 2015. [Google Scholar]
- Fernanda Paese, G.; Marcon Dal Sasso, T. Cultura da segurança do paciente na atenção primária à saúde. Texto Contexto Enfermagem 2013, 22, 302–310. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Urquiza, J.L.; Monsalve-Reyes, C.S.; San Luis-Costas, C.; Fernández-Castillo, R.; Aguayo-Estremera, R.; Cañadas-de la Fuente, G.A. Factores de riesgo y niveles de burnout en enfermeras de atención primaria: Una revisión sistemática. Atención Primaria 2017, 47, 77–85. [Google Scholar] [CrossRef] [Green Version]
- Khamisa, N.; Peltzer, K.; Oldenburg, B. Burnout in Relation to Specific Contributing Factors and Health Outcomes among Nurses: A Systematic Review. Int. J. Environ. Res. Public Health 2013, 10, 2214–2240. [Google Scholar] [CrossRef] [Green Version]
- Szecsenyi, J.; Goetz, K.; Campbell, S.; Broge, B.; Reuschenbach, B.; Wensing, M. Is the job satisfaction of primary careteam members associated with patient satisfaction? BMJ Qual. Saf. 2011, 20, 508–514. [Google Scholar] [CrossRef]
- Liu, Y.; Aungsuroch, Y.; Yunibhand, J. Job satisfaction in nursing: A concept analysis study. Int. Nurs. Rev. 2016, 63, 84–91. [Google Scholar] [CrossRef]
- Schrader, G.; Palagi, S.; Silveira Padilha, M.A.; Tuerlinckx Noguez, P.; Buss Thofehrn, M.; Dal Pai, D. Trabalho na Unidade Básica de Saúde: Implicações para a qualidade de vida dos enfermeiros. Revista Brasileira Enfermagem 2012, 65, 222–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomás-Sábado, J.; Maynegre-Santaulària, M.; Pérez-Bartolomé, M.; Alsina-Rodríguez, M.; Quinta-Barbero, R.; Sergi Granell-Navas, S. Síndrome de burnout y riesgo suicida en enfermeras de atención primaria. Enfermería Clínica 2010, 20, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Salyers, M.P.; Bonfils, K.A.; Luther, L.; Firmin, R.L.; White, D.A.; Adams, E.L.; Rollins, A.L. The Relationship between Professional Burnout and Quality and Safety in Healthcare: A Meta-Analysis. J. Gen. Intern. Med. 2017, 32, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Palmeira Sarmento Silva, S.C.; Prado Nunes, M.A.; Rocha Santana, V.; Prado Reis, F.; Machado Neto, J.; Oliveira Lima, S. A síndrome de burnout em profissionais da Rede de Atenção Primária à Saúde de Aracaju, Brasil. Ciência Saúde Coletiva 2015, 20, 3011–3020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domínguez Fernández, J.M.; Herrera Clavero, F.; Villaverde Gutiérrez, M.C.; Padilla Segura, I.; Martínez Bagur, M.L.; Domínguez Fernández, J. Síndrome de desgaste profesional en trabajadores de atención a la salud en el área sanitaria de Ceuta. Atención Primaria 2012, 44, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rui Gomes, A.; Fernando Cruz, J.; Cabanelas, S. Estresse Ocupacional em Profissionais de Saúde: Um Estudo com Enfermeiros Portugueses. Psicologia Teoria Pesquisa 2009, 25, 307–318. [Google Scholar] [CrossRef]
- Grau, A.; Flichtentrei, D.; Suñer, R.; Prats, M.; Braga, F. Influencia de factores personales, profesionales y transnacionales en el síndrome de burnout en personal. Sanitario hispanoamericano y español. Revista Española Salud Pública 2009, 83, 215–230. [Google Scholar] [CrossRef] [Green Version]
- de Dios del Valle, R.; Franco Vidal, A. Prevalencia de burnout entre los profesionales de Atención Primaria, factores asociados y relación con la incapacidad temporal y la calidad de la prescripción. SEMERGEN 2007, 33, 58–64. [Google Scholar] [CrossRef]
- Vilà Falgueras, M.; Cruzate Muñoz, C.; Orfila Pernas, F.; Creixell Sureda, J.; González López, M.P.; Davins Miralles, J. Burnout y trabajo en equipo en los profesionales de Atención Primaria. Atención Primaria 2015, 47, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Martín Asuero, A.; Rodríguez Blanco, T.; Pujol-Ribera, E.; Berenguera, A.; Moix Queraltó, J. Evaluación de la efectividad de un programa de mindfulness en profesionales de atención primaria. Gaceta Sanitaria 2013, 27, 521–528. [Google Scholar] [CrossRef] [Green Version]
- Navarro-González, D.; Ayechu-Díaz, A.; Huarte-Labiao, I. Prevalencia del síndrome de burnout y factores asociados a dicho síndrome en los profesionales sanitarios de Atención Primaria. SEMERGEN 2015, 41, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Berra, S.; Elorza-Ricart, J.P.; Estrada, M.D.; Sánchez, E. Instrumento para la lectura crítica y la evaluación de estudios epidemiológicos transversales. Gaceta Sanitaria 2008, 22, 492–497. [Google Scholar] [CrossRef] [PubMed]
- The Joanna Briggs Institute (JBI). The Joanna Briggs Institute New Levels of Evidence; The University of Adelaide: Adelaide, Australia, 2013. [Google Scholar]
- Cañadas-De la Fuente, G.A.; Albendín-García, L.; de la Fuente, E.I.; San Luis, C.; Gómez-Urquiza, J.L.; Cañadas, G.R. Síndrome de burnout en profesionales de enfermería que realizan jornada física complementaria en servicios de cuidados críticos y urgencias. Revista Española Salud Pública 2016, 90, e1–e9. [Google Scholar]
- González Correales, R.; De la Gándara Martín, J.J. El Médico Con Burnout; IM&C, S.A.: Madrid, Spain, 2004; pp. 1–84. [Google Scholar]
- López Bueno, R.; Casajús Mallén, J.A.; Garatachea Vallejo, N. La actividad física como herramienta para reducir el absentismo laboral debido a enfermedad en trabajadores sedentarios: una revisión sistemática. Rev. Esp. Salud. Pública 2018, 92, e1–e11. [Google Scholar]
- García Candil, M.T.; Lecuona Irigoyen, A.; Iknurov Mollov, A.; Navincopa Quezada, A.M.; García López, V. Abordaje preventivo del envejecimiento saludable por los servicios de prevención de riesgos laborales. Rev. Esp. Salud. Pública 2019, 93, e1–e17. [Google Scholar]


{kind=link}
| Tool | Reference a | |
|---|---|---|
| Nursing Overload. | Qualitative interview. | [12,26,35] |
| Specific questionnaires of each study | [6,8,10,11,23] | |
| EIPST, EACT | [12] | |
| No tool used | [1,2,7] | |
| Burnout/Effects on Nursing Health. | Maslach | [38,39,40,41,42,43,44,45,47] |
| WHQOL-100 | 25 | |
| Specific questionnaires of each study | [6,10,24,36,39], [40] (3 questionnaires), [44] (3 questionnaires), [45] | |
| No tool used | [1] | |
| Patient Safety. | Qualitative interview | [12] |
| Qualitative interview | [12,13] | |
| No tool used | [2] | |
| Quality of Care. | Delphi technique | [28] |
| Specific questionnaires of each study | [6,8,30] | |
| Qualitative interview | [3] | |
| EUROPEP | [33] | |
| SAQ | [30] | |
| Specific questionnaires of each study | [6,8] | |
| No tool used | [1,2] |
| Study | %Burnout | Cut-off Points | Sample | Score * | Burnout * |
|---|---|---|---|---|---|
| [31] Gómez-Urquiza JL, Monsalve-Reyes CS et al. 2017 | Various | - | - | Important part presents high EE, high D and low P | - |
| [32] Khamisa N et al. 2013. | Various | - | - | Important part presents high EE, high D and low P | - |
| [36] Tomás-Sábado J et al. 2010 | Not stated | EE > 24 D > 9 PA > 39 | N = 146 | High EE: 23.9% Hig D: 13% Low PA: 9.6% | High EE High D Low PA |
| [38] Palmeira Sarmento Silva SC et al. 2015. | 6.7–10.8% | EE > 25 D > 8 PA < 3 4 | N = 198 | High EE: 43% High D: 17% Low PA: 32% | High EE High D Low PA |
| [39] Domínguez Fernández JM, Herrera Clavero F, et al. 2012 | 17.2% | EE > 26 D > 9 PA < 34 | N = 200 | High EE: 26% High D: 34% Low PA: 71% | High EE High D Low PA |
| [40] Rui Gomes A et al. 2009. | 15% EE | Does not specify | N = 286 | High EE: 15% High D: 4% Low PA: 1% | Does not specify |
| [41] Grau A et al. 2009 | 11% (Global)/14% Spain | Does not specify | N = 11.530 | Gives means. | High EE High D Low PA |
| [42] de Dios del Valle R, Franco Vidal A. 2007 | 36.6% | EE > 31 D > 13 PA < 30 | N = 145 | High EE: 20% High D: 11% Low PA: 57.9% | One of the three dimensions with high degree |
| [43] Vilà Falgueras M et al. 2015 | 17.2% | EE > 28 D > 9 PA < 34 | N = 879 | High EE: 38.2% High D: 23.8% Low PA: 7.7% | High EE High D or High EE High PA or High D Low PA |
| [45] Navarro-González D et al. 2015 | 39.3% 22.4% | EE > 27 D > 10 PA < 34 | N = 78 | High EE 15.7% High D: 18.5% Low PA: 47.2% | One of the three dimensions with high degree |
| [49] Cañadas-De La Fuente, G.A., et al. 2016 | Between 42.5% and 44.1% | - | N = 1021 | High EE High D High PA | High EE High D High PA |
| Reference | Workload | Burnout | Patient Safety | Quality of Care |
|---|---|---|---|---|
| [4] M. Dall, T et al. | If it decreases: (more ratio of nurses) | Does not specify | Increases | Increases |
| [5] L. Kane, R et al. | If it decreases: (more ratio of nurses) | Does not specify | Increases | Does not specify |
| [6] H Aiken, L et al. | If it increases: (less nurse ratio) | It appears | Decreases | Decreases |
| [7] Needleman, J et al. | If it decreases: (more time per patient) | Does not specify | Decreases | Increases |
| [8] H Aiken, L et al. | If it increases: (high pressure/ high work rate) | Does not specify | Decreases | Does not specify |
| [10] Scherlowski Leal David, HM et al. | If it increases: (high pressure/high work rate) | It appears | Does not specify | Does not specify |
| [11] Pérez-Ciordia, I et al. | If it increases: | It appears | Does not specify | Decreases: demoralized professional |
| [16] Reyes Revuelta, JF et al. | If it increases: | Does not specify | Decreases | Decreases |
| [17] Joyce, K et al. | If it increases: | Does not specify | Does not specify | Decreases: sick professional |
| [18] González-Esteban, MP et al. | If it decreases: telenursing | Does not specify | Increases | Increases |
| [19] Echevarría-Zamanillo, MM et al. | If it decreases: (more time per patient) | Does not specify | Does not specify | Increases: patient satisfaction |
| [21] da Silveira Maissiar, D et al. | If it increases: | Does not specify | Does not specify | Decreases: exhausted professional |
| [24] Elaine Tomasi, E et al. | If it increases: | Does not specify | Does not specify | Decreases: sick professional |
| [25] Silva Fernandes, J et al. | If it increases: | Does not specify | Does not specify | Decreases: sick profesional/not updated knowledge |
| [26] Shihundla, RC et al. | If it increases: | Does not specify | Does not specify | Decreases: worse records |
| [28] Martínez Ques, AA et al. | If it increases: | Does not specify | Does not specify | Decreases |
| [29] Agra Varela, Y et al. | If they are not organized | Does not specify | Decreases | Does not specify |
| [30] Fernanda Paese, G et al. | If it increases: | Does not specify | Decreases | Does not specify |
| [32] Khamisa, N et al. | If it increases: stress related to care pressure | It appears | Does not specify | Decreases: sick professional |
| [37] Salyers, MP et al. | If there is a high workload | It appears | Does not specify | Decreases |
| [38] Palmeira Sarmento Silva, SC et al. | If there is a high workload | It appears | Does not specify | Does not specify |
| [39] Domínguez Fernández, JM et al. | If there is a high workload | It appears | Does not specify | Does not specify |
| [40] Rui Gomes, A et al. | If more hours are worked | It appears | Does not specify | Does not specify |
| [41] Grau, A et al. | If guards are made | It appears | Does not specify | Decreases |
| [42] de Dios del Valle, R et al. | If there is a high workload | It appears | Does not specify | Decreases |
| [45] Navarro-González, D et al. | If there is a high workload | It appears | Does not specify | Does not specify |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Francisco, D.H.; Duarte-Clíments, G.; del Rosario-Melián, J.M.; Gómez-Salgado, J.; Romero-Martín, M.; Sánchez-Gómez, M.B. Influence of Workload on Primary Care Nurses’ Health and Burnout, Patients’ Safety, and Quality of Care: Integrative Review. Healthcare 2020, 8, 12. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8010012
Pérez-Francisco DH, Duarte-Clíments G, del Rosario-Melián JM, Gómez-Salgado J, Romero-Martín M, Sánchez-Gómez MB. Influence of Workload on Primary Care Nurses’ Health and Burnout, Patients’ Safety, and Quality of Care: Integrative Review. Healthcare. 2020; 8(1):12. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8010012
Chicago/Turabian StylePérez-Francisco, Darío Hilario, Gonzalo Duarte-Clíments, José María del Rosario-Melián, Juan Gómez-Salgado, Macarena Romero-Martín, and María Begoña Sánchez-Gómez. 2020. "Influence of Workload on Primary Care Nurses’ Health and Burnout, Patients’ Safety, and Quality of Care: Integrative Review" Healthcare 8, no. 1: 12. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8010012