Wellbeing Impacts of City Policies for Reducing Greenhouse Gas Emissions

 ,
,
Abstract
:
1. Introduction
2. A Conceptualization of Wellbeing Relevant to Greenhouse Gas Reduction Policies
2.1. Subjective Wellbeing Measures
2.2. Objective Wellbeing Indices
2.2.1. Sustainability and Environment
2.2.2. Socioeconomic Status
2.2.3. Social Relationships
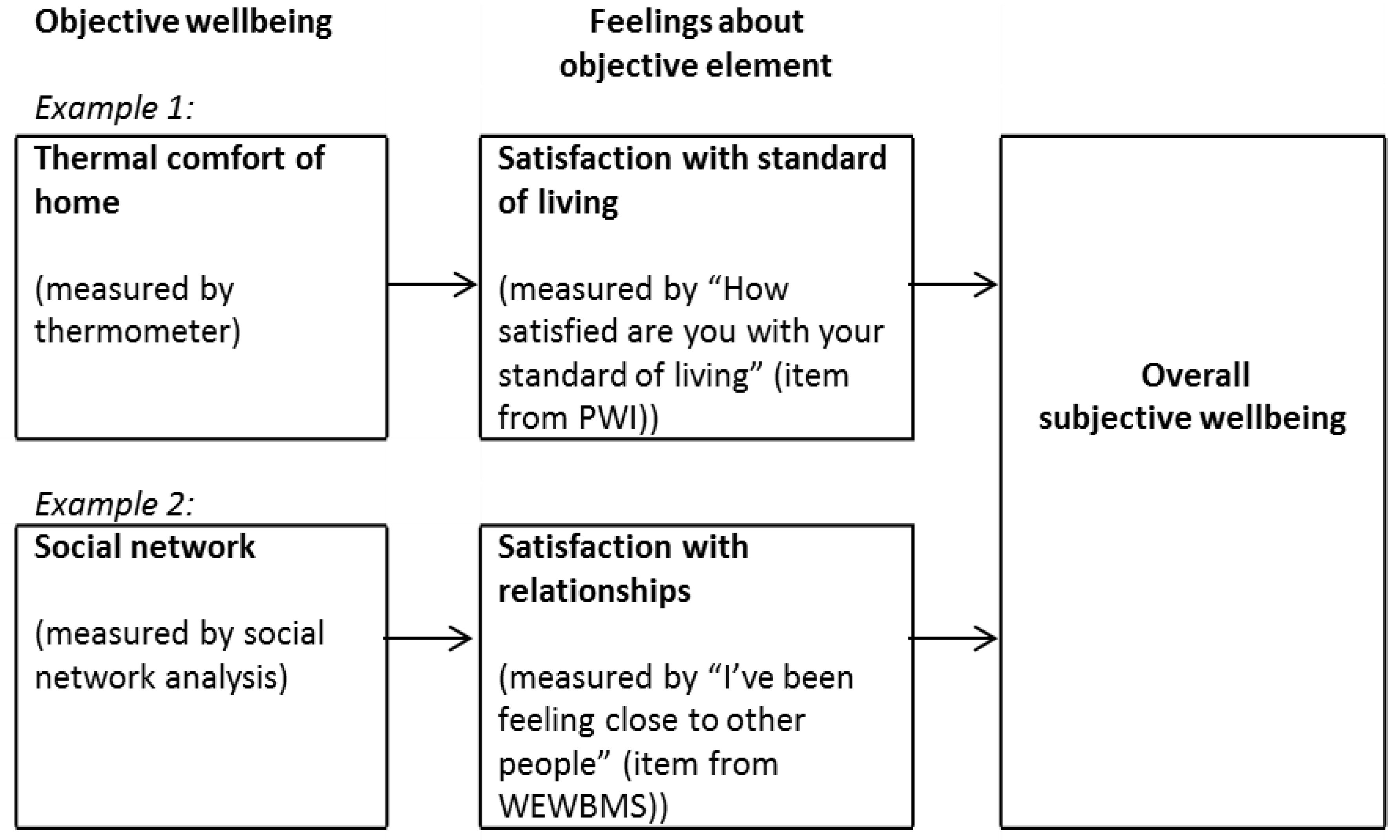
2.3. Combined Measures

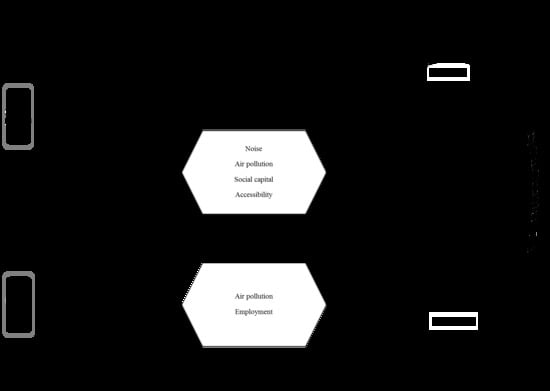
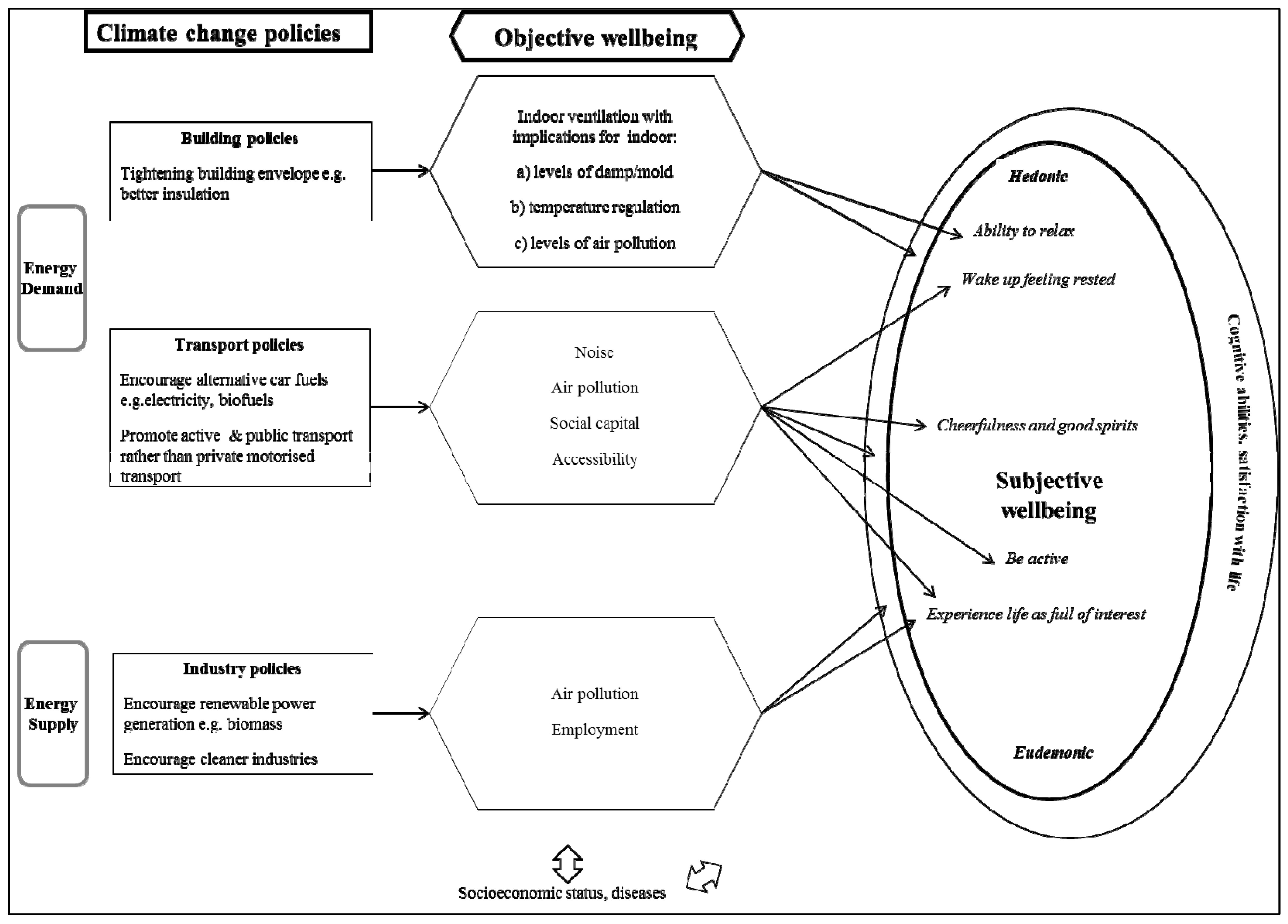
3. Development of the Conceptual Model within Policies for Reducing Greenhouse Gas Emissions
3.1. Climate Change Policies in the Conceptual Model
3.2. Objective Wellbeing Effects of GHG Reduction Policies in the Conceptual Model

3.2.1. Building Policies and Objective Wellbeing
3.2.2. Transport Policies and Objective Wellbeing
3.2.3. Industry Policies and Objective Wellbeing
3.3. Subjective Wellbeing Effects of GHG Reduction Policies in the Conceptual Model
3.3.1. Building Policies Implications Subjective Wellbeing (via Housing Conditions)
3.3.2. Transport Policy Implications for Subjective Wellbeing (via Active Transport, Social Capital and Air Pollution)
3.3.3. Industry Policy Implications for Subjective Wellbeing (via Air Pollution and Employment)
4. Quantification of the Theoretical Links between City Conditions and Wellbeing

{kind=link}
{kind=link}
{kind=link}
| Policy Area and Search Number | Search Terms * | Total Papers | Papers Providing Quantitative Assessment of Links |
|---|---|---|---|
| BUILDINGS | |||
| 1 | “((damp/mold/mould) / (thermal comfort/(cold & housing))) & (self-assessed health/mental health/ depression)” | 93 | 9 |
| 2 | “(heat stress/air conditioning) & (wellbeing/ depression/ mental health)” | NA ** | 1 |
| TRANSPORT | |||
| 1 | “(air pollution/noise) & (mental health/depression)” | 54 | 19 |
| 2 *** | “(public transport/exercise/physical activity) & (mental health/anxiety/depression)” | 568 | 1 (public transport related) |
| 3 | “(commut */transport mode/public transport/active transport) & (social capital/community/social network /volunteer */cultur *)” | 51 | 15 |
| 4 | “(accessibility/exclusion) & transport & wellbeing” | NA | 7 |
| 5 | “(green/environment/sustainable) & wellbeing” | NA | 7 |
| 6 | “(affordability/ frugality) & (wellbeing/depression/mental health)” | NA | 5 |
| INDUSTRY | |||
| 1 | “(unemployment/employment/job) & (greenhouse gas)” | 49 | 0 |
| Policies | Implications | Objective Wellbeing Aspects Explored | Subjective Wellbeing Aspects Explored | Notes on Potential for Quantification |
|---|---|---|---|---|
| BUILDINGS | ||||
| Tightening building envelope & improving insulation | Reduced air flow and reduced heat loss through building envelope | Mould and damp | Depression Mental health Self-assessed health Satisfaction with indoor air quality | Some evidence of a relationship found [98,150,151,152,153,154,155,156,157,158] but many studies are cross sectional or based in the UK (particularly the West of Scotland where there is a particular concentration of damp housing and disadvantage). Some odds ratios available. |
| Thermal comfort | Depression Mental health Residential satisfaction Self-assessed health | Most literature appears to have focused on insufficiently warm housing [152,153,154,155,156,157,158] whereas the combination of global warming and increased ventilation may lead to insufficiently cool housing [159]. Some odds ratios available. Differentiation of the effects of cold and damp is difficult. | ||
| TRANSPORT | ||||
| Tolls & Parking restrictions | Reduce private car use | Air pollution | Depression Suicide Mental Health | Fairly consistent findings [160,161,162] and one Canadian research team has provided relative risks [132,163,164,165]. However there are many differences by time of year, type of air pollution and gender. Some relative risks available. |
| Air pollution | Annoyance | ERFs developed for Europe [166,167] but direction of causality could be an issue [139]. | ||
| Noise | Annoyance Sleep disturbance Mental health Depression Satisfaction | Fairly consistent associations [98,118,121,122,168,169,170,171,172,173]. ERFs developed for annoyance and sleep disturbance [174,175]. Again direction of causality could be an issue [139]. | ||
| Accessibility | Mental health | There is a little, mostly descriptive, research on accessibility and wellbeing mostly from one Australian research team [99,176,177,178,179,180,181] which is suggestive of an association. | ||
| Biofuels | Leading a green lifestyle | Life satisfaction Happiness Social wellbeing | A consistent relationship found between leading a green lifestyle and wellbeing but studies have tended to use scales rather than dichotomous outcomes so the search did not find any ratios—generalising from the particular scales used is difficult [182,183,184,185]. | |
| Electric cars | Cars are less affordable | Affordability | Stress Depression Happiness | Studies on affordability and wellbeing are inconclusive [99,182,183,186,187,188]. Again outcomes tend to be on a continuous scale so ratios were not found. |
| Promotion of public transport | Use of public transport | Mental health | A few qualitative & descriptive studies [189] or benefits via extra walking [190] | |
| Cycle paths and foot paths | More walking and cycling | Social capital: informal social networks, community participation, trust, voting | Studies tend to be cross sectional so difficult to tell the direction of causation [101,140,141,142,143,144,145,146,147,148,149]. Odds ratios are available. | |
| Physical activity levels | Mental health Wellbeing | There is a vast literature in this area (e.g., [101,191,192,193,194,195,196,197,198,199]). | ||
| INDUSTRY | ||||
| Industries encouraged/ discouraged by city | Change in employment due to cc policies e.g., Power generation | Unemployment | Mental health | One European study has looked at climate change policies and unemployment but the results were not presented in a generalizable manner [113] and other papers are descriptive [200,201,202,203]. |
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Asikainen, A.; Savastola, M.; Parjala, E.; Kettunen, T.; Nittynen, M.; Tuomisto, J. URGENCHE WP10: Health Effect Assessment of CO2 Emission Reduction Methods in City of Kuopio. City of Kuopio and THL: 2014. Available online: http://www.kuopio.fi/c/document_library/get_file?uuid=990128c5-6c34-4320-b20e-cc1ff8f7d98f&groupId=12141 (accessed on 25 November 2014).
- Holder, M.D. Happiness in Children: Measurement, Correlates and Enhancement of Positive Subjective Well-Being; SpringerBriefs: New York, NY, USA, 2012. Available online: http://0-www-springer-com.brum.beds.ac.uk/cda/content/document/cda_downloaddocument/9789400744134-c2.pdf?SGWID=0-0-45-1327854-p174311515 (accessed on 25 November 2014).
- ONS. Measuring National Wellbeing, the Natural Environment. 2012. Available online: http://www.ons.gov.uk/ons/rel/wellbeing/measuring-national-well-being/natural-environment/art-the-natural-environment.html#tab-Introduction (accessed on 2 December 2013). [Google Scholar]
- Thomas, F.; Sabel, C.E.; Morton, K.; Hiscock, R.; Depledge, M.H. Extended impacts of climate change on health and wellbeing. Environ. Sci. Policy 2014, 44, 271–278. [Google Scholar] [CrossRef]
- Pridmore, A.; Miola, A. Public Acceptability of Sustainable Transport Measures: A Review of the Literature. Discussion Paper. International Transport Forum: 2011. Available online: http://www.internationaltransportforum.org/jtrc/DiscussionPapers/DP201120.pdf (accessed on 2 December 2013).
- WHO Regional Office for Europe. Measurement of and Target Setting for Well-Being: An Initiative by the WHO Regional Office for Europe. First Meeting of the Expert Group. Copenhagen, Denmark, 2012; Available online: http://www.euro.who.int/__data/assets/pdf_file/0009/181449/e96732.pdf?ua=1 (accessed on 25 November 2014).
- Oxfam. Oxfam Human Kind Index: A New Measure of Scotland’s Prosperity. 2012. Available online: http://policy-practice.oxfam.org.uk/~/media/Files/policy_and_practice/poverty_in_uk/HKI/HKI%20results%20April%202012.ashx (accessed on 10 April 2013).
- NEF. Happy Planet Index. Available online: http://www.happyplanetindex.org/ (accessed on 10 April 2013).
- WHO. Mental Health: A State of Well-Being. Available online: http://www.who.int/features/factfiles/mental_health/en/index.html (accessed on 17 December 2013).
- GOV.UK. PM Speech on WellbeingLondon; Cabinet Office and Prime Minister’s Office, Ed.; London, UK, 2010. Available online: https://www.gov.uk/government/speeches/pm-speech-on-wellbeing (accessed on 25 November 2014).
- ONS. Measuring National Wellbeing: A Discussion Paper on Domains and Measures. 2011. Available online: http://www.ons.gov.uk/ons/rel/wellbeing/measuring-national-well-being/discussion-paper-on-domains-and-measures/measuring-national-well-being---discussion-paper-on-domains-and-measures.html#tab-Introduction (accessed on 2 December 2013). [Google Scholar]
- Williamson, T. How deep is the distinction between a priori and a posteriori knowledge. In The a Priori in Philosophy; Casullo, A., Thurow, J., Eds.; Oxford Scholarship Online: Oxford, UK, 2013. [Google Scholar]
- Huppert, F.A.; Cooper, C.L. Wellbeing: A Complete Reference Guide, Interventions and Policies to Enhance Wellbeing; John Wiley & Sons: Chichester, UK, 2014; Volume 6. [Google Scholar]
- Taylor, D. Wellbeing and welfare: A psychosocial analysis of being well and doing well enough. J. Soc. Policy 2011, 40, 777–794. [Google Scholar] [CrossRef]
- Dodge, R.; Daly, A.P.; Huyton, J.; Sanders, L.D. The challenge of defining wellbeing. Int. J. Wellbeing 2012, 2, 222–235. [Google Scholar] [CrossRef]
- Carlisle, S.; Hanlon, P. The complex territory of well-being: contestable evidence, contentious theories and speculative conclusions. J. Public Mental Health 2007, 6, 8–13. [Google Scholar] [CrossRef]
- Carlisle, S.; Hanlon, P. “Well-being” as a focus for public health? A critique and defence. Crit. Public Health 2008. [Google Scholar] [CrossRef]
- Carlisle, S.; Henderson, G.; Hanlon, P.W. “Wellbeing”: A collateral casualty of modernity? Soc. Sci. Med. 2009, 69, 1556–1560. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Europe. Measurement of and Target Setting for Well-Being: An Initiative by the WHO Regional Office for Europe. Second Meeting of the Expert Group. Copenhagen, Denmark, 2013; Available online: http://www.euro.who.int/__data/assets/pdf_file/0009/181449/e96732.pdf?ua=1 (accessed on 25 November 2014).
- Richard, E.; Diener, E. Personality and Subjective Wellbeing. The Science of Wellbeing. 2009. Available online: http://0-link-springer-com.brum.beds.ac.uk/chapter/10.1007%2F978-90-481-2350-6_4 (accessed on 25 November 2014).
- Dolan, P.; Metcalfe, R. Measuring subjective wellbeing: Recommendations on measure for use by national governments. J. Soc. Policy 2012, 41, 409–427. [Google Scholar] [CrossRef]
- Huppert, F.A.; So, T.T. Flourishing across europe: Application of a new conceptual framework for defining well-being. Soc. Indic Res. 2013, 110, 837–861. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Deci, E.L. On happiness and human potentials: A review of research on hedonic and eudaimonic well-being. Annu. Rev. Psychol. 2001, 52, 141–166. [Google Scholar] [CrossRef] [PubMed]
- Constitution of the World Health Organisation; World Health Organization: Geneva, Switzerland, 1948. Available online: http://www.who.int/about/definition/en/print.html (accessed on 25 November 2014).
- Saylor, C. The circle of health: A health definition model. J. Holist. Nurs. 2004, 22, 97–115. [Google Scholar] [CrossRef] [PubMed]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The warwick-edinburgh mental well-being scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5. [Google Scholar] [CrossRef]
- Dreger, S.; Buck, C.; Bolte, G. Material, psychosocial and sociodemographic determinants are associated with positive mental health in Europe: A cross-sectional study. BMJ Open 2014, 4. [Google Scholar] [CrossRef] [PubMed]
- Bech, P.; Olsen, L.R.; Kjoller, M.; Rasmussen, N.K. Measuring well-being rather than the absence of distress symptoms: A comparison of the SF-36 mental health subscale and the who-five well-being scale. Int. J. Methods Psychiatr. Res. 2003, 12, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Allin, P.; Hand, D.J. The Wellbeing of Nations: Meaning, Motive and Measurement; Wiley: Hoboken, NJ, USA, 2014. [Google Scholar]
- Comprehensive Mental Health Action Plan 2013–2020; World Health Organization: Geneva, Switzerland, 2013. Available online: http://apps.who.int/gb/ebwha/pdf_files/EB132/B132_8-en.pdf (accessed on 11 April 2013).
- French, D.; Browning, C.; Kendig, H.; Luszcz, M.; Saito, Y.; Sargent-Cox, K.; Anstey, K. A simple measure with complex determinants: Investigation of the correlates of self-rated health in older men and women from three continents. BMC Public Health 2012, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkinson, S.; Joyce, K.E. The place and practices of well-being in local governance. Environ. Plann. C: Gov. Policy 2011, 29, 133–148. [Google Scholar] [CrossRef] [Green Version]
- OECD. OECD Guidelines on Measuring Subjective Well-being. OECD Publishing: 2013. Available online: http://0-dx-doi-org.brum.beds.ac.uk/10.1787/9789264191655-en (Accessed on 15th July 2014).
- E-Frame (Istat). Map on Policy Use of Progress Indicators [Draft]. Deliverable 11.1. Rondinella, T., Signore, M., Fazio, D., Calza, M.G., Righi, A., Eds.; 2014. Available online: http://www.eframeproject.eu/fileadmin/Deliverables/Deliverable11.1.pdf (accessed on 25 November 2014).
- European Comission (Eurostat). Quality of Life (QoL)—Context. Available online: http://epp.eurostat.ec.europa.eu/portal/page/portal/gdp_and_beyond/quality_of_life/context (accessed on 25 November 2014).
- Psychiactric Research Unit at the Medical Health Centre North Zealand. WHO-Five Well-being Index (WHO-5). Available online: http://www.who-5.org/ (Accessed on 2nd December 2013).
- Heun, R.; Bonsignore, M.; Barkow, K.; Jessen, F. Validity of the five-item WHO Well-Being Index (WHO-5) in an elderly population. Eur. Arch. Psychiat. Clin. Neuros. 2001, 251, 27–31. [Google Scholar] [CrossRef]
- Saipanish, R.; Lotrakul, M.; Sumrithe, S. Reliability and validity of the thai version of the who-five well-being index in primary care patients. Psychiatr. Clin. Neurosci. 2009, 63, 141–146. [Google Scholar] [CrossRef]
- Awata, S.; Bech, P.; Yoshida, S.; Hirai, M.; Suzuki, S.; Yamashita, M.; Ohara, A.; Hinokio, Y.; Matsuoka, H.; Oka, Y. Reliability and validity of the japanese version of the world health organization-five well-being index in the context of detecting depression in diabetic patients. Psychiat. Clin. Neurosciences 2007, 61, 112–119. [Google Scholar] [CrossRef]
- Hajos, T.R.; Pouwer, F.; Skovlund, S.E.; Den Oudsten, B.L.; Geelhoed-Duijvestijn, P.H.; Tack, C.J.; Snoek, F.J. Psychometric and screening properties of the WHO-5 well-being index in adult outpatients with type 1 or type 2 diabetes mellitus. Diabetic Med. 2013, 30, 63–69. [Google Scholar] [CrossRef]
- Shea, S.; Skovlund, S.E.; Bech, P.; Kalo, I.; Home, P. Routine assessment of psychological well-being in people with diabetes-validation of the WHO-5 well-being index in six countries. Diabetologia 2003, 46, A88. [Google Scholar]
- Tov, W.; Au, E. Comparing Well-Being Across Nations: Conceptual and Empirical Issues. The Oxford Handbook of Happiness. Available online: http://ink.library.smu.edu.sg/cgi/viewcontent.cgi?article=2405&context=soss_research&sei-redir=1&referer=http%3A%2F%2Fscholar.google.co.uk%2Fscholar_url%3Fhl%3Den%26q%3Dhttp%3A%2F%2Fink.library.smu.edu.sg%2Fcgi%2Fviewcontent.cgi%253Farticle%253D2405%2526context%253Dsoss_research%26sa%3DX%26scisig%3DAAGBfm3Muoasw4Wkcz0HYwo_Al_BN5xHMw%26oi%3Dscholarr%26ei%3DIeF0VNrZOOWP7AbonYDIBA%26ved%3D0CCEQgAMoADAA#search=%22http%3A%2F%2Fink.library.smu.edu.sg%2Fcgi%2Fviewcontent.cgi%3Farticle%3D2405%26context%3Dsoss_research%22 (accessed on 25 November 2014).
- Aminzadeh, K.; Denny, S.; Utter, J.; Milfont, T.L.; Ameratunga, S.; Teevale, T.; Clark, T. Neighbourhood social capital and adolescent self-reported wellbeing in New Zealand: A multilevel analysis. Soc. Sci. Med. 2013, 84, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Primack, B. The WHO-5 wellbeing index performed the best in screening for depression in primary care. Evid. Based Med. 2003, 8. [Google Scholar] [CrossRef]
- Eurofound. European quality of life surveys (EQLS). Available online: http://www.eurofound.europa.eu/surveys/eqls/index.htm (accessed on 20 May 2013).
- NHS Health Scotland; University of Warwick; University of Edinburgh. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS). Available online: http://www.experiential-researchers.org/instruments/leijssen/WEMWBS.pdf (accessed on 10 April 2013).
- Stewart-Brown, S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Weich, S. Internal construct validity of the warwick-edinburgh mental well-being scale (WEMWBS): A rasch analysis using data from the scottish health education population survey. Health Qual. Life Outcomes 2009, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C. Mental Well-Being: International Contributions to the Study of Positive Mental Health. Available online: http://books.google.co.uk/books?id=_Yv5_LMmPL8C&pg=PA148&lpg=PA148&dq=SWEMWBS&source=bl&ots=7Bc2mXMC2b&sig=LzNh_eZkKT-y4XewSW-IoESFfJQ&hl=en&sa=X&ei=1T9nUc3aAeOx0QW-y4GwAg&ved=0CGAQ6AEwCA#v=onepage&q&f=false (accessed on 12 April 2013).
- WHO Regional Office for Europe. Joint Meeting of Experts on Targets and Indicators for Health and Well-Being in Health 2020. Copenhagen, Denmark, 2013; Available online: http://www.euro.who.int/__data/assets/pdf_file/0003/186024/e96819.pdf?ua=1 (accessed on 3 November 2014).
- WHO Regional office for Europe. Health 2020 Targets, Indicators and Monitoring Framework. Regional Committee for Europe, Sixty-Third Session. Copenhagen, Denmark, 2013; Available online: http://www.euro.who.int/__data/assets/pdf_file/0008/195389/63wd08e_Health-2020-targets-3.pdf?ua=1 (accessed on 25 November 2014).
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Pavot, W.; Diener, E.; Colvin, C.R.; Sandvik, E. Further validation of the satisfaction with life scale: Evidence for the cross-method convergence of well-being measures. J. Pers. Assess. 1991, 57, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Diener, E. What is Subjective Well-Being (SWB)? Available online: http://internal.psychology.illinois.edu/~ediener/faq.html#SWB (accessed on 25 June 2014).
- Pavot, W.; Diener, E. Happiness Experienced: The Science of Subjective Well-Being. Oxford Handbook of Happiness. 2013. Available online: http://www.oxfordhandbooks.com/10.1093/oxfordhb/9780199557257.001.0001/oxfordhb-9780199557257-e-010 (accessed on 26 November 2014).
- Coughlan, S. Ofsted Plans to Scrap “satisfactory” Label for Schools. BBC News. 2012. Available online: http://www.bbc.co.uk/news/education-16579644 (accessed on 17 January 2012).
- Nieboer, A.; Lindenberg, S.; Boomsma, A.; Bruggen, A.V. Dimensions of well-being and their measurement: The SPF-IL scale. Soc. Indic Res. 2005, 73, 313–353. [Google Scholar] [CrossRef]
- ONS. Subjective Well-Being Survey User Guide: 12 Month Dataset. UK Data Archive Study Group Number 33376—Annual Population Survey: Special Licence Access. Available online: https://www.google.co.uk/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&uact=8&ved=0CCMQFjAA&url=http%3A%2F%2Fwww.ons.gov.uk%2Fons%2Fguide-method%2Fmethod-quality%2Fspecific%2Fsocial-and-welfare-methodology%2Fsubjective-wellbeing-survey-user-guide%2Fsubjective-well-being-survey-user-guide--12-month-dataset---download-version.pdf&ei=b-J0VP-mB4LW7AaZ2IH4BA&usg=AFQjCNE5xD3IVf1yg7kEACzAnzsmBdLDXA&bvm=bv.80185997,d.ZGU (accessed on 26 November 2014).
- Dillman, D.A.; Smyth, J.D.; Christian, L.M. Internet, Mail, and Mixed-Mode Surveys : The Tailored Design Method; Wiley: Hoboken, NJ, USA, 2009. [Google Scholar]
- Miller, G.A. The magical number seven plus or minus two: Some limits on our capacity for processing information. Psychol. Rev. 1956, 63, 81–97. [Google Scholar] [CrossRef] [PubMed]
- Cummins, R.A. Subjective wellbeing, homeostatically protected mood and depression: A synthesis. J. Happiness Stud. 2010, 11, 1–17. [Google Scholar] [CrossRef]
- ISOCARP. Livable Cities in a Rapidly Urbanizing World; Philips Center of Health and Well-Being: Singapore, 2010. Available online: http://www.philips-thecenter.org/Global/2011%20Livable%20Cities%20articles/Livable%20cities%20UPAT%20report%201Page%2013Jan2011.pdf (accessed on 10 April 2013).
- WHO Regional Office for Europe. Second Joint Meeting of Experts on Targets and Indicators for Health and Well-Being in Health 2020. Copenhagen, Denmark, 2014; Available online: http://www.euro.who.int/__data/assets/pdf_file/0008/253673/Meeting-Report-April-meeting-final-WEB.pdf?ua=1 (accessed on 3 November 2014).
- OECD Better Life Index. Available online: http://www.oecdbetterlifeindex.org/ (accessed on 2 May 2013).
- Gallup. Gallup Healthways Wellbeing Index. Available online: http://www.well-beingindex.com/ (accessed on 20 March 2013).
- ISTAT; CNEL. BES 2013 Report: Equitable and Sustainable Wellbeing in Italy. Available online: http://www.misuredelbenessere.it/index.php?id=48 (accessed on 4 July 2014).
- Horsman, J.; Furlong, W.; Feeny, D.; Torrance, G. The health utilities index (hui®): Concepts, measurement properties and applications. Health Qual. Life Outcomes 2003, 1. [Google Scholar] [CrossRef] [Green Version]
- Amiel, M.; Godefroy, P.; Lollivier, S. Quality of Life and Well-Being Often Go Hand in Hand. Insee Premiere. 2013. Available online: http://www.insee.fr/en/themes/document.asp?ref_id=ip1428 (accessed on 3 November 2014).
- ONS. National Wellbeing. Available online: http://www.ons.gov.uk/ons/guide-method/user-guidance/well-being/index.html (accessed on 10 April 2013).
- Boelhouwer, J. Wellbeing in the Netherlands: the SCP Life Situation Index Since 1974. The Netherlands Institute for Social Research SCP, The Hague, 2010. Available online: www.scp.nl/english/dsresource?objectid=25936&type=org (accessed on 3 June 2013).
- Ministry of the Interior Netherlands. Leefbaarometer. Available online: http://www.leefbaarometer.nl/ (accessed on 3 November 2014).
- Scott, K.; Bell, D. Trying to measure local well-being: Indicator development as a site of discursive struggles. Environ. Plann. C: Govern. Policy 2013, 31, 522–539. [Google Scholar] [CrossRef]
- Thompson, S.; Marks, N.; Jackson, T. Well-Being and Sustainable Development. Oxford Handbook of Happiness. Available online: http://www.oxfordhandbooks.com/view/10.1093/oxfordhb/9780199557257.001.0001/oxfordhb-9780199557257-e-038 (accessed on 25 November 2014).
- Burchell, B. A temporal comparison of the effects of unemployment and job insecurity on wellbeing. Sociol. Res. Online. 2011, 16, p. 9. Available online: http://0-www-socresonline-org-uk.brum.beds.ac.uk/16/1/9.html (accessed on 26 November 2014). [CrossRef]
- Dolan, P.; Peasgood, T.; Dixon, A.; Knight, M.; Phillips, D.; Tsuchiya, A.; White, M. Research on the Relationship between Well-Being and Sustainable Development; Department for Environment, Food and Rural Affairs: London, UK, 2006. [Google Scholar]
- Schneider, R.J. Theory of routine mode choice decisions: An operational framework to increase sustainable transportation. Transp. Policy 2013, 25, 128–137. [Google Scholar] [CrossRef]
- O’Campo, P.; Salmon, C.; Burke, J. Neighbourhoods and mental well-being: What are the pathways? Health Place 2009, 15, 56–68. [Google Scholar] [CrossRef] [PubMed]
- Brereton, F.; Clinch, J.; Ferreira, S. Happiness, gegraphy and the environment. Ecol. Econ. 2008, 65, 386–396. [Google Scholar] [CrossRef]
- Wong, C.K.; Wong, K.Y.; Mok, B.H. Subjective well-being, societal condition and social policy—The case study of a rich chinese society. Soc. Indic Res. 2006, 78, 405–428. [Google Scholar] [CrossRef]
- Diener, E.; Suh, E.M. Culture and Subjective Well-Being; Bradford Book Publisher: Bradford, UK, 2000. [Google Scholar]
- Atkinson, S.; Fuller, S.; Painter, J. Wellbeing and Place; Ashgate Publishing: Surrey, UK, 2012. [Google Scholar]
- Costanza, R.; Fisher, B.; Ali, S.; Beer, C.; Bond, L.; Boumans, R.; Danigelis, N.L.; Dickinson, J.; Elliott, C.; Farley, J. Quality of life: An approach integrating opportunities, human needs, and subjective well-being. Ecol. Econ. 2007, 61, 267–276. [Google Scholar] [CrossRef]
- Van Kamp, I.; Leidelmeijer, K.; Marsman, G.; de Hollander, A. Urban environmental quality and human well-being: Towards a conceptual framework and demarcation of concepts; A literature study. Landsc. Urban Plann. 2003, 65, 5–18. [Google Scholar] [CrossRef]
- Aslam, A.; Corrado, L. The geography of well-being. J. Econ. Geogr. 2012, 12, 627–649. [Google Scholar] [CrossRef]
- Pacione, M. Urban environmental quality and human wellbeing: A social geographical perspective. Landsc. Urban Plann. 2003, 65, 19–30. [Google Scholar] [CrossRef]
- Weissbecker, I. Climate change and human well-being. In Global Challenges and Opportunities; Springer: New York, NY, USA, 2011. [Google Scholar]
- Hanratty, B.; Farmer, S. Editorial: The new uk focus on well-being: What will it mean for tackling social inequalities in health? J. Public Health 2012. [Google Scholar] [CrossRef]
- Fleuret, S.; Atkinson, S. Wellbeing, health and geography: A crictical review and research agenda. N. Zeal. Geogr. 2007, 64, 106–118. [Google Scholar] [CrossRef]
- Reardon, L.; Abdallah, S. Well-being and transport: Taking stock and looking forward. Transp. Rev. 2013, 33, 634–657. [Google Scholar] [CrossRef]
- Putnam, R. Bowling alone: America’s declining social capital. J. Democr. 1995, 6, 65–78. [Google Scholar] [CrossRef]
- Zhou, Y.-C. The action logic between social capital and harmonious society construction. Acad. Explor. 2006, 4, C913. [Google Scholar]
- WHO. WHOQOL-BREF: Introduction, Administration, Scoring and Generic Version of the Assessment—Field Trial Version. Geneva, Switzerland, 1996; Available online: http://www.who.int/mental_health/media/en/76.pdf (accessed on 31 May 2013).
- Schmidt, S.; Mühlan, H.; Power, M. The EUROHIS-QOL 8-item index: Psychometric results of a cross-cultural field study. Eur. J. Public Health 2006, 16, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Van Beuningen, J.; de Jonge, T. The Personal Wellbeing Index: Construct Validity for the Netherlands. Centraal Bureau voor de Statistiek Discussion Paper 2011. Available online: http://www.cbs.nl/NR/rdonlyres/F0C01716-3E08-4A6E-AC30-9234A5EFC5FD/0/2011x1024art.pdf (accessed on 31 July 2013).
- International Wellbeing Group. Personal Wellbeing Index-Adult (PWI-A). 2013. Available online: http://www.deakin.edu.au/research/acqol/instruments/wellbeing-index/pwi-a-english.pdf (accessed on 10 October 2014).
- Parfitt, D. Reasons and Persons; Oxford University Place: Oxford, UK, 1984. [Google Scholar]
- Thomson, H.; Petticrew, M.; Douglas, M. Health impact assessment of housing improvements: Incorporating research evidence. J. Epidemiol. Commun. Health 2003, 57, 11–16. [Google Scholar] [CrossRef]
- Health in the Green Economy: Health Co-Benefits of Climate Change Mitigation in the Housing Sector; WHO: Geneva, Switzerland, 2011.
- Guite, H.; Clark, C.; Ackrill, G. The impact of the physical and urban environment on mental well-being. Public Health 2006, 120, 1117–1126. [Google Scholar] [CrossRef] [PubMed]
- Delbosc, A. The role of well-being in transport policy. Transp. Policy 2012, 23, 25–33. [Google Scholar] [CrossRef]
- International Institute for Democracy and Electoral Assistance. Voter Turnout in Western Europe Since 1945. Stockholm, 2004; Available online: http://www.idea.int/publications/voter_turnout_weurope/upload/Full_Reprot.pdf (accessed on 7 March 2013).
- Addy, C.L.; Wilson, D.K.; Kirtland, K.A.; Ainsworth, B.E.; Sharpe, P.; Kimsey, D. Associations of perceived social and physical environmental supports with physical activity and walking behavior. Amer. J. Public Health 2004, 94, 440–443. [Google Scholar] [CrossRef]
- Keniger, L.E.; Gaston, K.J.; Irvine, K.N.; Fuller, R.A. What are the benefits of interacting with nature? Int. J. Environ. Res. Public Health 2013, 10, 913–935. [Google Scholar] [CrossRef] [PubMed]
- Dur, F.; Yigitcanlar, T.; Bunker, J. A spatial-indexing model for measuring neighbourhood-level land-use and transport integration. Environ Plan B-Plan Design 2014, 41, 791–812. [Google Scholar] [CrossRef]
- Gabriel, Z.; Bowling, A. Quality of life from the perspectives of older people. Ageing Soc. 2004, 24, 675–691. [Google Scholar] [CrossRef]
- Pearce, J.; Witten, K.; Hiscock, R.; Blakely, T. Are socially disadvantaged neighbourhoods deprived of health-related community resources? Int. J. Epidemiol. 2007, 36, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S.; Halstead, J.; Gardner, K.; Carlson, C. Examining walkability and social capital as indicators of quality of life at the municipal and neighborhood scales. Appl. Res. Qual. Life 2011, 6, 201–213. [Google Scholar] [CrossRef]
- Leyden, K.M. Social capital and the built environment: The importance of walkable neighborhoods. Amer. J. Public Health 2003, 93, 1546–1551. [Google Scholar] [CrossRef]
- Ball, K.; Cleland, V.J.; Timperio, A.F.; Salmon, J.; Giles-Corti, B.; Crawford, D.A. Love thy neighbour? Associations of social capital and crime with physical activity amongst women. Soc. Sci. Med. 2010, 71, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Rotko, T.; Oglesby, L.; Künzli, N.; Carrer, P.; Nieuwenhuijsen, M.J.; Jantunen, M. Determinants of perceived air pollution annoyance and association between annoyance scores and air pollution (PM2.5, NO2) concentrations in the european expolis study. Atmos. Environ. 2002, 36, 4593–4602. [Google Scholar] [CrossRef]
- Colvile, R.N.; Hutchinson, E.J.; Mindell, J.S.; Warren, R.F. The transport sector as a source of air pollution. Atmos. Environ. 2001, 35, 1537–1565. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. WHO LARES Final Report Noise Effects and Morbidity. Copenhagen, Denmark, 2004; Available online: http://www.euro.who.int/__data/assets/pdf_file/0015/105144/WHO_Lares.pdf (accessed on 25 November 2014).
- Verheijen, E.; Jabben, J. Effect of Electric Cars on Traffic Noise and Safety. Available online: http://www.rivm.nl/bibliotheek/rapporten/680300009.pdf (accessed on 31 July 2013).
- European Trade Union Confederation (ETUC). Climate Change and Employment: Impact on Employment of Climate Change and CO2 Emission Reduction Measures in the EU-25 to 2030 Brussels, 2007. Available online: http://www.unizar.es/gobierno/consejo_social/documents/070201ClimateChang-Employment.pdf (accessed on 13 December 2011).
- UNEP. Green Jobs: Towards Decent Work in a Sustainable, Low-Carbon World; United Nations Environment Programme: Nairobi, Kenya, 2008. [Google Scholar]
- Levy, C. A 2020 Low Carbon Economy: A Knowldege Economy Programme Report. The Work Foundation: 2010. Available online: http://www.theworkfoundation.com/DownloadPublication/Report/243_lowcarbonFINAL_CORRECTED.pdf (accessed on 4 November 2014).
- Despres, C. The meaning of home: Literature review and directions for future research and theoretical development. J. Archit. Plann. Res. 1991, 8, 96–115. [Google Scholar]
- Petticrew, M.; Kearns, A.; Mason, P.; Hoy, C. The sharp study: A quantitative and qualitative evaluation of the short-term outcomes of housing and neighbourhood renewal. BMC Public Health 2009, 9. [Google Scholar] [CrossRef] [PubMed]
- Urban, J.; Máca, V. Linking traffic noise, noise annoyance and life satisfaction: A case study. Int. J. Environ. Res. Public Health 2013, 10, 1895–1915. [Google Scholar] [CrossRef] [PubMed]
- Birk, M.; Ivina, O.; von Klot, S.; Babisch, W.; Heinrich, J. Road traffic noise: Self-reported noise annoyance versus gis modelled road traffic noise exposure. J. Environ. Monit. 2011, 13, 3237–3245. [Google Scholar] [CrossRef] [PubMed]
- Fyhri, A.; Klaeboe, R. Road traffic noise, sensitivity, annoyance and self-reported health—A structural equation model exercise. Environ. Int. 2009, 35, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Kawada, T.; Yosiaki, S.; Yasuo, K.; Suzuki, S. Population study on the prevalence of insomnia and insomnia-related factors among japanese women. Sleep Med. 2003, 4, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Li, H.-J.; Yu, W.-B.; Lu, J.-Q.; Zeng, L.; Li, N.; Zhao, Y.-M. Investigation of road-traffic noise and annoyance in Beijing: A cross-sectional study of 4th ring road. Arch. Environ. Occup. Health 2008, 63, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Miedema, H.M.; Oudshoorn, C.G. Annoyance from transportation noise: Relationships with exposure metrics DNL and DENL and their confidence intervals. Environ. Health Persp. 2001, 109, 409–416. [Google Scholar] [CrossRef]
- Ising, H.; Kruppa, B. Health effects caused by noise: Evidence in the literature form the past 25 years. Noise Health 2004, 6, 5–13. [Google Scholar] [PubMed]
- Sallis, J.F.; Glanz, K. The role of built environments in physical activity, eating, and obesity in childhood. Future Child 2006, 16, 89–108. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, E.A.; Reyes, L. Continuity and change in relationships with neighbors: Implications for psychological well-being in middle and later life. J. Gerontol. Ser. B-Psychol. Sci. 2014. [Google Scholar] [CrossRef]
- Becchetti, L.; Ricca, E.G.; Pelloni, A. The relationship between social leisure and life satisfaction: Causality and policy implications. Soc. Indic Res. 2012, 108, 453–490. [Google Scholar] [CrossRef]
- Rodríguez-Pose, A.; von Berlepsch, V. Social capital and individual happiness in Europe. J. Happiness Stud. 2014, 15, 357–386. [Google Scholar] [CrossRef]
- Shenassa, E.; Liebhaber, A.; Ezeamama, A. Perceived safety of area of residence and exercise: A pan-european study. Amer. J. Epidemiol. 2006, 163, 1012–1017. [Google Scholar] [CrossRef]
- Welsch, H. Preference over prosperity and pollution: Environmental valuation based on happiness surveys. Kyklos 2002, 55, 473–494. [Google Scholar] [CrossRef]
- Rehdanz, K.; Maddison, D. Local environmental quality and life-satisfaction in germany. Ecol. Econ. 2008, 64, 787–797. [Google Scholar] [CrossRef]
- Szyszkowicz, M.; Rowe, B.H.; Colman, I. Air pollution and daily emergency department visits for depression. Int. J. Occup. Med. Environ. Health 2009, 22, 355–362. [Google Scholar] [PubMed]
- Clougherty, J.E.; Kubzansky, L.D. A framework for examining social stress and susceptibility to air pollution in respiratory health. Ciência Saúde Coletiva 2010, 15, 2059–2074. [Google Scholar] [CrossRef] [PubMed]
- Downey, L.; Van Willigen, M. Environmental stressors: The mental health impacts of living near industrial activity. J. Health Soc. Behav. 2005, 46, 289–305. [Google Scholar] [CrossRef] [PubMed]
- Pascal, M.; Pascal, L.; Bidondo, M.-L.; Cochet, A.; Sarter, H.; Stempfelet, M.; Wagner, V. A review of the epidemiological methods used to investigate the health impacts of air pollution around major industrial areas. J. Environ. Public Health 2013. [Google Scholar] [CrossRef]
- McManus, S.; Mowlam, A.; Dorsett, D.; Stansfeld, S.; Clark, C.; Brown, V.; Wollny, I.; Rahim, N.; Morrell, G.; Graham, J.; et al. Mental Health in Context: The National Study of Worksearch and Wellbeing; UK Deparatment for Work and Pensions: UK, 2012. Available online: http://research.dwp.gov.uk/asd/asd5/rports2011-2012/rrep810.pdf (accessed on 11 April 2013).
- Weich, S.; Brugha, T.; King, M.; McManus, S.; Bebbington, P.; Jenkins, R.; Cooper, C.; McBride, O.; Stewart-Brown, S. Mental well-being and mental illness: Findings from the adult psychiatric morbidity survey for england 2007. Brit. J. Psychiat. 2011, 199, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Gili, M.; Roca, M.; Basu, S.; McKee, M.; Stuckler, D. The mental health risks of economic crisis in Spain: Evidence from primary care centres, 2006 and 2010. Eur. J. Public Health 2013, 23, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Persson, R.; Bjork, J.; Ardo, J.; Albin, M.; Jakobsson, K. Trait anxiety and modeled exposure as determinants of self-reported annoyance to sound, air pollution and other environmental factors in the home. Int. Arch. Occup. Environ. Health 2007, 81, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Lindstrom, M. Social capital, desire to increase physical activity and leisure-time physical activity: A population-based study. Public Health 2011, 125, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Renalds, A.; Smith, T.H.; Hale, P.J. A systematic review of built environment and health. Fam. Commun. Health 2010, 33, 68–78. [Google Scholar] [CrossRef]
- Nguyen, D. Evidence of the impacts of urban sprawl on social capital. Environ. Plan. B-Plan. Des. 2010, 37, 610–627. [Google Scholar] [CrossRef]
- Hopkins, D.; Williamson, T. Inactive by design? Neighborhood design and political participation. Polit. Behav. 2012, 34, 79–101. [Google Scholar] [CrossRef]
- Richard, L.; Gauvin, L.; Gosselin, C.; Laforest, S. Staying connected: Neighbourhood correlates of social participation among older adults living in an urban environment in Montreal, Quebec. Health Promot. Int. 2009, 24, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.; Frank, L.D.; Giles-Corti, B. Sense of community and its relationship with walking and neighborhood design. Soc. Sci. Med. 2010, 70, 1381–1390. [Google Scholar] [CrossRef] [PubMed]
- Wilkerson, A.; Carlson, N.E.; Yen, I.H.; Michael, Y.L. Neighborhood physical features and relationships with neighbors: Does positive physical environment increase neighborliness? Environ. Behav. 2012, 44, 595–615. [Google Scholar] [CrossRef]
- Toit, L.D.; Cerin, E.; Leslie, E.; Owen, N. Does walking in the neighbourhood enhance local sociability? Urban Studies 2007, 44, 1677–1695. [Google Scholar] [CrossRef]
- Poortinga, W. Perceptions of the environment, physical activity, and obesity. Soc. Sci. Med. 2006, 63, 2835–2846. [Google Scholar] [CrossRef] [PubMed]
- Hanibuchi, T.; Kondo, K.; Nakaya, T.; Shirai, K.; Hirai, H.; Kawachi, I. Does walkable mean sociable? Neighborhood determinants of social capital among older adults in Japan. Health Place 2012, 18, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Shenassa, E.D.; Daskalakis, C.; Liebhaber, A.; Braubach, M.; Brown, M. Dampness and mold in the home and depression: An examination of mold-related illness and perceived control of one’s home as possible depression pathways. Amer. J. Public Health 2007, 97, 1893–1899. [Google Scholar] [CrossRef]
- Packer, C.N.; Stewartbrown, S.; Fowle, S.E. Damp housing and adult health-results from a life-style study in Worcester, England. J. Epidemiol. Commun. Health 1994, 48, 555–559. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. Large Analysis and Review of European Housing and Health Status (LARES): Preliminary Overview. Copenhagen, Denmark, 2007; Available online: http://www.euro.who.int/en/health-topics/environment-and-health/Housing-and-health/activities/the-large-analysis-and-review-of-european-housing-and-health-status-lares-project (accessed on 25 November 2014).
- Evans, J.; Hyndman, S.; Stewart-Brown, S.; Smith, D.; Petersen, S. An epidemiological study of the relative importance of damp housing in relation to adult health. J. Epidemiol. Commun. Health 2000, 54, 677–686. [Google Scholar] [CrossRef]
- Hopton, J.L.; Hunt, S.M. Housing conditions and mental health in a disadvantaged area in scotland. J. Epidemiol. Commun. Health 1996, 50, 56–61. [Google Scholar] [CrossRef]
- Blackman, T.; Harvey, J.; Lawrence, M.; Simon, A. Neighbourhood renewal and health: Evidence from a local case study. Health Place 2001, 7, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Hopton, J.; Hunt, S. The health effects of improvements to housing: A longitudinal study. Hous. Stud. 1996, 11, 271–286. [Google Scholar] [CrossRef]
- Hyndman, S.J. Housing dampness and health amongst british bengalis in east London. Soc. Sci. Med. 1990, 30, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Butler, S.; Williams, M.; Tukuitonga, C.; Paterson, J. Problems with damp and cold housing among pacific families in New Zealand. N. Z. Med. J. 2003, 116, 1177. [Google Scholar]
- Tawatsupa, B.; Yiengprugsawan, V.; Kjellstrom, T.; Seubsman, S.-A.; Sleigh, A.; The Thai Cohort Study Team. Heat stress, health and well-being: Findings from a large national cohort of Thai adults. BMJ Open 2012, 2. [Google Scholar] [CrossRef] [PubMed]
- Welsch, H. Environment and happiness: Valuation of air pollution using life satisfaction data. Ecol. Econ. 2006, 58, 801–813. [Google Scholar] [CrossRef]
- Menz, T. Do people habituate to air pollution? Evidence from international life satisfaction data. Ecol. Econ. 2011, 71, 211–219. [Google Scholar] [CrossRef]
- Lim, Y.-H.; Kim, H.; Kim, J.H.; Bae, S.; Park, H.Y.; Hong, Y.-C. Air pollution and symptoms of depression in elderly adults. Environ. Health Persp. 2012, 120, 1023–1028. [Google Scholar] [CrossRef]
- Szyszkowicz, M.; Willey, J.B.; Grafstein, E.; Rowe, B.H.; Colman, I. Air pollution and emergency department visits for suicide attempts in Vancouver, Canada. Environ. Health Insights 2010, 4, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Szyszkowicz, M. Air pollution and emergency department visits for depression in edmonton, Canada. Int. J. Occup. Med. Environ. Health 2007, 20, 241–245. [Google Scholar] [PubMed]
- Szyszkowicz, M.; Tremblay, N. Case-crossover design: Air pollution and health outcomes. Int. J. Occup. Med. Environ. Health 2011, 24, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Amundsen, A.H.; Klaeboe, R.; Fyhri, A. Annoyance from vehicular air pollution: Exposure-response relationships for Norway. Atmos. Environ. 2008, 42, 7679–7688. [Google Scholar] [CrossRef]
- Klaeboe, R.; Amundsen, A.H.; Fyhri, A. Annoyance from vehicular air pollution: A comparison of european exposure-response relationships. Atmos. Environ. 2008, 42, 7689–7694. [Google Scholar] [CrossRef]
- Paunovic, K.; Jakovljevic, B.; Belojevic, G. Predictors of noise annoyance in noisy and quiet urban streets. Sci. Total Environ. 2009, 407, 3707–3711. [Google Scholar] [CrossRef] [PubMed]
- Kryter, K.D. Acoustical model and theory for predicting effects of environmental noise on people. J. Acoust. Soc. Amer. 2009, 125, 3707–3721. [Google Scholar] [CrossRef]
- Schram-Bijkerk, D.; van Kempen, E.; Knol, A.B.; Kruize, H.; Staatsen, B.; van Kamp, I. Quantitative health impact assessment of transport policies: Two simulations related to speed limit reduction and traffic re-allocation in the Netherlands. Occup. Environ. Med. 2009, 66, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Osada, Y.; Kawaguchi, T.; Hoshiyama, Y.; Yoshida, K.; Yamamoto, K. Effects of road traffic noise on inhabitants of Tokyo. J. Sound Vibr. 1997, 205, 517–522. [Google Scholar] [CrossRef]
- Schreckenberg, D.; Griefahn, B.; Meis, M. The associations between noise sensitivity, reported physical and mental health, perceived environmental quality, and noise annoyance. Noise Health 2010, 12, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Dratva, J.; Zemp, E.; Dietrich, D.F.; Bridevaux, P.-O.; Rochat, T.; Schindler, C.; Gerbase, M.W. Impact of road traffic noise annoyance on health-related quality of life: Results from a population-based study. Qual. Life Res. 2010, 19, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Miedema, H.M.E.; Vos, H. Exposure-response relationships for transportation noise. J. Acoust. Soc. Amer. 1998, 104, 3432–3445. [Google Scholar] [CrossRef]
- Miedema, H.M.; Vos, H. Associations between self-reported sleep disturbance and environmental noise based on reanalyses of pooled data from 24 studies. Behav. Sleep Med. 2007, 5, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Stanley, J.K.; Hensher, D.A.; Stanley, J.R.; Vella-Brodrick, D. Mobility, social exclusion and well-being: Exploring the links. Transp. Res. Part A-Policy Pract. 2011, 45, 789–801. [Google Scholar] [CrossRef]
- Johnson, V.; Currie, G.; Stanley, J. Measures of disadvantage: Is car ownership a good indicator? Soc. Indicat. Res. 2010, 97, 439–450. [Google Scholar] [CrossRef]
- Hurni, A. Marginalised groups in western sydney: The experience of sole parents and unemployed young people. In No Way to Go: Transport and Social Disadvantage in Australian Communities; Currie, G., Stanley, J., Stanley, J., Eds.; Monash University ePress: Melbourne, Australia, 2007. [Google Scholar]
- Delbosc, A.; Currie, G. Exploring the relative influences of transport disadvantage and social exclusion on well-being. Transp. Policy 2011, 18, 555–562. [Google Scholar] [CrossRef]
- Currie, G.; Delbosc, A. Modelling the social and psychological impacts of transport disadvantage. Transportation 2010, 37, 953–966. [Google Scholar] [CrossRef]
- Olsson, L.E.; Jakobsson, C.; Gamble, A.; Garling, T. The road to happiness? Car use and subjective well-being. Int. J. Psychol. 2008, 43, 469–469. [Google Scholar]
- Corral-Verdugo, V.; Mireles-Acosta, J.; Tapia-Fonllem, C.; Fraijo-Sing, B. Happiness as correlate of sustainable behavior: A study of pro-ecological, frugal, equitable and altruistic actions that promote subjective wellbeing. Hum. Ecol. Rev. 2011, 18, 95–104. [Google Scholar]
- Kasser, T.; Sheldon, K. What makes for a merry Christmas? J. Happiness Stud. 2002, 3, 313–329. [Google Scholar] [CrossRef]
- Mellan, M. Green and Happy? The Relationship between Personal Well-Being and Environmental Knowledge, Attitudes and Behaviours; Imperial College: London, UK, 2006. [Google Scholar]
- Brown, K.W.; Kasser, T. Are psychological and ecological well-being compatible? The role of values, mindfulness, and lifestyle. Soc. Indic Res. 2005, 74, 349–368. [Google Scholar] [CrossRef]
- Bentley, R.; Baker, E.; Mason, K. Cumulative exposure to poor housing affordability and its association with mental health in men and women. J. Epidemiol. Community Health 2012, 66, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Bentley, R.; Baker, E.; Mason, K.; Subramanian, S.V.; Kavanagh, A.M. Association between housing affordability and mental health: A longitudinal analysis of a nationally representative household survey in australia reply. Amer. J. Epidemiol. 2011, 174, 753–760. [Google Scholar] [CrossRef]
- Harkness, J.; Newman, S. Geographic differences in housing prices and the wellbeing of children and parents. J. Urban Affair. 2009, 31, 123–146. [Google Scholar] [CrossRef]
- Jones, A.; Steinbach, R.; Roberts, H.; Goodman, A.; Green, J. Rethinking passive transport: Bus fare exemptions and young people’s wellbeing. Health Place 2012, 18, 605–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Besser, L.M.; Dannenberg, A.L. Walking to public transit: Steps to help meet physical activity recommendations. Amer. J. Prev. Med. 2005, 29, 273–280. [Google Scholar] [CrossRef]
- Gatersleben, B.; Uzzell, D. Affective appraisals of the daily commute-comparing perceptions of drivers, cyclists, walkers, and users of public transport. Environ. Behav. 2007, 39, 416–431. [Google Scholar] [CrossRef]
- Wen, L.M.; Rissel, C. Inverse associations between cycling to work, public transport, and overweight and obesity: Findings from a population based study in Australia. Prev. Med. 2008, 46, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Abu-Omar, K. Mental health and physical activity in the European Union. Sozial-Und Praventivmedizin 2004, 49, 301–309. [Google Scholar] [PubMed]
- Culpepper, D.; Jevas, S.; Perkins, H. Predicting symptoms of depression based on self-reported levels of physical activity. Res. Quart. Exercise Sport 2004, 75, 89–90. [Google Scholar]
- Daley, A. Exercise and depression: A review of reviews. J. Clin. Psychol. Med. Set. 2008, 15, 140–147. [Google Scholar] [CrossRef]
- Holley, J. Physical activity and mental health: Reflections from research and implications for practice. Ment. Health Today 2011, 2, 30–33. [Google Scholar]
- Kirby, S. The positive effect of exercise as a therapy for clinical depression. Nurs. Times 2005, 101, 28–29. [Google Scholar]
- Deslandes, A.; Moraes, H.; Ferreira, C.; Veiga, H.; Silveira, H.; Mouta, R.; Pompeu, F.A.; Coutinho, E.S.; Laks, J. Exercise and mental health: Many reasons to move. Neuropsychobiology 2009, 59, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Rissel, C.E. Active travel: A climate change mitigation strategy with co-benefits for health. N. S. W. Public Health Bull. 2009, 20, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Paul, K.I.; Moser, K. Unemployment impairs mental health: Meta-analyses. J. Vocat. Behav. 2009, 74, 264–282. [Google Scholar] [CrossRef]
- Neuwahl, F.; Loeschel, A.; Mongelli, I.; Delgado, L. Employment impacts of eu biofuels policy: Combining bottom-up technology information and sectoral market simulations in an input-output framework. Ecol. Econ. 2008, 68, 447–460. [Google Scholar] [CrossRef]
- Babiker, M.H.; Eckaus, R.S. Unemployment effects of climate policy. Environ. Sci. Policy 2007, 10, 600–609. [Google Scholar] [CrossRef]
- Sonneborn, C. Generating jobs-sustainable energy initiatives deliver more jobs and lower greenhouse gas emissions. Altern. J. 2000, 26, 30–31. [Google Scholar]
- Sarigiannis, D.A.; Karakitsios, S.P.; Kermenidou, M.; Nikolaki, S.; Zikopoulos, D.; Semelidis, S.; Papagiannakis, A.; Tzimou, R. Total exposure to airborne particulate matter in cities: The effect of biomass combustion. Sci. Total Environ. 2014, 493, 795–805. [Google Scholar] [CrossRef] [PubMed]
- Keuken, M.; Jonkers, S.; Verhagen, H.; Perez, L.; Trüeb, S.; Okkerse, W.-J.; Liu, J.; Pan, X.; Zheng, L.; Wang, H. Impact on air quality of measures to reduce CO2 emissions from road traffic in Basel, Rotterdam, Xi’an and Suzhou. Atmosp. Environ. 2014. [Google Scholar] [CrossRef]
- Global Footprint Network. Ecological Footprint Atlas. 2010. Available online: http://www.footprintnetwork.org/images/uploads/Ecological_Footprint_Atlas_2010.pdf (accessed on 25 November 2014).
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hiscock, R.; Mudu, P.; Braubach, M.; Martuzzi, M.; Perez, L.; Sabel, C. Wellbeing Impacts of City Policies for Reducing Greenhouse Gas Emissions. Int. J. Environ. Res. Public Health 2014, 11, 12312-12345. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph111212312
Hiscock R, Mudu P, Braubach M, Martuzzi M, Perez L, Sabel C. Wellbeing Impacts of City Policies for Reducing Greenhouse Gas Emissions. International Journal of Environmental Research and Public Health. 2014; 11(12):12312-12345. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph111212312
Chicago/Turabian StyleHiscock, Rosemary, Pierpaolo Mudu, Matthias Braubach, Marco Martuzzi, Laura Perez, and Clive Sabel. 2014. "Wellbeing Impacts of City Policies for Reducing Greenhouse Gas Emissions" International Journal of Environmental Research and Public Health 11, no. 12: 12312-12345. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph111212312