
Development of an RF-EMF Exposure Surrogate for Epidemiologic Research

Abstract
:1. Introduction
2. Methods
2.1. Hermes Study
- Duration of calls made and received with their own and other mobile phones (GSM and UMTS mobile phone calls);
- Proportion of calls with the mobile phone using a headset (GSM and UMTS mobile phone calls);
- Duration of mobile phone use for data traffic (mobile phone data traffic and mobile phone data traffic WLAN);
- Duration of carrying the mobile phone close to the body (mobile phone close to body);
- Duration of calls made and received with a DECT phone at home (DECT phone calls);
- Duration of computer, laptop and tablet use and WLAN connection of the corresponding devices (computer, laptop and tablet use with WLAN).
2.2. Personal Measurements in the Framework of the Hermes Study

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency Band | Frequency Range (MHz) | Quantitation Limit (V/m) | Reporting Limit (V/m) | |
|---|---|---|---|---|
| Expom 1 and Expom 3 | Expom 1 | Expom 3 | Expom 1 and Expom 3 | |
| TV | 470–790 | 0.010 | 0.005 | 0.0025 |
| Uplink 900 * | 880–915 | 0.015 | 0.005 | 0.0025 |
| Downlink 900 * | 925–960 | 0.015 | 0.005 | 0.0025 |
| Uplink 1800 * | 1710–1785 | 0.015 | 0.005 | 0.0025 |
| Downlink 1800 * | 1805–1880 | 0.005 | 0.005 | 0.0025 |
| DECT | 1880–1900 | 0.005 | 0.005 | 0.0025 |
| Uplink 1900 * | 1920–1980 | 0.003 | 0.003 | 0.0015 |
| Downlink 2100 * | 2110–2170 | 0.010 | 0.003 | 0.0015 |
| WLAN | 2400–2485 | 0.005 | 0.005 | 0.0025 |
2.3. Dose Calculations
2.3.1. Near-Field Dose
Derivation of the SARs
| Near-Field Predictor | Brain SAR | Whole-Body SAR | References | ||
|---|---|---|---|---|---|
| (mW/kg) | Derivation | (mW/kg) | Derivation | ||
| GSM 1 mobile phone calls without headset | 3.198 | − | 0.411 | − | [18] |
| GSM 1 mobile phone calls with headset | 3.198 × 10−3 | 3.198 × 0.001 | 0.411 | 0.411 × 1 | [18,20] |
| UMTS mobile phone calls without headset | 0.023 | − | 0.003 | − | [18] |
| UMTS mobile phone calls with headset | 0.023 × 10−3 | 0.023 × 0.001 | 0.003 | 0.003 × 1 | [18,20] |
| DECT phone calls without eco mode | 0.373 | − | 0.051 | − | [18] |
| DECT phone calls with eco mode | 0.0373 | 0.373 × 0.1 | 0.0051 | 0.051 × 0.1 | [18,20] |
| mobile phone data traffic with mobile internet connection | 0.092 × 10−3 | 0.023 × 4 × 0.001 | 0.012 | 0.003 × 4 × 1 | [18,20,21,22,23,24] |
| mobile phone close to body (passive mobile phone data traffic) | 0.092 × 10−3 | 0.023 × 4 × 0.001 | 0.012 | 0.003 × 4 × 1 | [18,20,21,22,23,24] |
| mobile phone data traffic with WLAN | 0.092 × 10−3 | 0.023 × 4 × 0.001 | 0.012 | 0.003 × 4 × 1 | [18,20,21,22,23,24] |
| computer, laptop and tablet use with WLAN | 0.092 × 10−3 | 0.023 × 4 × 0.001 | 0.012 | 0.003 × 4 × 1 | [18,20,21,22,23,24] |
2.3.2. Far-Field Dose
Geospatial Propagation Model
2.3.3. Multivariable Regression Models
Combining Near-Field and Far-Field Dose
2.4. Comparison of Dose Calculations with Personal Measurements
3. Results
3.1. Near-Field Dose
3.1.1. Near-Field Predictors
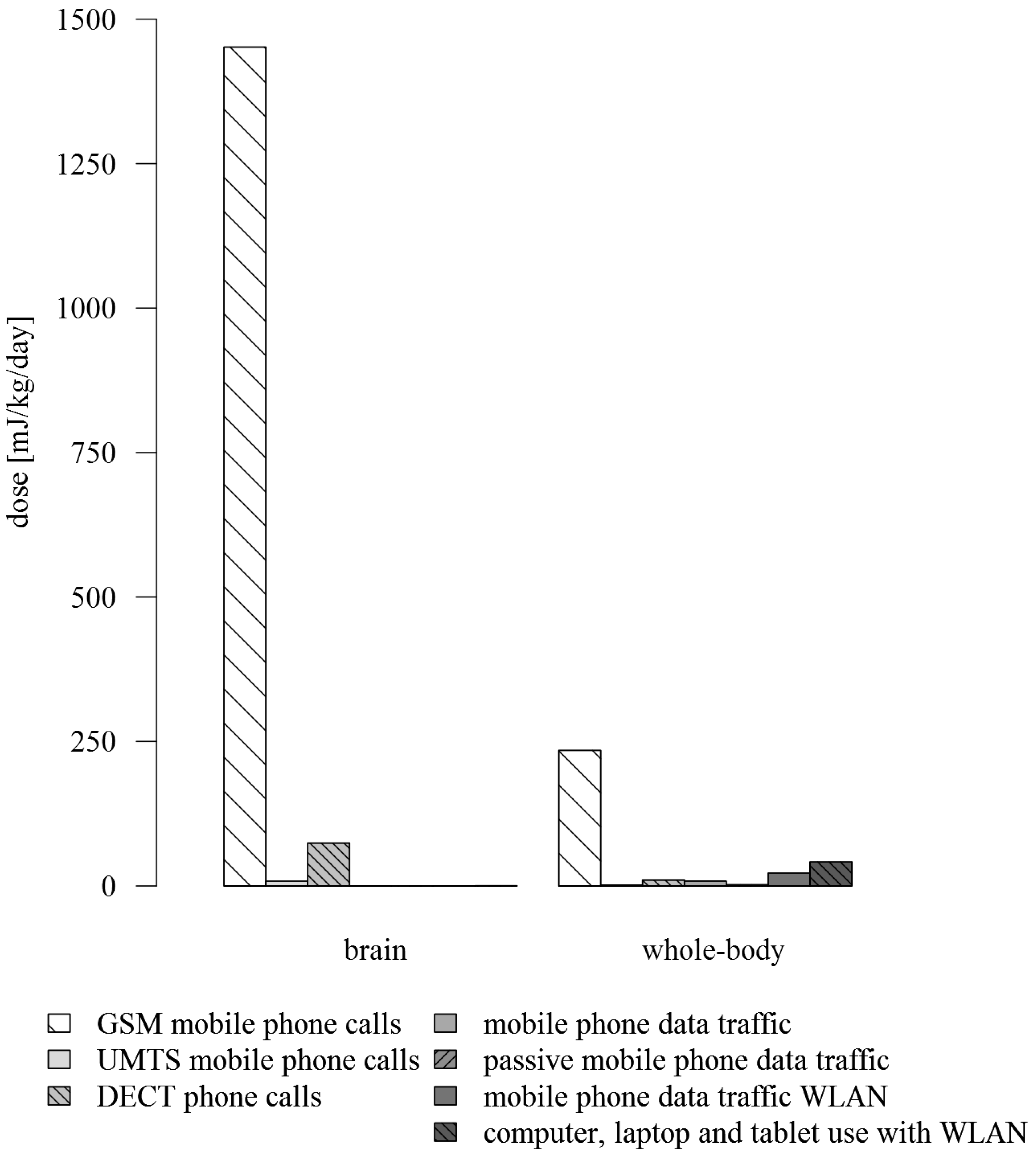
3.1.2. Near-Field Dose
| Near-Field Predictor | Brain SAR (mW/kg) | Whole-Body SAR (mW/kg) | Exposure Duration (min/day) | Brain Dose Rate (mJ/kg/min) | Whole-Body Dose Rate (mJ/kg/min) | Brain Dose (mJ/kg/day) | Whole-Body Dose (mJ/kg/day) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Value | Value | Mean (SD) | Value | Value | Mean (%) | Min | Median | Max | Mean (%) | Min | Median | Max | |
| GSM 1 mobile phone calls without headset | 3.198 | 0.411 | 7.6 (13.0) | 191.88 | 24.66 | − | − | − | − | − | − | − | − |
| GSM 1 mobile phone calls with headset | 0.003198 | 0.411 | 1.9 (7.6) | 0.19 | 24.66 | − | − | − | − | − | − | − | − |
| GSM 1 mobile phone calls headset considered 2 | − | − | 9.5 (16.7) | − | − | 1451.78 (94.6%) | 0.00 | 601.90 | 22587.02 | 234.47 (73.3%) | 0.00 | 85.14 | 3785.98 |
| UMTS mobile phone calls without headset | 0.023 | 0.003 | 5.8 (14.8) | 1.38 | 0.18 | − | − | − | − | − | − | − | − |
| UMTS mobile phone calls with headset | 0.000023 | 0.003 | 1.9 (8.1) | 0.001 | 0.18 | − | − | − | − | − | − | − | − |
| UMTS mobile phone calls headset considered 2 | − | − | 7.7 (19.9) | − | − | 8.04 (0.5%) | 0.00 | 2.57 | 217.49 | 1.39 (0.4%) | 0.00 | 0.37 | 34.20 |
| DECT phone calls without eco mode | 0.373 | 0.051 | − | 22.38 | 3.06 | − | − | − | − | − | − | − | − |
| DECT phone calls with eco mode | 0.0373 | 0.0051 | − | 2.24 | 0.31 | − | − | − | − | − | − | − | − |
| DECT phone calls eco mode considered 3 | − | − | 9.0 (10.9) | − | − | 74.10 (4.8%) | 0.00 | 18.70 | 1364.86 | 10.13 (3.2%) | 0.00 | 2.61 | 190.28 |
| Mobile phone data traffic | 0.000092 | 0.012 | 11.5 (22.5) | 0.01 | 0.72 | 0.06 (0.004%) | 0.00 | 0.01 | 0.54 | 8.29 (2.6%) | 0.00 | 1.63 | 70.89 |
| Mobile phone close to the body (passive data traffic) 4 | 0.000092 | 0.012 | 265.2 (349.5) | 0.00006 | 0.01 | 0.01 (0.001%) | 0.00 | 0.01 | 0.08 | 1.91 (0.6%) | 0.00 | 0.86 | 10.37 |
| Mobile phone data traffic WLAN | 0.000092 | 0.012 | 30.6 (35.0) | 0.01 | 0.72 | 0.17 (0.01%) | 0.00 | 0.10 | 0.54 | 22.03 (6.9%) | 0.00 | 13.68 | 70.89 |
| Computer, laptop and tablet use with WLAN | 0.000092 | 0.012 | 57.6 (83.3) | 0.01 | 0.72 | 0.32 (0.02%) | 0.00 | 0.17 | 3.42 | 41.46 (13.0%) | 0.00 | 21.60 | 446.40 |

3.2. Far-Field Dose
3.2.1. Far-Field Predictors
- Availability of WLAN in school: +0.49 μW/m² (WLAN);
- Availability of WLAN at home and not switching off the base station during night: +1.02 μW/m² (WLAN);
- Number of smartphones used at home: +9.39 μW/m² per smartphone (Uplink);
- Time spent in trains: +0.07 μW/m² per minute spent in trains (WLAN), +1.06 μW/m² per minute spent in trains (Uplink);
- Time spent in buses: +0.64 μW/m² per minute spent in buses (Uplink).
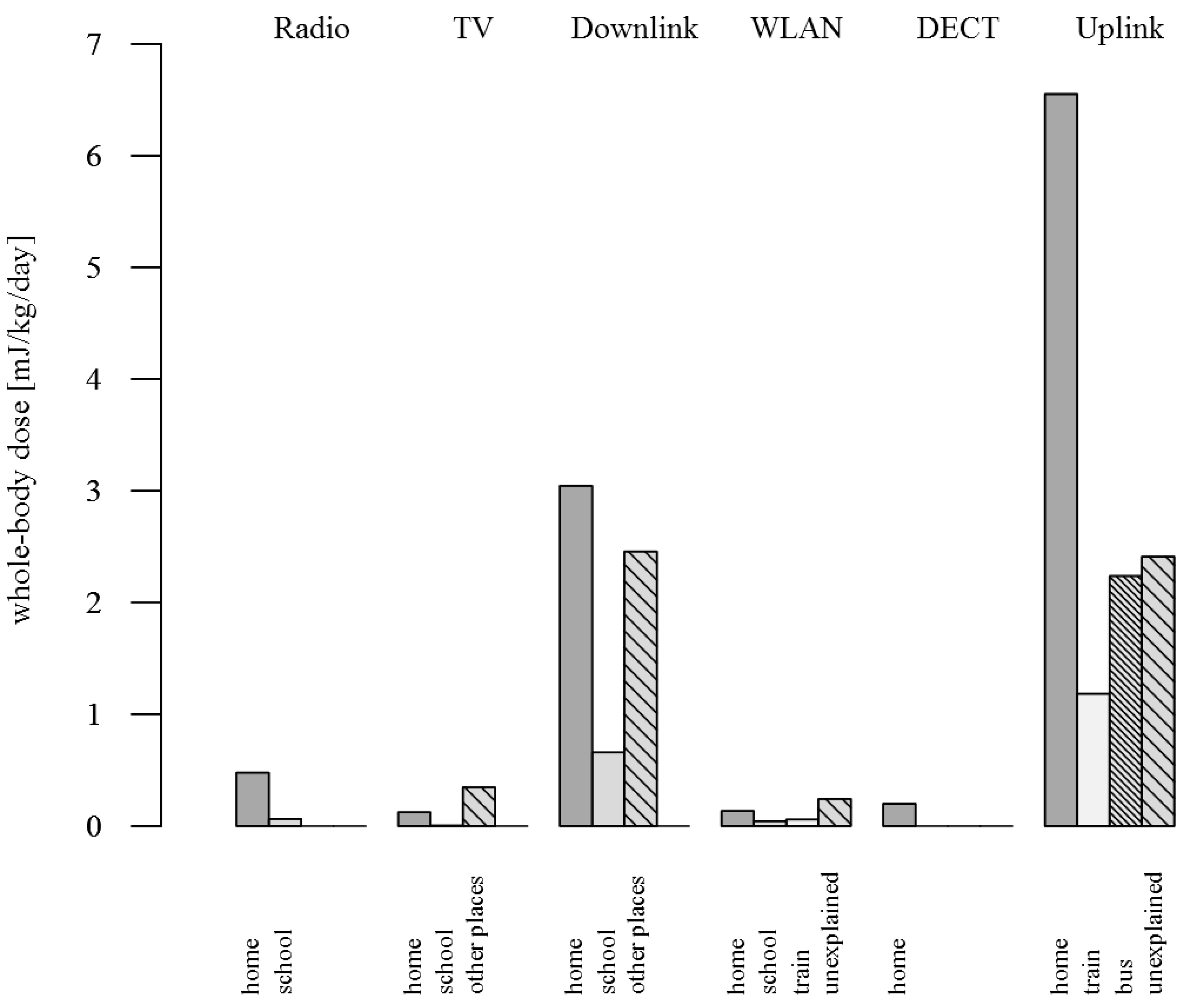
3.2.2. Far-Field Dose
| Band | Description | SAR ((mW/kg)/(mW/m²)) | Power Flux Density (mW/m²) | Dose Rate ((mJ/kg)/(mW/m²)/min) | Dose (mJ/kg/day) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Derivation | Mean (%) | Min | Median | Max | ||||
| Radio 1 | Radio broadcast transmitter | 0.001 | 0.002 | modelling | 0.09 | 0.16 (0.6%) | 0.00 | 0.07 | 3.30 |
| TV | Television broadcast transmitter | 0.008 | 0.001 | modelling and personal measurements | 0.46 | 0.79 (3.1%) | 0.58 | 0.58 | 14.40 |
| Downlink 900 | Transmission from base station to mobile phone handset | 0.007 | − | − | 0.41 | − | − | − | − |
| Downlink 1800 | Transmission from base station to mobile phone handset | 0.003 | − | − | 0.19 | − | − | − | − |
| Downlink 2100 | Transmission from base station to mobile phone handset | 0.003 | − | − | 0.17 | − | − | − | − |
| Downlink | Downlink 900+ Downlink 1800+ Downlink 2100 | − | 0.019 | modelling and personal measurements | − | 8.43 (33.5%) | 3.76 | 5.02 | 124.64 |
| WLAN | Wireless local area network | 0.002 | 0.002 | prediction regression model | 0.14 | 0.39 (1.6%) | 0.20 | 0.40 | 2.37 |
| DECT | Digital enhanced cordless telecommunications | 0.003 | 0.001 | personal measurements | 0.17 | 0.19 (0.8%) | 0.19 | 0.19 | 0.19 |
| Uplink 2 | Transmission from mobile phone handset to base station | 0.004 | 0.041 | prediction regression model | 0.26 | 15.22 (60.4%) | 2.96 | 13.54 | 71.16 |
| Band | Description | SAR((mW/kg)/(mW/m²)) | Power Flux Density(mW/m²) | Dose Rate((mJ/kg)/(mW/m²)/min) | Dose(mJ/kg/day) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Derivation | Mean (%) | Min | Median | Max | ||||
| Radio 1 | Radio broadcast transmitter | 0.005 | 0.002 | modelling | 0.29 | 0.54 (2.7%) | 0.00 | 0.22 | 11.30 |
| TV | Television broadcast transmitter | 0.005 | 0.001 | modelling and personal measurements | 0.27 | 0.47 (2.3%) | 0.35 | 0.35 | 8.61 |
| Downlink 900 | Transmission from base station to mobile phone handset | 0.004 | − | − | 0.26 | −- | − | − | − |
| Downlink 1800 | Transmission from base station to mobile phone handset | 0.003 | − | − | 0.20 | − | − | − | − |
| Downlink 2100 | Transmission from base station to mobile phone handset | 0.003 | − | − | 0.18 | − | − | − | − |
| Downlink | Downlink 900+ Downlink 1800+ Downlink 2100 | − | 0.019 | modelling and personal measurements | − | 6.16 (30.4%) | 2.46 | 3.47 | 86.19 |
| WLAN | Wireless local area network | 0.003 | 0.002 | prediction regression model | 0.17 | 0.48 (2.4%) | 0.24 | 0.49 | 2.90 |
| DECT | Digital enhanced cordless telecommunications | 0.003 | 0.001 | personal measurements | 0.18 | 0.20 (1.0%) | 0.20 | 0.20 | 0.20 |
| Uplink 2 | Transmission from mobile phone handset to base station | 0.004 | 0.041 | prediction regression model | 0.21 | 12.38 (61.2%) | 2.41 | 11.01 | 57.87 |

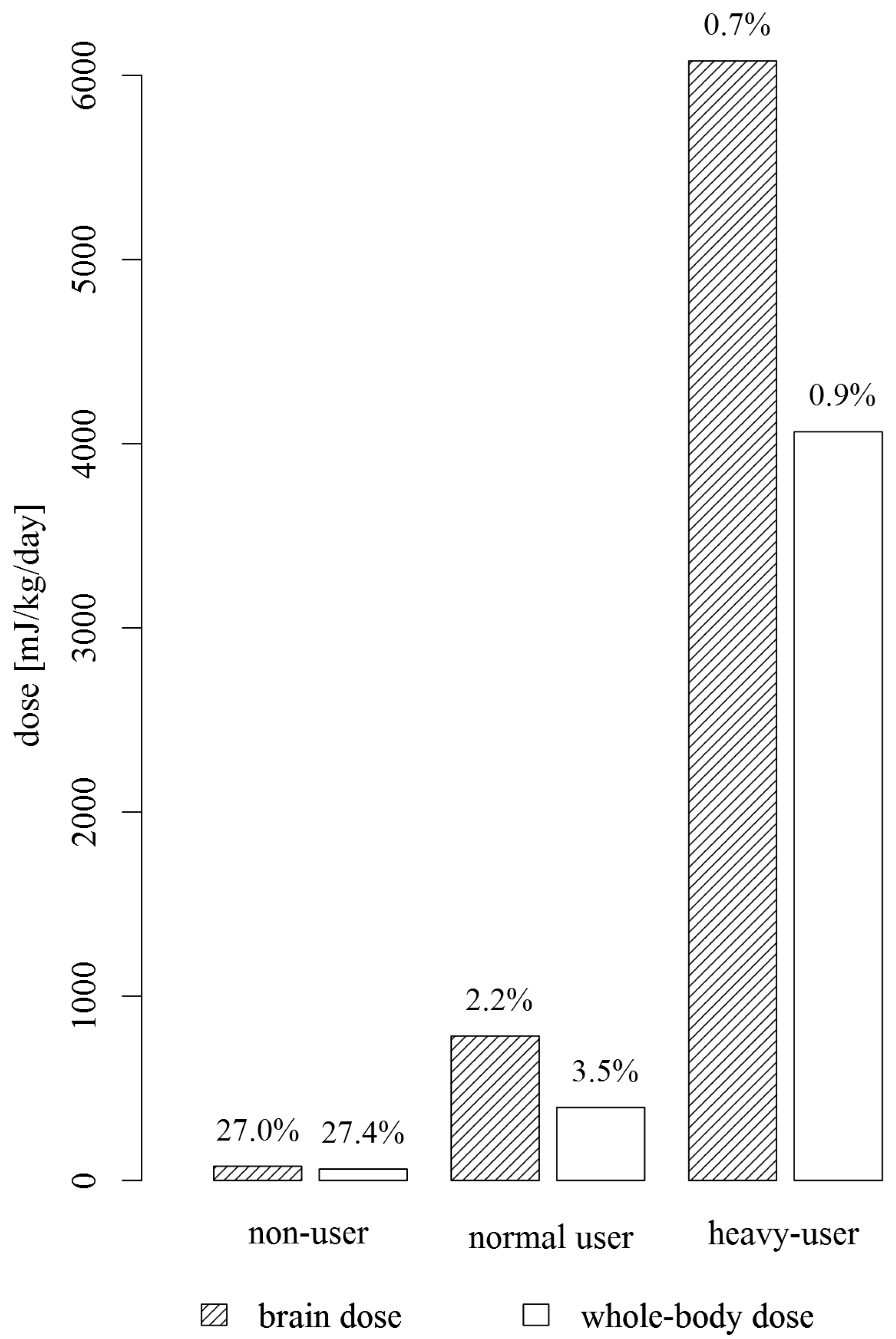
3.3. Combining Near-Field and Far-Field Dose

3.4. Comparing Dose Calculations and Personal Measurements

4. Discussion
4.1. Near-Field Exposure
4.2. Far-Field Exposure
4.3. Comparing Dose Calculations and Personal Measurements
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Heinrich, S.; Thomas, S.; Heumann, C.; von Kries, R.; Radon, K. Association between exposure to radiofrequency electromagnetic fields assessed by dosimetry and acute symptoms in children and adolescents: A population based cross-sectional study. Environ. Health 2010. [Google Scholar] [CrossRef]
- Heinrich, S.; Thomas, S.; Heumann, C.; von Kries, R.; Radon, K. The impact of exposure to radio frequency electromagnetic fields on chronic well-being in young people—A cross-sectional study based on personal dosimetry. Environ. Int. 2011, 37, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Heinrich, S.; von Kries, R.; Radon, K. Exposure to radio-frequency electromagnetic fields and behavioural problems in Bavarian children and adolescents. Eur. J. Epidemiol. 2010, 25, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Inyang, I.; Benke, G.; McKenzie, R.; Abramson, M. Comparison of measuring instruments for radiofrequency radiation from mobile telephones in epidemiological studies: Implications for exposure assessment. J. Expo. Sci. Environ. Epidemiol. 2008, 18, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Röösli, M.; Frei, P.; Bolte, J.; Neubauer, G.; Cardis, E.; Feychting, M.; Gajsek, P.; Heinrich, S.; Joseph, W.; Mann, S.; et al. Conduct of a personal radiofrequency electromagnetic field measurement study: Proposed study protocol. Environ. Health 2010. [Google Scholar] [CrossRef] [Green Version]
- Beekhuizen, J.; Vermeulen, R.; Kromhout, H.; Bürgi, A.; Huss, A. Geospatial modelling of electromagnetic fields from mobile phone base stations. Sci. Total Environ. 2013, 445, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Breckenkamp, J.; Neitzke, H.P.; Bornkessel, C.; Berg-Beckhoff, G. Applicability of an exposure model for the determination of emissions from mobile phone base stations. Radiat. Prot. Dosim. 2008, 131, 474–481. [Google Scholar] [CrossRef]
- Briggs, D.; Beale, L.; Bennett, J.; Toledano, M.B.; de Hoogh, K. A geographical model of radio-frequency power density around mobile phone masts. Sci. Total Environ. 2012, 426, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Bürgi, A.; Frei, P.; Theis, G.; Mohler, E.; Braun-Fahrländer, C.; Fröhlich, J.; Neubauer, G.; Egger, M.; Röösli, M. A model for radiofrequency electromagnetic field predictions at outdoor and indoor locations in the context of epidemiological research. Bioelectromagnetics 2010, 31, 226–236. [Google Scholar] [PubMed]
- Bürgi, A.; Theis, G.; Siegenthaler, A.; Röösli, M. Exposure modeling of high-frequency electromagnetic fields. J. Expo. Sci. Environ. Epidemiol. 2008, 18, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; Toledano, M.B.; Bennett, J.; Beale, L.; de Hoogh, K.; Best, N.; Briggs, D.J. Mobile phone base stations and early childhood cancers: Case-control study. BMJ 2010. [Google Scholar] [CrossRef]
- Ha, M.; Im, H.; Lee, M.; Kim, H.J.; Kim, B.C.; Gimm, Y.M.; Pack, J.K. Radio-frequency radiation exposure from AM radio transmitters and childhood leukemia and brain cancer. Amer. J. Epidemiol. 2007, 166, 270–279. [Google Scholar] [CrossRef]
- Merzenich, H.; Schmiedel, S.; Bennack, S.; Bruggemeyer, H.; Philipp, J.; Blettner, M.; Schuz, J. Childhood leukemia in relation to radio frequency electromagnetic fields in the vicinity of TV and radio broadcast transmitters. Amer. J. Epidemiol. 2008, 168, 1169–1178. [Google Scholar] [CrossRef]
- Frei, P.; Mohler, E.; Bürgi, A.; Fröhlich, J.; Neubauer, G.; Braun-Fahrländer, C.; Röösli, M. A prediction model for personal radio frequency electromagnetic field exposure. Sci. Total Environ. 2009, 408, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Frei, P.; Mohler, E.; Braun-Fahrländer, C.; Fröhlich, J.; Neubauer, G.; Röösli, M. Cohort study on the effects of everyday life radio frequency electromagnetic field exposure on non-specific symptoms and tinnitus. Environ. Int. 2012, 38, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohler, E.; Frei, P.; Fröhlich, J.; Braun-Fahrländer, C.; Röösli, M. Exposure to radiofrequency electromagnetic fields and sleep quality: a prospective cohort study. PLoS One 2012. [Google Scholar] [CrossRef] [Green Version]
- Cardis, E.; Varsier, N.; Bowman, J.D.; Deltour, I.; Figuerola, J.; Mann, S.; Moissonnier, M.; Taki, M.; Vecchia, P.; Villegas, R.; et al. Estimation of RF energy absorbed in the brain from mobile phones in the interphone study. Occup. Environ. Med. 2011, 68, 686–693. [Google Scholar] [CrossRef] [PubMed]
- Lauer, O.; Frei, P.; Gosselin, M.C.; Joseph, W.; Röösli, M.; Fröhlich, J. Combining near- and far-field exposure for an organ-specific and whole-body RF-EMF proxy for epidemiological research: A reference case. Bioelectromagnetics 2013, 34, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Lauer, O.; Leidenberger, P.; Müri, M.; Zahner, M.; Fröhlich, J. A Novel Measurement System for Environmental Exposure Monitoring. In Proceedings of the ACM Conference on Embedded Networked Sensor Systems, Seattle, WA, USA, 1–4 November, 2011.
- SEAWIND Sound Exposure & Risk Assessment of Wireless Network Devices Final Summary Report, 2013. Available online: http://seawind-fp7.eu/uploads/SEAWIND_FINAL.pdf (accessed on 7 June 2013).
- Gati, A.; Hadjem, A.; Man-Fai, W.; Wiart, J. Exposure induced by WCDMA mobiles phones in operating networks. IEEE Wirel. Commun. 2009, 8, 5723–5727. [Google Scholar] [CrossRef]
- Hadjem, A.; Conil, E.; Gati, A.; Wong, M.-F.; Wiart, J. Analysis of power absorbed by children's head as a result of new usages of mobile phone. IEEE Trans. Electromagn. Compat. 2010, 52, 812–819. [Google Scholar] [CrossRef]
- Huang, Y.; Wiart, J.; Varsier, N.; Person, C. Sensitivity Analysis of Downlink Received and Uplink Emitted Powers in a Geographical Area to ICT Usage Parameters. In Proceedings of The Annual Meeting of BEMS and EBEA, Capetown, South Africa, 8-13 June, 2014.
- Persson, T.; Tornevik, C.; Larsson, L.E.; Loven, J. Output power distributions of terminals in a 3G mobile communication network. Bioelectromagnetics 2012, 33, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Vrijheid, M.; Mann, S.; Vecchia, P.; Wiart, J.; Taki, M.; Ardoino, L.; Armstrong, B.K.; Auvinen, A.; Bedard, D.; Berg-Beckhoff, G.; et al. Determinants of mobile phone output power in a multinational study: Implications for exposure assessment. Occup. Environ. Med. 2009, 66, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Beekhuizen, J.; Vermeulen, R.; van Eijsden, M.; van Strien, R.; Bürgi, A.; Loomans, E.; Guxens, M.; Kromhout, H.; Huss, A. Modelling indoor electromagnetic fields (EMF) from mobile phone base stations for epidemiological studies. Environ. Int. 2014, 67, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Bolte, J.F.; Eikelboom, T. Personal radiofrequency electromagnetic field measurements in the Netherlands: Exposure level and variability for everyday activities, times of day and types of area. Environ. Int. 2012, 48, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Frei, P.; Mohler, E.; Neubauer, G.; Theis, G.; Bürgi, A.; Fröhlich, J.; Braun-Fahrländer, C.; Bolte, J.; Egger, M.; Röösli, M. Temporal and spatial variability of personal exposure to radio frequency electromagnetic fields. Environ. Res. 2009, 109, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Urbinello, D.; Röösli, M. Impact of one’s own mobile phone in stand-by mode on personal radiofrequency electromagnetic field exposure. J. Expo. Sci. Environ. Epidemiol. 2013, 23, 545–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aerts, S.; Plets, D.; Thielens, A.; Martens, L.; Joseph, W. Impact of a small cell on the RF-EMF exposure in a train. Int. J. Environ. Res. Public Health 2015, 12, 2639–2652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roosli, M.; Frei, P.; Mohler, E.; Hug, K. Systematic review on the health effects of exposure to radiofrequency electromagnetic fields from mobile phone base stations. Bull. World Health Organ. 2010, 88, 887–896. [Google Scholar] [CrossRef] [PubMed]
- Aydin, D.; Feychting, M.; Schuz, J.; Andersen, T.V.; Poulsen, A.H.; Prochazka, M.; Klaeboe, L.; Kuehni, C.E.; Tynes, T.; Roosli, M. Impact of random and systematic recall errors and selection bias in case—Control studies on mobile phone use and brain tumors in adolescents (CEFALO study). Bioelectromagnetics 2011, 32, 396–407. [Google Scholar] [CrossRef] [PubMed]
- Inyang, I.; Benke, G.; Morrissey, J.; McKenzie, R.; Abramson, M. How well do adolescents recall use of mobile telephones? Results of a validation study. BMC Med. Res. Methodol. 2009. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Roser, K.; Schoeni, A.; Bürgi, A.; Röösli, M. Development of an RF-EMF Exposure Surrogate for Epidemiologic Research. Int. J. Environ. Res. Public Health 2015, 12, 5634-5656. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120505634
Roser K, Schoeni A, Bürgi A, Röösli M. Development of an RF-EMF Exposure Surrogate for Epidemiologic Research. International Journal of Environmental Research and Public Health. 2015; 12(5):5634-5656. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120505634
Chicago/Turabian StyleRoser, Katharina, Anna Schoeni, Alfred Bürgi, and Martin Röösli. 2015. "Development of an RF-EMF Exposure Surrogate for Epidemiologic Research" International Journal of Environmental Research and Public Health 12, no. 5: 5634-5656. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120505634