
The Impact of Arts Activity on Nursing Staff Well-Being: An Intervention in the Workplace

Abstract
:
1. Introduction
2. Materials and Methods
Data Analysis
3. Results
4. Discussion
4.1. A Positive Impact on Health and Well-Being
4.2. Increasing Positive Emotions: A Positive Impact on Mental Well-Being
4.3. Reducing Stress
4.4. Reducing Fatigue
4.5. Increasing Sense of Community at Work
5. Conclusions
Limitations of the Study
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| WEMWBS | The Warwick-Edinburgh Mental Well-Being Scale |
| SF-36 | The Short Form-36 Health Survey Questionnaire |
| Stress scale | The Reeder Stress Scale |
| MFI-20 | The Multidimensional Fatigue Inventory |
References
- WHO. The European Health Report 2012: Charting the Way to Well-Being; WHO: Copenhagen, Denmark, 2013. [Google Scholar]
- Fujiwara, D.; Dolan, O.; Lawton, R. Creative Occupations and Subjective Wellbeing; Nesta Working Paper: London, UK, 2015. [Google Scholar]
- WHO. Mental Health Declaration for Europe. Facing the Challenges, Building Solutions; WHO: Geneva, Switzerland, 2005. [Google Scholar]
- Stewart-Brown, S.; Janmohamed, K. Warwick-Edinburgh Mental Well-being Scale (WEMWBS) User Guide Version 1; Parkinson, J., Ed.; Warwick Medical School, University of Warwick, NHS Health Scotland: Coventry, UK, 2008. [Google Scholar]
- Persechino, B.; Valenti, A.; Ronchetti, M.; Rondinone, B.M.; Tecco, C.; Vitali, S.; Iavicoli, S. Work-Related Stress Risk Assessment in Italy: A Methodological Proposal Adapted to Regulatory Guidelines. Saf. Health Work 2013, 4, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Jeffrey, K.; Mahony, S.; Michaelson, J.; Abdallah, S. Well-being at Work. A Review of the Literature; Murphy, M., Ed.; New Economics Foundation: London, UK, 2014. [Google Scholar]
- European pact for mental health and well-being. In Proceedings of the EU High-level Conference Together for Mental Health and Well-being, Brussels, Belgium, 12–13 June 2008.
- Eurofound. Fifth European Working Conditions Survey; Publications Office of the European Union: Luxembourg, Luxembourg, 2012. [Google Scholar]
- Montesinos, M.J.L. Psychosocial study about the consequences of work in hospital nurses as human resource management. Rev. Latino-Am. Enferm. 2013, 21, 61–70. [Google Scholar] [CrossRef]
- Fernandes, M.F.P.; Komessu, J.H. Nurses’ challenges in view of the pain and suffering of families of terminal patients. Rev. Esc. Enferm. USP 2013, 47, 246–253. [Google Scholar]
- Aiken, L.H.; Sloane, D.M.; Bruyneel, L.; Heede, K.V.; Sermeus, W. Nurses’ reports of working conditions and hospital quality of care in 12 countries in Europe. Int. J. Nurs. Stud. 2013, 5, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Filha, M.M.T.; Costa, M.A.S.; Guilam, M.C.R. Occupational stress and self-rated health among nurses. Rev. Latino-Am. Enferm. 2013, 21, 475–483. [Google Scholar] [CrossRef]
- Oliveira, J.D.S.; Alchieri, J.C.; Júnior, J.M.P.; Miranda, F.A.N.; Almeida, M.G. Nurses’ social representations of work related stress in an emergency room. Rev. Esc. Enferm. USP 2013, 47, 980–985. [Google Scholar]
- Czaja, A.S.; Moss, M.; Mealer, M. Symptoms of Post-traumatic Stress Disorder Among Pediatric Acute Care Nurses. J. Pediatr. Nurs. 2012, 27, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Ariapooran, S. Compassion fatigue and burnout in Iranian nurses: The role of perceived social support. Iran. J. Nurs. Midwifery Res. 2014, 19, 279–284. [Google Scholar] [PubMed]
- Khamisa, N.; Peltzer, K.; Oldenburg, B. Burnout in Relation to Specific Contributing Factors and Health Outcomes among Nurses: A Systematic Review. Int. J. Environ. Res. Public Health 2013, 10, 2214–2240. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.F.; You, L.M.; Liu, K.; Zheng, J.; Fang, J.B.; Lu, M.M.; Lv, A.L.; Ma, W.G.; Wang, J.; Wang, S.H.; et al. The Association of Chinese Hospital Work Environment with Nurse Burnout, Job Satisfaction, and Intention to Leave. Nurs. Outlook 2014, 62, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Daraiseh, N.M.; Davis, K.G.; Pan, W. Sources of work-related acute fatigue in United States hospital nurses. Nurs. Health Sci. 2014, 16, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.M.; Labrecque, C.A.; Candler, S.G.; Newell-Amato, D.; Messler, J.; Wolf, M.; Caughman, S.W.; Raggi-Moore, J. Communicating Through the Arts: Lessons for Medicine and Public Health. J. Health Commun. Int. Perspect. 2013, 18, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Adeane, M. Is there a place for the arts in our modern healthcare system? Perspect. Public Health 2013, 133, 19–20. [Google Scholar] [PubMed]
- Hume, V. Creative care: The role of the arts in hospital. Nurs. Manag. 2010, 17, 16–20. [Google Scholar]
- Macneill, P.U. The arts and medicine: A challenging relationship. Med. Humanit. 2011, 37, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Almalki, M.J.; FitzGerald, G.; Clark, M. The relationship between quality of work life and turnover intention of primary health care nurses in Saudi Arabia. BMC Health Serv. Res. 2012. [Google Scholar] [CrossRef] [PubMed]
- Perry, L.; Lamont, S.; Brunero, S.; Gallagher, R.; Duffield, C. The mental health of nurses in acute teaching hospital settings: A cross-sectional survey. BMC Nurs. 2015. [Google Scholar] [CrossRef] [PubMed]
- Chan, Z.C.Y. Exploration of artistry in nursing teaching activities. Nurse Educ. Today 2014, 34, 924–928. [Google Scholar] [CrossRef] [PubMed]
- Jack, K. “Putting the words ‘I am sad’, just doesn’t quite cut it sometimes!”: The use of art to promote emotional awareness in nursing students. Nurse Educ. Today 2012, 32, 811–816. [Google Scholar] [CrossRef] [PubMed]
- O¨zcan, N.K.; Bilgin, H.; Eracar, N. The Use of Expressive Methods for Developing Empathic Skills. Issues Ment. Health Nurs. 2011, 32, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Potash, J.S.; Chen, J.Y.; Tsang, J.P.Y. Medical student mandala making for holistic well-being. Med. Humanit. 2016, 42, 17–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Titus, J.E.; Sinacore, A.L. Art-making and well-being in healthy young adult women. Arts Psychother. 2013, 40, 29–36. [Google Scholar] [CrossRef]
- Guerin, P.; Guerin, B.; Tedmanson, D.; Clark, Y. How can country, spirituality, music and arts contribute to Indigenous mental health and wellbeing? Austral. Psychiatry 2011, 19, S38–S41. [Google Scholar] [CrossRef] [PubMed]
- Kelaher, M.; Dunt, D.; Berman, N.; Curry, S.; Joubert, L.; Johnson, V. Evaluating the health impacts of participation in Australian community arts groups. Health Promot. Int. 2014, 29, 392–402. [Google Scholar] [CrossRef] [PubMed]
- Phinney, A.; Moody, E.M.; Small, J.A. The Effect of a Community-Engaged Arts Program on Older Adults’ Well-being. Can. J. Aging 2014, 33, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Theorell, T.; Osika, W.; Leineweber, C.; Hanson, L.L.M.; Bojner Horwitz, E.; Westerlund, H. Is cultural activity at work related to mental health in employees? Int. Arch. Occup. Environ. Health 2013, 86, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Salzano, A.T.; Lindemann, E.; Tronsky, L.N. The effectiveness of a collaborative art-making task on reducing stress in hospice caregivers. Arts Psychother. 2013, 40, 45–52. [Google Scholar] [CrossRef]
- Karpavičiūtė, S.; Parkinson, C. Arts Activity and Well-being in the Workplace: A Pilot Study of Health Service Workers in Lithuania. Semin. Neurol. 2015, 19, 210–216. [Google Scholar]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Stewart-Brown, S. The Warwick-Edinburgh mental well-being scale (WEMWBS): Development and UK validation. Health Quality Life Outcomes 2007. [Google Scholar] [CrossRef] [PubMed]
- Karpavičiūtė, S. Warwick-Edinburgh Mental Well-Being Scale. Biol. Psychiatry Psychopharmacol. 2014, 16, 110–112. [Google Scholar]
- Maheswaran, H.; Weich, S.; Powell, J.; Stewart-Brown, S. Evaluating the responsiveness of the Warwick Edinburgh Mental Well-Being Scale (WEMWBS): Group and individual level analysis. Health Qual Life Outcomes 2012. [Google Scholar] [CrossRef] [PubMed]
- Crone, D.M.; O’Connell, E.E.; Tyson, P.J.; Clark-Stone, F.; Opher, S.; James, D.V. “Art Lift” intervention to improve mental well-being: An observational study from UK general practice. Int. J. Ment. Health Nurs. 2013, 22, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-ltem short-form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Joslin, L.E.; Davis, C.R.; Dolan, P.; Clark, E.M. Quality of life and neck pain in nurses. Int. J. Occup. Med. Environ. Health 2014, 27, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Staniūtė, M.; Brožaitienė, J. Assessment of health-related quality of life in depression patients compared with coronary artery disease patients and general population subjects. Biol. Psychiatry Psychopharmacol. 2008, 10, 3–6. [Google Scholar]
- Staniūtė, M. Health related quality of life assessment using SF-36 questionnaire. Biol. Psychiatry Psychopharmacol. 2007, 9, 22–25. [Google Scholar]
- Suner-Soler, R.; Grau-Martin, A.; Font-Mayolas, S.; Gras, M.E.; Bertran, C.; Sullman, M.J.M. Burnout and quality of life among Spanish healthcare personnel. J. Psychiatr. Ment. Health Nurs. 2013, 20, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Galatsch, M.; Li, J.; Derycke, H.; Müller, B.H.; Hasselhorn, H.M. Effects of Requested, Forced and Denied Shift Schedule Change on Work Ability and Health of Nurses in Europe. Results from the European NEXT-Study. BMC Public Health 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reeder, L.G.; Chapman, J.M.; Coulson, A.H. Socioenvironmental stress, tranquilizers and cardiovascular disease. Proc. Excerpta Med. Int. Congr. Ser. 1968, 182, 226–238. [Google Scholar]
- Vanagas, G.; Axelsson, B.S. The factors associated to psychosocial stress among general practitioners in Lithuania. Cross-sectional study. BMC Health Serv. Res. 2005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gustainienė, L.; Bakšienė, V. Relationship among stresogenic aspects of work, social, and subjective health among medical personnel. Public Health 2008, 2, 47–55. [Google Scholar]
- Šidlauskaitė-Stripeikienė, I.; Žemaitienė, N.; Klumbienė, J. Stress and social support relations in adults from districts of Lithuania. Public Health 2008, 4, 31–36. [Google Scholar]
- Smets, E.M.; Garssen, B.; Bonke, B.; De Haes, J.C. The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J. Psychosom. Res. 1995, 39, 315–325. [Google Scholar] [CrossRef]
- Lin, J.-M.S.; Brimmer, D.J.; Maloney, E.M.; Nyarko, E.; BeLue, R.; Reeves, W.C. Further validation of the Multidimensional Fatigue Inventory in a US adult population sample. Popul. Health Metr. 2009. [Google Scholar] [CrossRef]
- Stankus, A. The Multidimensional Fatigue Inventory. Biol. Psychiatry Psychopharmacol. 2007, 9, 86–87. [Google Scholar]
- Hagelin, C.L.; Wengström, Y.; Runesdotter, S.; Fürst, C.J. The psychometric properties of the Swedish Multidimensional Fatigue Inventory MFI-20 in four different populations. Acta Oncol. 2007, 46, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Riad, W.; Mansour, A.; Moussa, A. Anesthesiologists work-related exhaustion: A comparison study with other hospital employees. Saud. J. Anaesth. 2011, 5, 244–247. [Google Scholar] [CrossRef] [PubMed]
- Stankus, A. Validation of the Multidimensional Fatigue Inventory in patients with coronary artery disease. In Proceedings of the II KMU Institute of Psychophysiology and Rehabilitation Annual Conference, Palanga, Lithuania, 20 December 2002; p. 39.
- Pukkaew, C. Assessment of the effectiveness of internet-based distance learning through the VClass e-Education platform. IRROLD 2013, 14, 255–276. [Google Scholar]
- Reed, L.F.; Battistutta, D.; Young, J.; Newman, B. Prevalence and risk factors for foot and ankle musculoskeletal disorders experienced by nurses. BMC Musculoskel. Disord. 2014. [Google Scholar] [CrossRef] [PubMed]
- Arquaharson, B.; Bell, C.; Johnston, D.; Jones, M.; Schofield, P.; Allan, J.; Ricketts, I.; Morrison, K.; Johnston, M. Nursing stress and patient care: Real-time investigation of the effect of nursing tasks and demands on psychological stress, physiological stress, and job performance: Study protocol. J. Adv. Nurs. 2013, 69, 2327–2335. [Google Scholar] [CrossRef] [PubMed]
- Gordon-Nesbitt, R.; Arts for Health. Exploring the Longitudinal Relationship between Arts Engagement and Health; Parkinson, C., Ed.; Arts for Health, Manchester Metropolitan University: Manchester, UK, 2015. [Google Scholar]
- Bungay, H.; Vella-Burrows, T. The effects of participating in creative activities on the health and well-being of children and young people: A rapid review of the literature. Perspect. Public Health 2013, 133, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A. Beyond the borders: The use of art participation for the promotion of health and well-being in Britain and Denmark. Arts Health. Int. J. Res. Policy Pract. 2013, 5, 204–215. [Google Scholar] [CrossRef] [PubMed]
- Swindells, R.; Lawthom, R.; Rowley, K.; Siddiquee, A.; Kilroy, A.; Kagan, C. Eudaimonic well-being and community arts participation. Perspect. Public Health 2013, 133, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Cameron, M.; Crane, N.; Ings, R.; Taylor, K. Promoting well-being through creativity: How arts and public health can learn from each other. Perspect. Public Health 2013, 133, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Broderick, S. Arts practices in unreasonable doubt? Reflections on understandings of arts practices in healthcare contexts. Arts Health Int. J. Res. Policy Pract. 2011, 3, 95–109. [Google Scholar] [CrossRef] [PubMed]
- Stuckey, H.L.; Nobel, J. The Connection between Art, Healing, and Public Health: A Review of Current Literature. Am. J. Public Health 2010, 100, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Philipp, R.; Gibbons, N.; Thorne, P.; Wiltshire, L.; Burrough, J.; Easterby, J. Evaluation of a community arts installation event in support of public health. Perspect. Public Health 2015, 135, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Foresight Mental Capital and Wellbeing Project. Mental Capital and Wellbeing: Making the Most of Ourselves in the 21st Century. Final Project Report; The Government Office for Science: London, UK, 2008. [Google Scholar]
- Aked, J.; Thompson, S. Five Ways to Wellbeing. New applications, New Ways of Thinking; NEF, NHS Confederation: London, UK, 2011. [Google Scholar]
- Wright, P.R.; Pascoe, R. Eudaimonia and creativity: The art of human flourishing. Camb. J. Educ. 2015, 45, 295–306. [Google Scholar] [CrossRef]
- Kilroy, A.; Garner, C.; Parkinson, C.; Kagan, C.; Senior, P. Invest to Save: Arts in Health Evaluation. Exploring the Impact of Creativity, Culture and the Arts, on Health and Well-being; Arts for Health, Manchester Metropolitan University: Manchester, UK, 2008. [Google Scholar]
- Abdallah, S.; Mahony, S.; Marks, N.; Michaelson, J.; Seaford, C.; Stoll, L.; Thompson, S. Measuring our Progress the Power of Well-being; NEF: London, UK, 2011. [Google Scholar]
- Rollins, J.; Sonke, J.; Cohen, R.; Boles, A.; Jiahan, L. State of the Field Report: Arts in Healthcare; Society for the Arts in Healthcare: Washington, DC, USA, 2009. [Google Scholar]
- Maben, J.; Peccei, R.; Adams, M.; Robert, G.; Richardson, A.; Murrells, T.; Morrow, E. National Institute for Health Research Service Delivery and Organization Programme. Exploring the Relationships between Patients’ Experiences of Care and the Influence of Staff Motivation, Affect and Wellbeing; National institute for health research, Service Delivery and Organisation Programme: London, UK, 2012. [Google Scholar]
- Sonke, J.; Pesata, V.; Arce, L.; Carytsas, F.P.; Zemina, K.; Jokisch, C. The effects of arts-in-medicine programming on the medical-surgical work environment. Arts Health 2015, 7, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Bygren, L.O.; Weissglas, G.; Wikström, B.M.; Konlaan, B.B.; Grjibovski, A.; Karlsson, A.B.; Andersson, S.O.; Sjöström, M. Cultural participation and health: A randomized controlled trial among medical care staff. Psychosom. Med. 2009, 71, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Tuisku, K.; Pulkki-Råback, L.; Ahola, K.; Hakanen, J.; Virtanen, M. Cultural leisure activities and well-being at work: A study among health care professionals. J. Appl. Arts Health 2012, 1, 273–287. [Google Scholar] [CrossRef]
- Munyewende, P.O.; Rispel, L.C.; Chirwa, T. Positive practice environments influence job satisfaction of primary health care clinic nursing managers in two South African provinces. Hum. Resour. Health 2014. [Google Scholar] [CrossRef] [PubMed]
- Repar, P.A.; Reid, S. Creatively Caring: Effects of Arts-Based Encounters on Hospice Caregivers in South Africa. J. Pain Symptom Manag. 2014, 47, 946–954. [Google Scholar] [CrossRef] [PubMed]
- Huss, E.; Sarid, O. Visually transforming artwork and guided imagery as a way to reduce work related stress: A quantitative pilot study. Arts Psychother. 2014, 41, 409–412. [Google Scholar] [CrossRef]
- Lin, S.C.; Tsai, K.W.; Chen, M.W.; Koo, M. Association between fatigue and Internet addiction in female hospital nurses. J. Adv. Nurs. 2013, 69, 374–383. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, V.J.C.; Power, S.; Greiner, B.A. Perceived occupational stress in nurses working in Ireland. Occup. Med. 2010, 60, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Fradelos, E.; Mpelegrinos, S.; Mparo, C.; Vassilopoulou, C.; Argyrou, P.; Tsironi, M.; Zyga, S.; Theofilou, P. Burnout syndrome impacts quality life nursing professionals. The contribution of perceived social support. Prog. Health Sci. 2014, 4, 102–109. [Google Scholar]
- Gerikienė, V. Work Satisfaction of Lithuanian Community Nurses in the Context of Primary Health Care Reform; Doctoral Dissertation, Biomedical Sciences, LUHS: Kaunas, Lithuania, 2007. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Characteristics * | Intervention Group n (%) | Control Group n (%) |
|---|---|---|
| Gender | ||
| Female | 56 (100) | 59 (100) |
| Age in groups (years) | ||
| 21–24 | 7 (12) | 2 (3) |
| 25–39 | 11 (20) | 9 (15) |
| 40–54 | 32 (57) | 33 (56) |
| 55–70 | 6 (11) | 15 (25) |
| Education | ||
| Secondary | 9 (16) | 7 (12) |
| Vocational ** | 16 (29) | 30 (51) |
| Higher non-university | 17 (30) | 14 (24) |
| Higher university | 14 (25) | 8 (13) |
| Position at work | ||
| Nurse | 39 (70) | 48 (81) |
| Nurse assistant | 17 (30) | 11 (19) |
| Work experience as nurses/nurse assistants (years) | ||
| 1–5 | 15 (27) | 9 (15) |
| 6–10 | 15 (27) | 8 (14) |
| 11–15 | 3 (5) | 5 (8) |
| 16–20 | 8 (14) | 11 (19) |
| ≥21 | 15 (27) | 26 (44) |
| Work experience at this hospital (years) | ||
| 1–5 | 15 (27) | 15 (25) |
| 6–10 | 14 (25) | 12 (20) |
| 11–15 | 4 (7) | 5 (8) |
| 16–20 | 7 (12) | 9 (15) |
| ≥21 | 16 (29) | 18 (31) |
| Department | ||
| Palliative care | 12 (21) | 13 (22) |
| Surgery | 19 (34) | 18 (31) |
| Therapeutic | 10 (18) | 8 (14) |
| Emergency | 6 (11) | 9 (15) |
| Obstetrics | 4 (7) | 5 (8) |
| Intensive care | 5 (9) | 6 (10) |
| Personal workload in this hospital | ||
| 0.6–1.0 full working time | 29 (52) | 27 (46) |
| More than 1.1–1.5 full working time | 27 (48) | 32 (54) |
| Work shift | ||
| Day | 23 (41) | 20 (25) |
| Night | 4 (7) | 8 (17) |
| 24-h | 1 (2) | 5 (14) |
| Rotating | 28 (50) | 26 (44) |
| Work is physically exhausting | ||
| Rarely | 5 (9) | 4 (7) |
| Sometimes | 10 (18) | 20 (34) |
| Often | 27 (48) | 22 (37) |
| Always | 14 (25) | 13 (22) |
| Work is emotionally difficult | ||
| Rarely | 1 (2) | 4 (7) |
| Sometimes | 8 (14) | 17 (29) |
| Often | 24 (43) | 21 (35) |
| Always | 23 (41) | 17 (29) |
| Title of Subscale/Scale | The Differences in the Total Scores in Subscales/Scales between Baseline ** and Post-intervention *** in the Intervention Group | ||
|---|---|---|---|
| Before Art Activities, n = 56 Mean (SD ****) | After Art Activities, n = 56 Mean (SD ****) | (p value) | |
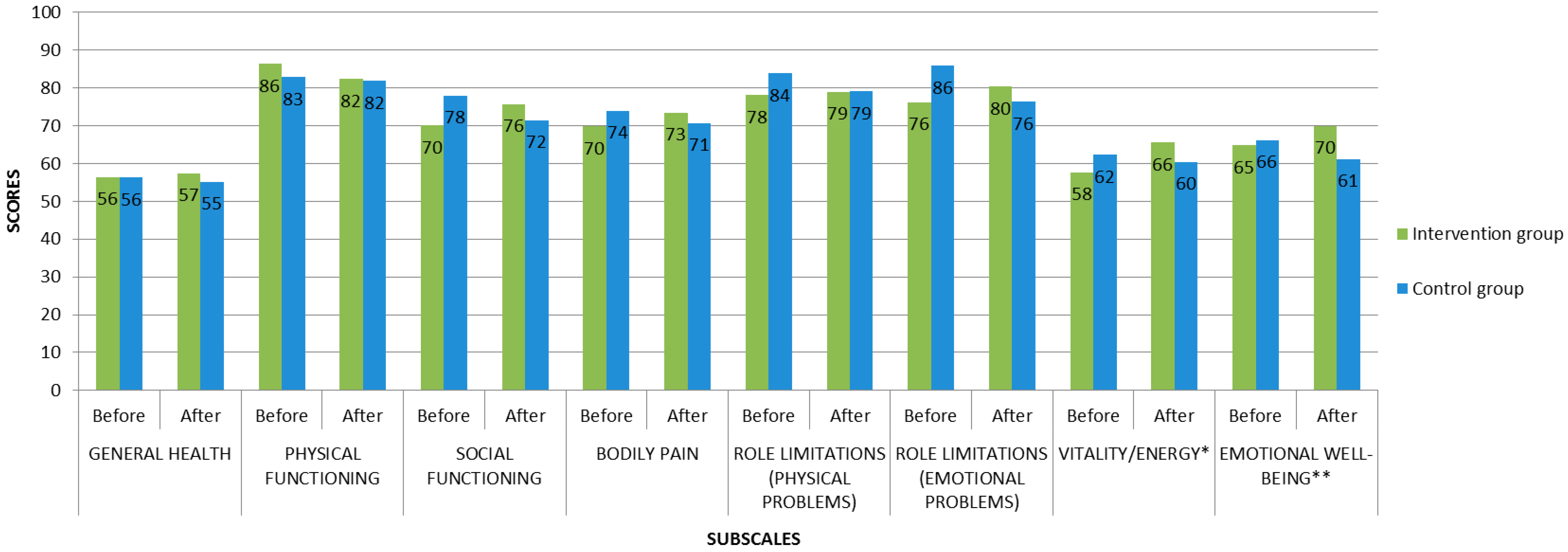
| SF-36 Physical functioning | 86 (14) | 82 (15) | (0.06) |
| SF-36 General health | 56 (14) | 57 (15) | (0.25) |
| SF-36 Vitality/Energy | 58 (15) | 66 (14) | * |
| SF-36 Social functioning | 70 (19) | 76 (20) | (0.06) |
| SF-36 Bodily pain | 70 (20) | 73 (18) | (0.36) |
| SF-36 Role limitations (physical problems) | 78 (27) | 79 (33) | (0.74) |
| SF-36 Role limitations (emotional problems) | 76 (28) | 80 (29) | (0.51) |
| SF-36 Emotional wellbeing | 65 (15) | 70 (15) | (0.14) |
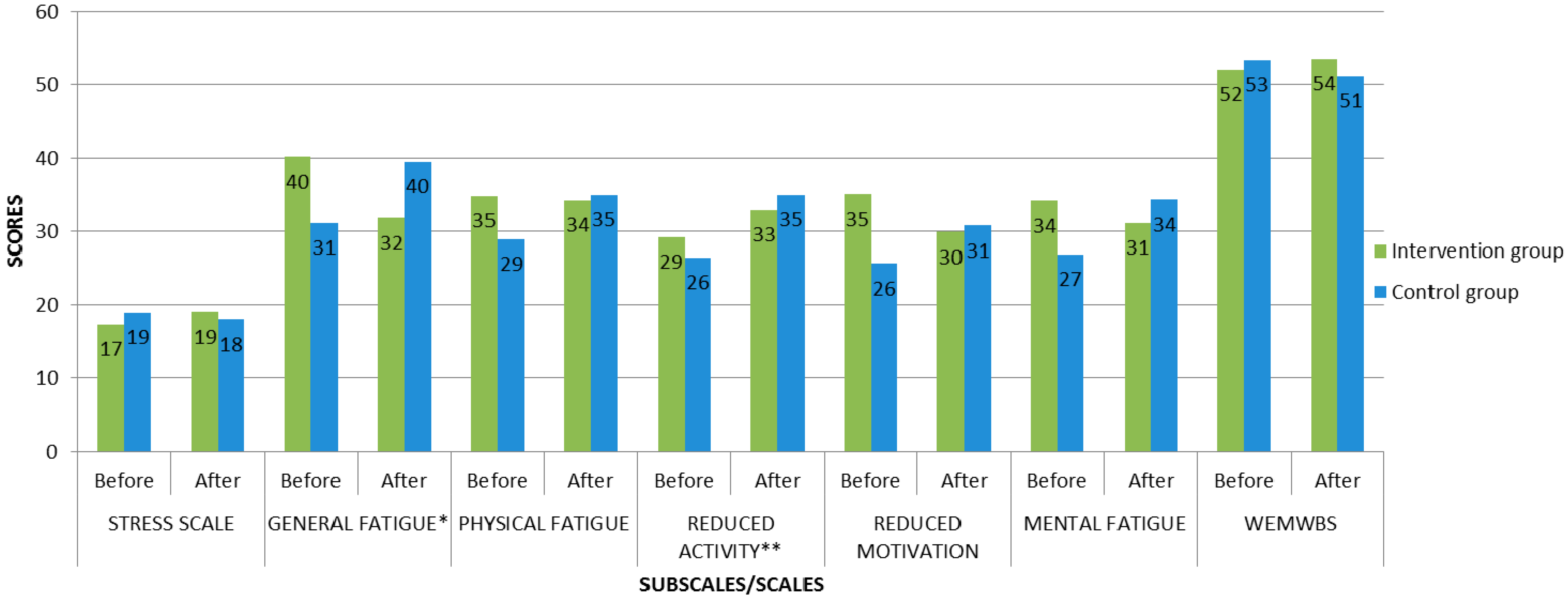
| MFI-20 General fatigue | 40 (21) | 32 (22) | (0.03) * |
| MFI-20 Physical fatigue | 35 (23) | 34 (23) | (0.58) |
| MFI-20 Reduced motivation | 35 (18) | 30 (20) | (0.13) |
| MFI-20 Mental fatigue | 34 (20) | 31 (19) | (0.39) |
| MFI-20 Reduced activity | 29 (19) | 33 (21) | (0.47) |
| WEMBWS | 52 (7) | 54 (7) | (0.15) |
| Stress scale | 17 (4) | 19 (4) | (0.06) |
| Title of Subscale/Scale | The Differences in the Total Scores in Subscales/Scales between Baseline ** and Post-intervention *** in the Control Group | ||
|---|---|---|---|
| Before Art Activities, n = 59 Mean (SD ****) | After Art Activities, n = 55 Mean (SD ****) | (p value) | |
| SF-36 Physical functioning | 83 (19) | 82 (18) | (0.98) |
| SF-36 General health | 56 (14) | 55 (13) | (0.60) |
| SF-36 Vitality/Energy | 62 (13) | 60 (16) | (0.89) |
| SF-36 Social functioning | 78 (18) | 72 (21) | (0.17) |
| SF-36 Bodily pain | 74 (23) | 71 (20) | (0.44) |
| SF-36 Role limitations (physical problems) | 84 (28) | 79 (30) | (0.54) |
| SF-36 Role limitations (emotional problems) | 86 (29) | 76 (31) | (0.20) |
| SF-36 Emotional wellbeing | 66 (17) | 61 (17) | (0.24) |
| MFI-20 General fatigue | 31 (22) | 40 (23) | (0.10) |
| MFI-20 Physical fatigue | 29 (23) | 35 (23) | (0.25) |
| MFI-20 Reduced motivation | 26 (19) | 31 (18) | (0.18) |
| MFI-20 Mental fatigue | 27 (22) | 34 (25) | (0.19) |
| MFI-20 Reduced activity | 26 (22) | 35 (25) | (0.05) * |
| WEMBWS | 53 (7) | 51 (9) | (0.14) |
| Stress scale | 19 (5) | 18 (4) | (0.43) |
| Title of Subscale/Scale | The Differences in the Total Scores in Subscales/Scales between Intervention Group and Control Group at Post–Intervention ** | ||
|---|---|---|---|
| Intervention Group, n = 56 Mean (SD ***) | Control Group, n = 55 Mean (SD ***) | (p value) | |
| SF-36 Physical functioning | 82 (15) | 82 (18) | (0.73) |
| SF-36 General health | 57 (15) | 55 (13) | (0.15) |
| SF-36 Vitality/Energy | 66 (14) | 60 (16) | (0.07) |
| SF-36 Social functioning | 76 (20) | 72 (21) | (0.24) |
| SF-36 Bodily pain | 73 (18) | 71 (20) | (0.43) |
| SF-36 Role limitations (physical problems) | 79 (33) | 79 (30) | (0.51) |
| SF-36 Role limitations (emotional problems) | 80 (29) | 76 (31) | (0.40) |
| SF-36 Emotional wellbeing | 70 (15) | 61 (17) | (0.00) * |
| MFI-20 General fatigue | 32 (22) | 40 (23) | (0.07) |
| MFI-20 Physical fatigue | 34 (23) | 35 (23) | (0.95) |
| MFI-20 Reduced motivation | 30 (20) | 31 (18) | (0.65) |
| MFI-20 Mental fatigue | 31 (19) | 34 (25) | (0.64) |
| MFI-20 Reduced activity | 33 (21) | 35 (25) | (0.67) |
| WEMBWS | 54 (7) | 51 (9) | (0.07) |
| Stress scale | 19 (4) | 18 (4) | (0.32) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karpavičiūtė, S.; Macijauskienė, J. The Impact of Arts Activity on Nursing Staff Well-Being: An Intervention in the Workplace. Int. J. Environ. Res. Public Health 2016, 13, 435. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13040435
Karpavičiūtė S, Macijauskienė J. The Impact of Arts Activity on Nursing Staff Well-Being: An Intervention in the Workplace. International Journal of Environmental Research and Public Health. 2016; 13(4):435. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13040435
Chicago/Turabian StyleKarpavičiūtė, Simona, and Jūratė Macijauskienė. 2016. "The Impact of Arts Activity on Nursing Staff Well-Being: An Intervention in the Workplace" International Journal of Environmental Research and Public Health 13, no. 4: 435. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13040435