Perspective of Pakistani Physicians towards Hospital Antimicrobial Stewardship Programs: A Multisite Exploratory Qualitative Study

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
2.3. Interview Guide Development
2.4. Participant Enrollment
2.5. Inclusion and Exclusion Criteria
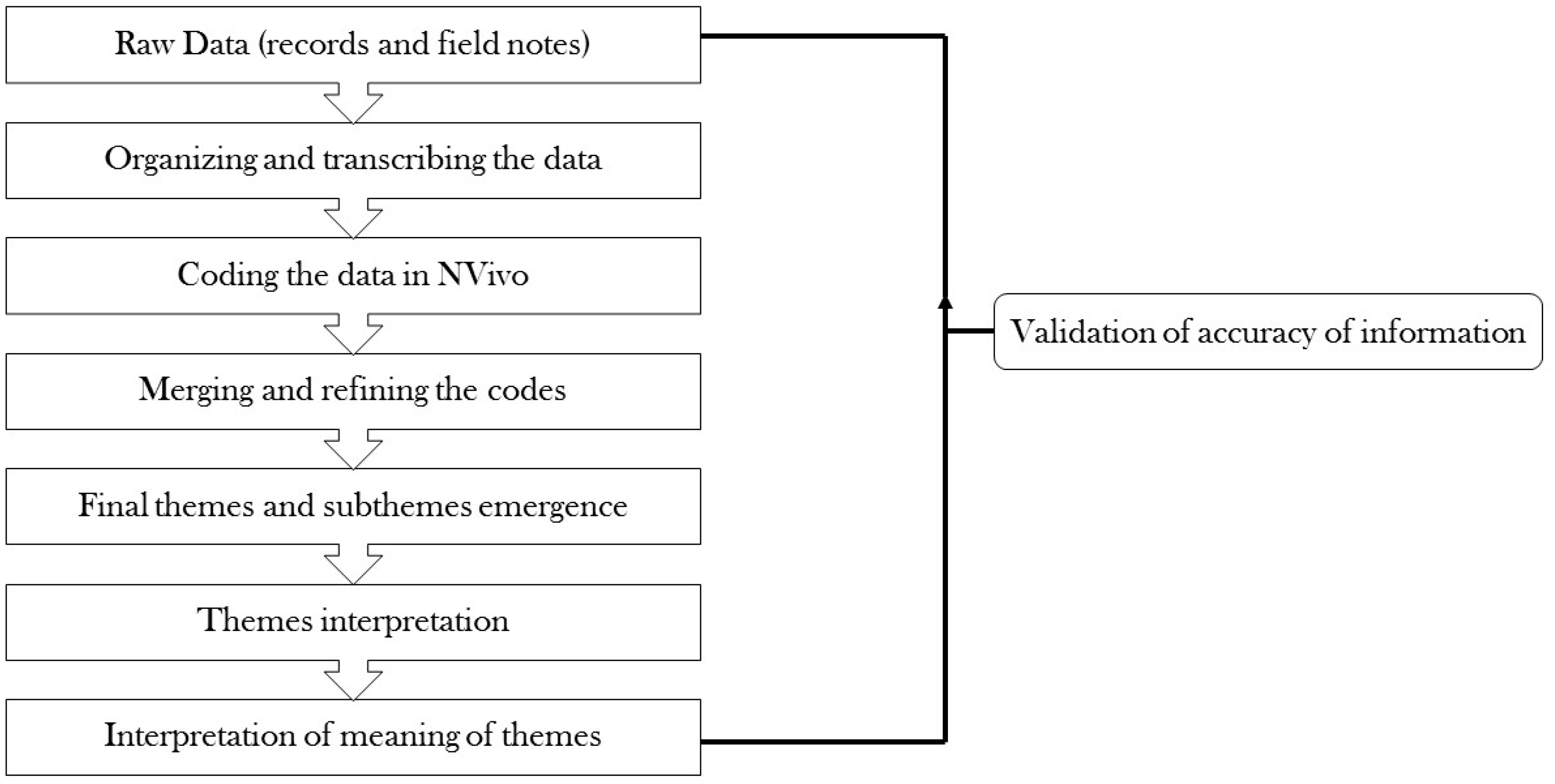
2.6. Qualitative Analysis
2.7. Ethical Permission
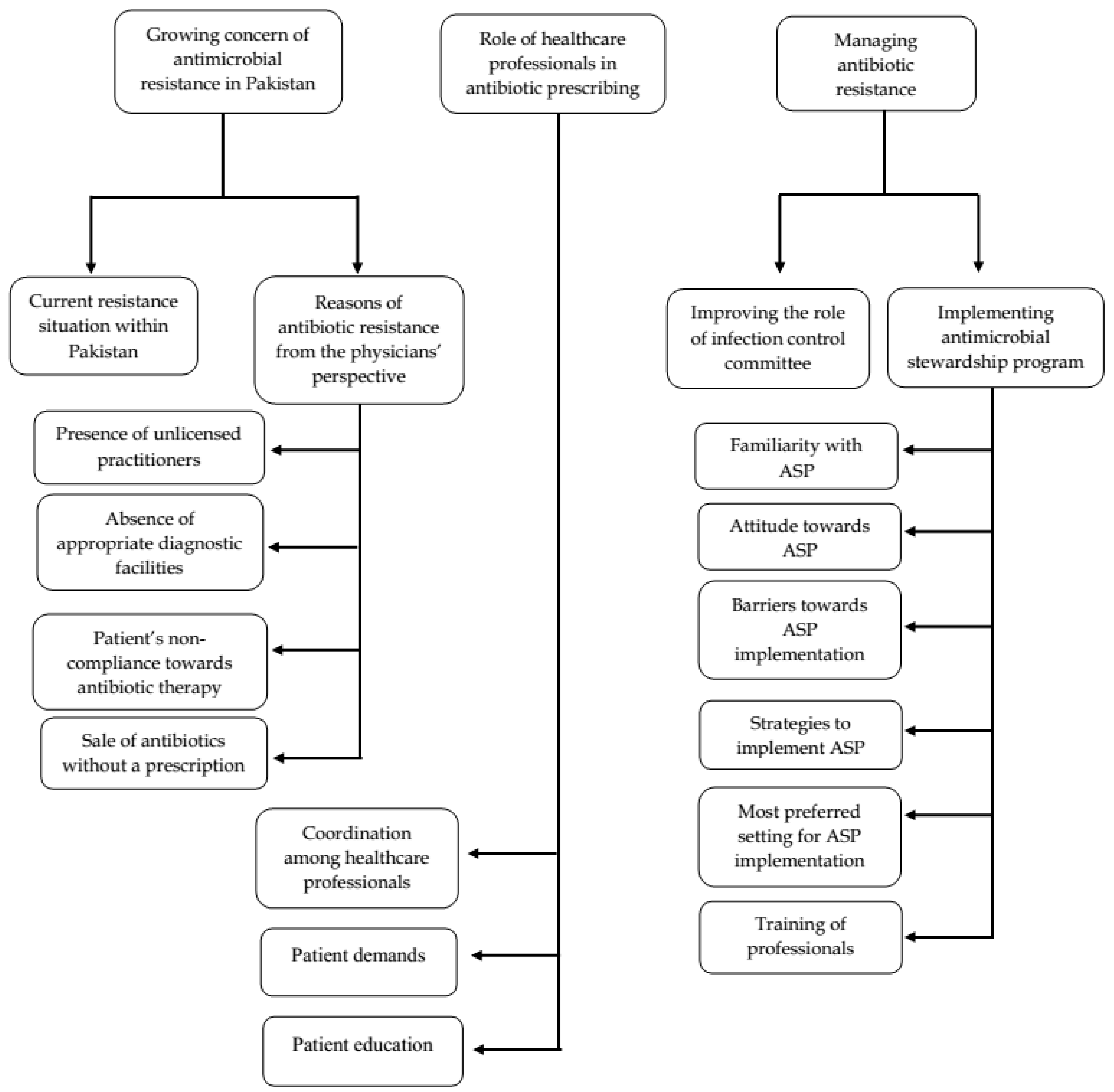
3. Results
3.1. Growing Concern of Antimicrobial Resistance in Pakistan
3.1.1. Current Resistance Situation
“Resistance of course is increasing in Pakistan and, unfortunately, we are facing this problem with higher intensity every year (...) Now, at this stage I feel that a simple sore throat infection that was easily cured by erythromycin is no longer cured due to the emergence of resistance.” (P7)
“There is no doubt that there is a strong relationship between irrational use of antibiotics with antibiotic resistance and it is continuously growing in Pakistan.” (P2)
3.1.2. Reasons of Antibiotic Resistance from the Perspective of Physicians
Presence of Unlicensed Medical Practitioners
“Unfortunately, there are (a) number of other so-called doctors such as unlicensed practitioners who most of the times prescribe antibiotics in an irrational way, thus increasing the risk of antibiotic resistance.” (P6)
“In our country, unlicensed practitioners prescribe antibiotics without any rational approach and (are) amplifying the problem of antibiotic resistance.” (P16)
Absence of Appropriate Diagnostic Facilities
“There is a lack of appropriate diagnostic facilities, especially in basic health units and district hospitals. This further promotes the use of antibiotics without culture sensitivity tests.” (P8)
“Physicians in the periphery and remote areas mostly use broad spectrum antibiotics and they do not bother to recommend lab tests, maybe due to (the) absence of diagnostic facilities.” (P5)
Patient’s Non-Compliance towards Antibiotic Therapy
“Non-compliance with antibiotic treatment is common among patients, as most of them don’t complete their treatment course and when they use the same medicine in future, it is unable to cure them due to the emergence of resistance.” (P9)
“They (patients) will stop their antibiotics once they think that they are feeling better and do not complete the recommended duration of therapy as we have instructed them.” (P12)
“Resistance against antibiotics is increasing just like (in) other countries (….) there is a need to educate and encourage patients to complete their antibiotic course to prevent the risk of resistance against antibiotics.” (P21)
Sale of Antibiotics without a Prescription
“Unfortunately, self-medication is very common, and you can take any drug like antibiotics freely from the medical store or pharmacy without a prescription.” (P5)
“In my view, the origin of resistance is the inappropriate use of antibiotics by the community. This risk will be higher if they are able to get these pills without any prescription.” (P11)
“I think the government should take meaningful steps to prevent the sale of antibiotics without a prescription.” (15)
3.2. Role of Healthcare Professionals in Antibiotic Prescribing
3.2.1. Coordination among Healthcare Professionals
“A major weakness in government sector hospitals is (the) lack of mutual cooperation among different healthcare professionals, which could affect the rational use of antibiotics in hospitals.” (P3)
“Antibiotic prescribing is a team (effort) in which every professional is doing his/her job (……) being a physician, we can discuss about antibiotic therapy with pharmacists and nurses. Obviously, microbiologist will be helpful for lab results. So, in this way, we will have evidence-based antibiotic therapy, which will improve the quality of life of patients, but unfortunately this coordination is missing.” (P13)
“No doubt if all the stakeholders of our healthcare system including physicians, pharmacists, nurses, and microbiologists work in coordination then it will definitely improve antibiotic usage within a hospital.” (P15)
3.2.2. Demand of Antibiotics
“[Patients] sometimes demand antibiotics and try to influence our clinical judgment, especially in government hospitals. They know basic information about antibiotics, like names of certain very common antibiotics, which (were) possibly tracked from friends or the Internet, and they are pre-occupied with receiving a specific antibiotic. So, they even ask us to prescribe that antibiotic.” (P3)
“This is a demand of patients to be given an antibiotic, but we try to prescribe only if it is suitable for them. Some patients come after evaluation from several doctors and show us their previous prescriptions and tell us which antibiotic showed better results, then in such situations, we sometimes prescribe the same antibiotic.” (P6)
3.2.3. Patient Education
“Well, there are certain infections like flu in which antibiotics should not be given. I try to counsel such patients and tell them that it’s nothing but an extra expense from your pocket. Most of the times, patients agree to what I say.” (P1)
“We educate patients suffering from viral infections by saying that symptomatic relief is all that you need, and antibiotics use will be ineffective in this case. In reality, self-medication with antibiotics is very common in our community and the rate of compliance is higher if you prescribe a greater number of pills to the patients regardless of their clinical needs.” (P7)
3.3. Managing Antibiotic Resistance
3.3.1. Improving the Role of Infection Control Committee
“Yes, we do have an infection control committee in our hospital, but at the moment I am not satisfied with its current performance due to [the] lack of its active role in reducing the risk of hospital-acquired infections as well in the development of infection prevention policies and treatment guidelines. Its performance must be improved to address resistance issues.” (P20)
“The infection control committee exists in our hospital, but it is in a very pathetic condition. Its working is not up to the mark, probably due to insufficient funds and inadequate staff. (……) There is a need to improve its role to reduce antibiotic resistance.” (P3)
3.3.2. Implementation of ASP in Pakistani hospitals
Familiarity
“To be honest, I am not aware of this program, but now I have some basic information about it after a discussion with you. It seems to be a new concept to rationalize the use of antimicrobials including antibiotics.” (P14)
“Unfortunately, I do not have any prior information about this program.” (P13)
Attitude towards ASP
“I personally do not have any reservation in (regard to) its (ASP) implementation, as it is not only useful for patients but also for physicians.” (P11)
“It is a very useful program and, being a physician, I have (a) very positive attitude towards ASP due to its benefits in (terms of reducing) antibiotic resistance, which will speed up the prognosis rate among patients. If we consider ASP in ideal condition(s) then, of course, this system will have multiple merits.” (P9)
Barriers towards Implementation of ASP
“There will be a lot of barriers. For example, we have heavy patient loads and it would be too difficult for us to get a prior approval of an antibiotic from an ID physician every time (…) Secondly, there will be a need of huge financing to implement hospital ASPs.” (P8)
“I perceive that budgeting, which is the main hindrance, and inadequate resources could be the major barriers in its implementation.” (P1)
“We may not have enough qualified and trained professionals like ID physicians, nurses, microbiologists, and clinical pharmacists who have experience of working in (an) ASP healthcare facility.” (P17)
Preferred ASP Strategies
“As per my opinion, the second one [formulary restriction] will be more effective, as this will restrict the use of antimicrobials. This restriction should be specific to every hospital, but some physicians may resist in order to seek approval before prescribing antibiotics.” (P7)
“Prior approval of prescribing antibiotics will be more beneficial in Pakistan, as this will act as a check point and limit the prescribing of antibiotics by physicians, but this may also challenge the authority of the physicians.” (P4)
“I think we should try to implement a combination of different ASP strategies to determine the best suitable and useful option.” (P12)
Preferred Hospital Setting for ASP Implementation
“Well, we must start this program from tertiary healthcare units and district hospitals, where there are more trained staff and experts. Once they understand it, then they will teach to their juniors and (knowledge will) trickle down from top to bottom.” (P1)
“I think ASP should be implemented first in tertiary hospitals and then step by step to other hospital settings, including secondary and primary.” (P10)
Training of Healthcare Professionals
“Yes, obviously, training is needed in order to get better understanding in the form of workshops or conferences and I think healthcare professionals should have (a) certification from an approved course in order to be the part of ASP.” (P5)
“It will be a good option to train the physicians before the implementation of this program. We need to do some pilot project first and if results are positive then we can continue it with zeal.” (P10)
“Well, training is always necessary in order to get better results. So, all healthcare professionals should be trained before the implementation of ASP in hospitals. In my view, the government should plan a training program accompanied with a certificate, so that only a trained healthcare professional could join the ASP team.” (P18)
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Interview Guide
Antimicrobial Prescribing and Resistance
- How often do you prescribe antibiotics per day?
- How do you deal with patients who demand antibiotics for their illness?
- (a)
- Do you counsel them?
- (b)
- Do they influence your antibiotic prescribing behavior?
- In your opinion, what is the role(s) of other healthcare professionals in your antibiotic prescribing?
- (a)
- How do different healthcare professionals affect your prescribing of antibiotics?
- Could you describe the role of the infection control committee in your hospital?
- (a)
- Are you satisfied with its performance?
- What do you think about antimicrobial resistance in Pakistan?
- (a)
- Is it reducing or increasing?
- (b)
- If it is increasing, then what are the reasons of the increase in resistance?
Perception and Attitude towards the Antimicrobial Stewardship Program (ASP)
- Do you know what the antimicrobial stewardship program is?
- In your view, how can we implement ASP in the public hospitals of Pakistan?
- (a)
- Should we first implement ASP in tertiary care hospitals or basic health units?
- Could you describe the strategies that are the most useful in implementing hospital ASPs in Pakistan (formulary restriction, prospective audit with feedback, combination of these strategies)?
- What will be the benefits of implementing hospital ASPs in Pakistan?
- How will physicians see the implementation of hospital ASPs in Pakistani?
- (a)
- Will they have any sort of reservations on its implementation?
- What are your views about the training of healthcare professionals prior to the implementation of the hospital ASPs in Pakistan?
- In your opinion, what are the barriers in successful implementation of ASP in Pakistani hospitals (unavailability of trained staff, limited resources)?
- Are there any other comments you would like to give about antimicrobial resistance or the antimicrobial stewardship program?
References
- Broom, A.; Broom, J.; Kirby, E. Cultures of resistance? A Bourdieusian analysis of doctors’ antibiotic prescribing. Soc. Sci. Med. 2014, 110, 81–88. [Google Scholar] [CrossRef] [PubMed]
- WHO Antimicrobial Resistance: Global Report on Surveillance. April 2014. Available online: http://www.who.int/drugresistance/documents/surveillancereport/en/ (accessed on 24 October 2018).
- O’neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. 2016. Available online: https://amr-review.org/sites/default/files/160525_Final%20paper_with%20cover.pdf (accessed on 24 October 2018).
- Molnar, A. Antimicrobial Resistance Awareness and Games. Trends Microbiol. 2019, 27, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Tangcharoensathien, V.; Chanvatik, S.; Sommanustweechai, A. Complex determinants of inappropriate use of antibiotics. Bull. World Health Organ. 2018, 96, 141–144. [Google Scholar] [CrossRef]
- Cantón, R.; Horcajada, J.P.; Oliver, A.; Garbajosa, P.R.; Vila, J. Inappropriate use of antibiotics in hospitals: The complex relationship between antibiotic use and antimicrobial resistance. Enferm. Infecc. Y Microbiol. Clin. 2013, 31, 3–11. [Google Scholar] [CrossRef]
- Ingram, P.R.; Seet, J.M.; Budgeon, C.A.; Murray, R. Point-prevalence study of inappropriate antibiotic use at a tertiary Australian hospital. Intern. Med. J. 2012, 42, 719–721. [Google Scholar] [CrossRef]
- CDC Antibiotic Use in the United States 2017: Progress and Opportunities. 2017. Available online: https://www.cdc.gov/antibiotic-use/stewardship-report/pdf/stewardship-report.pdf (accessed on 25 October 2018).
- Baig, M.T.; Sial, A.A.; Huma, A.; Ahmed, M.; Shahid, U.; Syed, N. Irrational antibiotic prescribing practice among children in critical care of tertiary hospitals. Pak. J. Pharm. Sci. 2017, 30 (Suppl. 4), 1483–1489. [Google Scholar]
- Aziz, M.M.; Masood, I.; Yousaf, M.; Saleem, H.; Ye, D.; Fang, Y. Pattern of medication selling and self-medication practices: A study from Punjab, Pakistan. PLoS ONE 2018, 13, e0194240. [Google Scholar] [CrossRef]
- Khan, D.E.A. Centre for Disease Dynamics, Economics & Policy, Situation Analysis Report on Antimicrobial Resistance in Pakistan. 2018. Available online: https://cddep.org/publications/garp-pakistan-situation-analysis/ (accessed on 25 October 2018).
- Butt, Z.A.; Gilani, A.H.; Nanan, D.; Sheikh, A.L.; White, F. Quality of pharmacies in Pakistan: A cross-sectional survey. Int. J. Qual. Health Care 2005, 17, 307–313. [Google Scholar] [CrossRef]
- Joseph, H.A.; Agboatwalla, M.; Hurd, J.; Jacobs-Slifka, K.; Pitz, A.; Bowen, A. What Happens When “Germs Don’t Get Killed and They Attack Again and Again”: Perceptions of Antimicrobial Resistance in the Context of Diarrheal Disease Treatment Among Laypersons and Health-Care Providers in Karachi, Pakistan. Am. J. Trop. Med. Hyg. 2016, 95, 221–228. [Google Scholar] [CrossRef]
- Barker, A.K.; Brown, K.; Ahsan, M.; Sengupta, S.; Safdar, N. What drives inappropriate antibiotic dispensing? A mixed-methods study of pharmacy employee perspectives in Haryana, India. BMJ Open 2017, 7, e013190. [Google Scholar] [CrossRef] [Green Version]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef] [Green Version]
- Shahid, A.; Iftikhar, F.; Arshad, M.K.; Javed, Z.; Sufyan, M.; Ghuman, R.S.; Tarar, Z. Knowledge and attitude of physicians about antimicrobial resistance and their prescribing practices in Services hospital, Lahore, Pakistan. J. Pak. Med. Assoc. 2017, 67, 968. [Google Scholar]
- Dyar, O.J.; Huttner, B.; Schouten, J.; Pulcini, C. What is antimicrobial stewardship? Clin. Microbiol. Infect. 2017, 23, 793–798. [Google Scholar] [CrossRef]
- Buckel, W.R.; Veillette, J.J.; Vento, T.J.; Stenehjem, E. Antimicrobial Stewardship in Community Hospitals. Med. Clin. N. Am. 2018, 102, 913–928. [Google Scholar] [CrossRef]
- Baur, D.; Gladstone, B.P.; Burkert, F.; Carrara, E.; Foschi, F.; Döbele, S.; Tacconelli, E. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 990–1001. [Google Scholar] [CrossRef]
- SHEA Antimicrobial Stewardship. Available online: https://www.shea-online.org/index.php/practice-resources/priority-topics/antimicrobial-stewardship (accessed on 25 October 2018).
- Nori, P.; Guo, Y.; Ostrowsky, B. Creative Collaborations in Antimicrobial Stewardship: Using the Centers for Disease Control and Prevention’s Core Elements as Your Guide. Med. Clin. N. Am. 2018, 102, 845–854. [Google Scholar] [CrossRef]
- Parente, D.M.; Morton, J. Role of the Pharmacist in Antimicrobial Stewardship. Med. Clin. N. Am. 2018, 102, 929–936. [Google Scholar] [CrossRef]
- Lockwood, A.R.; Bolton, N.S.; Winton, M.D.; Carter, J.T. Formalization of an antimicrobial stewardship program in a small community hospital. Am. J. Health Syst. Pharm. 2017, 74 (Suppl. 3), S52–S60. [Google Scholar] [CrossRef]
- Carter, E.J.; Greendyke, W.G.; Furuya, E.Y.; Srinivasan, A.; Shelley, A.N.; Bothra, A.; Saiman, L.; Larson, E.L. Exploring the nurses’ role in antibiotic stewardship: A multisite qualitative study of nurses and infection preventionists. Am. J. Infect. Control 2018, 46, 492–497. [Google Scholar] [CrossRef]
- Monsees, E.; Popejoy, L.; Jackson, M.A.; Lee, B.; Goldman, J. Integrating staff nurses in antibiotic stewardship: Opportunities and barriers. Am. J. Infect. Control 2018, 46, 737–742. [Google Scholar] [CrossRef]
- Brink, A.J.; Messina, A.P.; Feldman, C.; Richards, G.A.; Becker, P.J.; Goff, D.A.; Bauer, K.A.; Nathwani, D.; van den Bergh, D. Antimicrobial stewardship across 47 South African hospitals: An implementation study. Lancet Infect. Dis. 2016, 16, 1017–1025. [Google Scholar] [CrossRef]
- Momattin, H.; Al-Ali, A.Y.; Mohammed, K.; Al-Tawfiq, J.A. Benchmarking of antibiotic usage: An adjustment to reflect antibiotic stewardship program outcome in a hospital in Saudi Arabia. J. Infect. Public Health 2018, 11, 310–313. [Google Scholar] [CrossRef]
- Polinski, J.M.; Harmon, S.L.; Henderson, K.J.; Barker, T.; Sussman, A.; Gagliano, N.J. Antibiotic stewardship in the retail clinic setting: Implementation in 1100 clinics nationwide. Healthcare 2017, 5, 89–91. [Google Scholar] [CrossRef]
- Patel, S.; Vasavada, H.; Damor, P.; Parmar, V. Impact of antibiotic stewardship strategy on the outcome of non-critical hospitalized children with suspected viral infection. Pediatr. Infect. Dis. 2016, 8, 103–106. [Google Scholar] [CrossRef]
- Sikkens, J.J.; van Agtmael, M.A.; Peters, E.J.G.; Lettinga, K.D.; van der Kuip, M.; Vandenbroucke-Grauls, C.M.J.E.; Wagner, C.; Kramer, M.H.H. Behavioral approach to appropriate antimicrobial prescribing in hospitals: The dutch unique method for antimicrobial stewardship (dumas) participatory intervention study. JAMA Intern. Med. 2017, 177, 1130–1138. [Google Scholar] [CrossRef]
- Thomas, M. Prescribing in A Rheumatology Clinic. 2005. Available online: https://www.pharmaceutical-journal.com/news-and-analysis/prescribing-in-a-rheumatology-clinic/10971435.article?firstPass=false (accessed on 17 January 2018).
- Wood, F.; Phillips, C.; Brookes-Howell, L.; Hood, K.; Verheij, T.; Coenen, S.; Little, P.; Melbye, H.; Godycki-Cwirko, M.; Jakobsen, K. Primary care clinicians’ perceptions of antibiotic resistance: A multi-country qualitative interview study. J. Antimicrob. Chemother. 2012, 68, 237–243. [Google Scholar] [CrossRef]
- Salsgiver, E.; Bernstein, D.; Simon, M.S.; Eiras, D.P.; Greendyke, W.; Kubin, C.J.; Mehta, M.; Nelson, B.; Loo, A.; Ramos, L.G. Knowledge, attitudes, and practices regarding antimicrobial use and stewardship among prescribers at acute-care hospitals. Infect. Control Hosp. Epidemiol. 2018, 39, 316–322. [Google Scholar] [CrossRef]
- Venugopalan, V.; Trustman, N.; Manning, N.; Hashem, N.; Berkowitz, L.; Hidayat, L. Administration of a survey to evaluate the attitudes of house staff physicians towards antimicrobial resistance and the antimicrobial stewardship programme at a community teaching hospital. J. Glob. Antimicrob. Resist. 2016, 4, 21–27. [Google Scholar] [CrossRef]
- Boyce, C.; Neale, P. Conducting in-depth interviews: A guide for designing and conducting in-depth interviews for evaluation input. In Monitoring and Evaluation; Pathfinder International: Watertown, MA, USA, 2006. [Google Scholar]
- Fox, N. Using Interviews in A Research Project; The NIHR RDS for the East Midlands/Yorkshire & the Humber; National Institute of Health Research: Bristol, UK, 2009. [Google Scholar]
- Provisional Summary Results of 6th Population and Housing Census-2017. 2017. Available online: https://web.archive.org/web/20171015113737/http://www.pbscensus.gov.pk/ (accessed on 23 October 2018).
- Pakistan: Provinces and Major Cities. 2018. Available online: http://www.citypopulation.de/Pakistan-100T.html (accessed on 24 December 2018).
- List of Hospitals in Lahore. Available online: https://en.wikipedia.org/wiki/List_of_hospitals_in_Lahore#cite_note-1 (accessed on 3 December 2018).
- Pulcini, C.; Gyssens, I.C. How to educate prescribers in antimicrobial stewardship practices. Virulence 2013, 4, 192–202. [Google Scholar] [CrossRef]
- Skodvin, B.; Aase, K.; Charani, E.; Holmes, A.; Smith, I. An antimicrobial stewardship program initiative: A qualitative study on prescribing practices among hospital doctors. Antimicrob. Resist. Infect. Control 2015, 4, 24. [Google Scholar] [CrossRef]
- Pakyz, A.L.; Moczygemba, L.R.; VanderWielen, L.M.; Edmond, M.B.; Stevens, M.P.; Kuzel, A.J. Facilitators and barriers to implementing antimicrobial stewardship strategies: Results from a qualitative study. Am. J. Infect. Control 2014, 42, S257–S263. [Google Scholar] [CrossRef]
- Johannsson, B.; Beekmann, S.E.; Srinivasan, A.; Hersh, A.L.; Laxminarayan, R.; Polgreen, P.M. Improving antimicrobial stewardship the evolution of programmatic strategies and barriers. Infect. Control Hosp. Epidemiol. 2011, 32, 367–374. [Google Scholar] [CrossRef]
- Cox, J.A.; Vlieghe, E.; Mendelson, M.; Wertheim, H.; Ndegwa, L.; Villegas, M.V.; Gould, I.; Levy Hara, G. Antibiotic stewardship in low- and middle-income countries: The same but different? Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2017, 23, 812–818. [Google Scholar] [CrossRef]
- García, C.; Llamocca, L.P.; García, K.; Jiménez, A.; Samalvides, F.; Gotuzzo, E.; Jacobs, J. Knowledge, attitudes and practice survey about antimicrobial resistance and prescribing among physicians in a hospital setting in Lima, Peru. BMC Clin. Pharmacol. 2011, 11, 18. [Google Scholar] [CrossRef]
- Md Rezal, R.S.; Hassali, M.A.; Alrasheedy, A.A.; Saleem, F.; Md Yusof, F.A.; Godman, B. Physicians’ knowledge, perceptions and behaviour towards antibiotic prescribing: A systematic review of the literature. Expert Rev. Anti-Infect. Ther. 2015, 13, 665–680. [Google Scholar] [CrossRef]
- Palinkas, L.A.; Horwitz, S.M.; Green, C.A.; Wisdom, J.P.; Duan, N.; Hoagwood, K. Purposeful Sampling for Qualitative Data Collection and Analysis in Mixed Method Implementation Research. ADM Policy Ment. Health 2015, 42, 533–544. [Google Scholar] [CrossRef]
- Guest, G.; MacQueen, K.M.; Namey, E.E. Applied Thematic Analysis, 1st ed.; SAGE: New York, NY, USA, 2011. [Google Scholar]
- Sorensen, T.D.; Pestka, D.; Sorge, L.A.; Wallace, M.L.; Schommer, J. A qualitative evaluation of medication management services in six Minnesota health systems. Am. J. Health Syst. Pharm. 2016, 73, 307–314. [Google Scholar] [CrossRef]
- Lee, M.S.; Ray, K.N.; Mehrotra, A.; Giboney, P.; Yee, H.F.; Barnett, M.L. Primary care practitioners’ perceptions of electronic consult systems: A qualitative analysis. JAMA Intern. Med. 2018, 178, 782–789. [Google Scholar] [CrossRef]
- Saunders, B.; Sim, J.; Kingstone, T.; Baker, S.; Waterfield, J.; Bartlam, B.; Burroughs, H.; Jinks, C. Saturation in qualitative research: Exploring its conceptualization and operationalization. Qual. Quant. 2018, 52, 1893–1907. [Google Scholar] [CrossRef]
- Curry, L.A.; Nembhard, I.M.; Bradley, E.H. Qualitative and mixed methods provide unique contributions to outcomes research. Circulation 2009, 119, 1442–1452. [Google Scholar] [CrossRef]
- Islam, Z. 80,000 Quacks Operating in Karachi. 2011. Available online: https://www.thenews.com.pk/archive/print/298552-%E2%80%9880000-quacks-operating-in-karachi%E2%80%99 (accessed on 25 October 2018).
- Warraich, S. Curing the Quacks. 2018. Available online: http://tns.thenews.com.pk/curing-quacks/ (accessed on 24 October 2018).
- World Antibiotic Awareness Week: Are Over-The-Counter Antibiotics Even Safe for Your Health? 2017. Available online: https://www.pakistantoday.com.pk/2017/11/19/world-antibiotic-awareness-week-are-over-the-counter-antibiotics-even-safe-for-your-health/ (accessed on 28 October 2018).
- Hussnain, F. Punjab Plagued with 80,000 Quacks, SC Told. 2018. Available online: https://nation.com.pk/15-Apr-2018/punjab-plagued-with-80-000-quacks-sc-told (accessed on 24 October 2018).
- Ayukekbong, J.A.; Ntemgwa, M.; Atabe, A.N. The threat of antimicrobial resistance in developing countries: Causes and control strategies. Antimicrob. Resist. Infect. Control 2017, 6, 47. [Google Scholar] [CrossRef] [PubMed]
- Sakeena, M.; Bennett, A.A.; McLachlan, A.J. Enhancing pharmacists’ role in developing countries to overcome the challenge of antimicrobial resistance: A narrative review. Antimicrob. Resist. Infect. Control 2018, 7, 63. [Google Scholar] [CrossRef] [PubMed]
- Sutthiruk, N.; Considine, J.; Hutchinson, A.; Driscoll, A.; Malathum, K.; Botti, M. Thai clinicians’ attitudes toward antimicrobial stewardship programs. Am. J. Infect. Control 2018, 46, 425–430. [Google Scholar] [CrossRef]
- PMDC Curriculum of M.B.B.S. 2011. Available online: http://umr.prime.edu.pk/files/PMDC_Curriculum_2011.pdf (accessed on 24 October 2018).
- Kumar, S.; Bano, S. Comparison and Analysis of Health Care Delivery Systems: Pakistan versus Bangladesh. J. Hosp. Med. Manag. 2017, 3, 1–7. [Google Scholar] [CrossRef]
- Despite a Growth of 25% between 2006 to 2015 in MBBS Doctors in Punjab, Doctor Patient Ratio Remains Alarmingly Low and Unable to Keep up with Population Growth: Gallup Pakistan Big Analytics Team. 2018. Available online: http://gallup.com.pk/despite-a-growth-of-25-between-2006-to-2015-in-mbbs-doctors-in-punjab-doctor-patient-ratio-remains-alarmingly-low-and-unable-to-keep-up-with-population-growth-gallup-pakistan-big-analytics-team/ (accessed on 29 October 2018).
- Patel, S.J.; Saiman, L. Principles and Strategies of Antimicrobial Stewardship in the Neonatal Intensive Care Unit. Semin. Perinatol. 2012, 36, 431–436. [Google Scholar] [CrossRef] [Green Version]
- Cook, P.P.; Gooch, M. Long-term effects of an antimicrobial stewardship programme at a tertiary-care teaching hospital. Int. J. Antimicrob. Agents 2015, 45, 262–267. [Google Scholar] [CrossRef]
- Bannan, A.; Buono, E.; McLaws, M.L.; Gottlieb, T. A survey of medical staff attitudes to an antibiotic approval and stewardship programme. Intern. Med. J. 2009, 39, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Broom, J.; Broom, A.; Plage, S.; Adams, K.; Post, J.J. Barriers to uptake of antimicrobial advice in a UK hospital: A qualitative study. J. Hosp. Infect. 2016, 93, 418–422. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Total n (%) |
|---|---|
| Age (years) | |
| 20–30 | 4 (18.18) |
| 31–40 | 9 (40.91) |
| 41–50 | 7 (31.82) |
| >50 | 2 (9.09) |
| Gender | |
| Male | 17 (77.27) |
| Female | 5 (22.73) |
| Experience (years) | |
| 1–5 | 3 (13.64) |
| 6–10 | 7 (31.82) |
| 11–15 | 2 (9.09) |
| 16–20 | 8 (36.36) |
| >20 | 2 (9.09) |
| Education | |
| MBBS 1 | 10 (45.45) |
| FCPS 2 | 12 (54.55) |
| Nationality | |
| Pakistani | 22 (100) |
| Hospital departments | |
| Medicine | 11 (50) |
| Surgery | 6 (27.27) |
| Obstetrics & Gynecology | 5 (22.73) |
| Frequency of antibiotic prescribing/day | |
| 6–10 prescription | 6 (27.27) |
| >10 prescriptions | 16 (72.73) |
| Bed capacity of hospitals (n = 7) | |
| <1000 | 2 (28.57) |
| 1000 to 1500 | 4 (57.14) |
| >1500 | 1 (14.29) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayat, K.; Rosenthal, M.; Gillani, A.H.; Zhai, P.; Aziz, M.M.; Ji, W.; Chang, J.; Hu, H.; Fang, Y. Perspective of Pakistani Physicians towards Hospital Antimicrobial Stewardship Programs: A Multisite Exploratory Qualitative Study. Int. J. Environ. Res. Public Health 2019, 16, 1565. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091565
Hayat K, Rosenthal M, Gillani AH, Zhai P, Aziz MM, Ji W, Chang J, Hu H, Fang Y. Perspective of Pakistani Physicians towards Hospital Antimicrobial Stewardship Programs: A Multisite Exploratory Qualitative Study. International Journal of Environmental Research and Public Health. 2019; 16(9):1565. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091565
Chicago/Turabian StyleHayat, Khezar, Meagen Rosenthal, Ali Hassan Gillani, Panpan Zhai, Muhammad Majid Aziz, Wenjing Ji, Jie Chang, Hao Hu, and Yu Fang. 2019. "Perspective of Pakistani Physicians towards Hospital Antimicrobial Stewardship Programs: A Multisite Exploratory Qualitative Study" International Journal of Environmental Research and Public Health 16, no. 9: 1565. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091565