The Effect of Long Working Hours and Overtime on Occupational Health: A Meta-Analysis of Evidence from 1998 to 2018


Abstract
:1. Introduction
1.1. Cardiovascular and Cerebrovascular Diseases
1.2. Hypertension
1.3. Diabetes Mellitus
1.4. Depression and Anxiety
1.5. Work Stress
1.6. Health Behaviours
1.7. Sleep and Fatigue
1.8. Occupational Injury
1.9. Aim of the Study
2. Methods
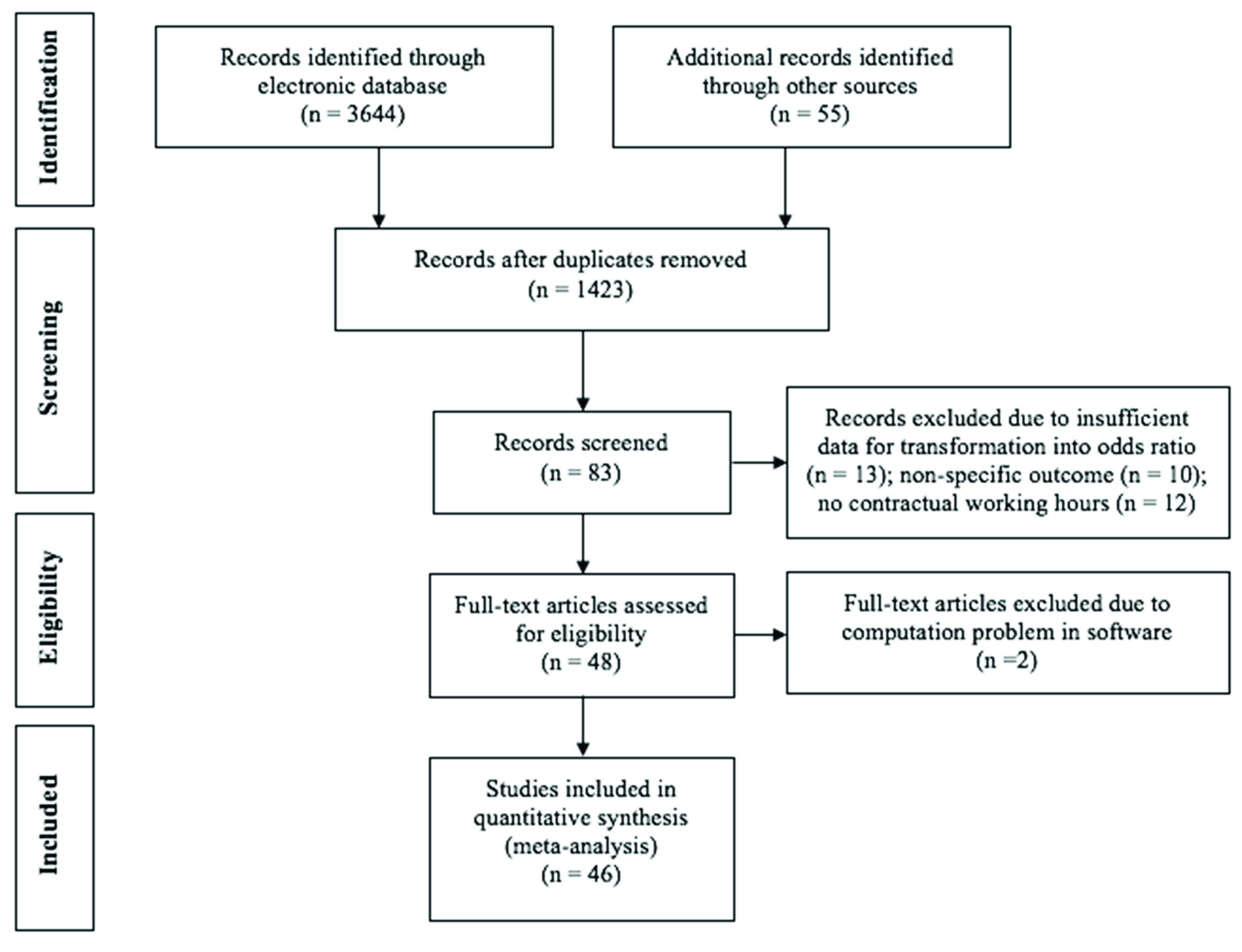
2.1. Literature Search and Selection
2.2. Coding Procedures
2.3. Meta-Analysis
3. Results
3.1. Characteristics of Selected Papers
3.2. Random-Effects Model of Long Working Hours and Occupational Health Conditions
3.3. Moderator Analysis
4. Discussion
4.1. The Effects of Long Working Hours on Sleep, Fatigue and Injuries
4.2. Effects of Moderators
4.3. Comparison of Previous Meta-Analysis
4.4. Theoretical Implications
4.5. Practical Implications
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Occupational Health: A Manual for Primary Health Care Workers; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Lee, S.; McCann, D.; Messenger, J.C. Working Time Around the World. Trend in Working Hours, Laws and Policies in a Global Comparative Perspective; International Labour Office: Geneva, Switzerland, 2007. [Google Scholar]
- Bannai, A.; Tamakoshi, A. The association between long working hours and health: A systematic review of epidemiological evidence. Scand. J. Work Environ. Health 2014, 40, 5–18. [Google Scholar] [CrossRef]
- Liu, Y.; Tanaka, H. Overtime work, insufficient sleep, and risk of non-fatal acute myocardial infarction in Japanese men. Occup. Environ. Med. 2002, 59, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Sparks, K.; Cooper, C.; Fried, Y.; Shirom, A. The effects of hours of work on health: A meta-analytic review. J. Occup. Organ. Psychol. 1997, 70, 391–408. [Google Scholar] [CrossRef]
- Uehata, T. Long working hours and occupational stress-related cardiovascular attacks among middle-aged workers in Japan. J. Hum. Ergol. 1991, 20, 147–153. [Google Scholar]
- White, J.; Beswick, J. Working Long Hours; Health and Safety Laboratory: Sheffield, UK, 2003. [Google Scholar]
- Artazcoz, L.; Cortès, I.; Escribà-Agüir, V.; Cascant, L.; Villegas, R. Understanding the relationship of long working hours with health status and health-related behaviours. J. Epidemiol. Community Health 2009, 63, 521–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukuoka, Y.; Dracup, K.; Froelicher, E.S.; Ohno, M.; Hirayama, H.; Shiina, H.; Kobayashi, F. Do Japanese workers who experience an acute myocardial infarction believe their prolonged working hours are a cause? Int. J. Cardiol. 2005, 100, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Grosch, J.W.; Caruso, C.C.; Rosa, R.R.; Sauter, S.L. Long hours of work in the US: Associations with demographic and organizational characteristics, psychosocial working conditions, and health. Am. J. Ind. Med. 2006, 49, 943–952. [Google Scholar] [CrossRef]
- Lallukka, T.; Lahelma, E.; Rahkonen, O.; Roos, E.; Laaksonen, E.; Martikainen, P.; Head, J.; Brunner, E.; Mosdol, A.; Marmot, M.; et al. Associations of job strain and working overtime with adverse health behaviors and obesity: Evidence from the Whitehall II Study, Helsinki Health Study, and the Japanese Civil Servants Study. Soc. Sci. Med. 2008, 66, 1681–1698. [Google Scholar] [CrossRef]
- Kim, W.; Park, E.C.; Lee, T.H.; Kim, T.H. Effect of working hours and precarious employment on depressive symptoms in South Korean employees: A longitudinal study. Occup. Environ. Med. 2016, 73, 816–822. [Google Scholar] [CrossRef]
- Cheng, Y.; Du, C.L.; Hwang, J.J.; Chen, I.S.; Chen, M.F.; Su, T.C. Working hours, sleep duration and the risk of Acute Coronary Heart Disease: A case-control study of middle aged men in Taiwan. Int. J. Cardiol. 2014, 171, 419–422. [Google Scholar] [CrossRef]
- Lunde, L.-K.; Koch, M.; Veiersted, K.B.; Moen, G.-H.; Wærsted, M.; Knardahl, S. Heavy physical work: Cardiovascular load in male construction workers. Int. J. Environ. Res. Public Health 2016, 13, 356. [Google Scholar]
- Kim, I.S.; Ryu, S.C.; Kim, Y.H.; Kwon, Y.J. Influencing factors in approving cerebrovascular and cardiovascular disease as work-related disease of workers’ in manufacturing sectors. Korean J. Occup. Environ. Med. 2012, 24, 158–166. [Google Scholar]
- Skogstad, M.; Mamen, A.; Lunde, L.-K.; Ulvestad, B.; Matre, D.; Aass, H.C.D.; Øvstebø, R.; Nielsen, P.; Samuelsen, K.N.; Skare, Ø.; et al. Shift work including night work and long working hours in industrial plants increases the risk of atherosclerosis. Int. J. Environ. Res. Public Health 2019, 16, 521. [Google Scholar] [CrossRef] [PubMed]
- Sokejima, S.; Kagamimori, S. Working hours as a risk factor for acute myocardial infarction in Japan: Case-control study. BMJ 1998, 317, 775–780. [Google Scholar] [CrossRef] [PubMed]
- Spurgeon, A.; Harringtion, J.M.; Cooper, C.L. Health and safety problems associated with long working hours: A review of the current position. Occup. Environ. Med. 1997, 54, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, M.; Heikkilä, K.; Jokela, M.; Ferrie, J.E.; Batty, G.D.; Vahtera, J.; Kivimäki, M. Long working hours and Coronary Heart Disease: A systematic review and meta-analysis. Am. J. Epidemiol. 2012, 176, 586–596. [Google Scholar] [CrossRef] [PubMed]
- Netterstrøm, B.; Kristensen, T.S.; Jensen, G.; Schnor, P. Is the demand-control model still a usefull tool to assess work-related psychosocial risk for ischemic heart disease? Results from 14 year follow up in the Copenhagen City heart study. Int. J. Occup. Med. Environ. Health 2010, 23, 217–524. [Google Scholar] [CrossRef]
- Kang, M.Y.; Park, H.; Seo, J.C.; Kim, D.; Lim, Y.H.; Lim, S.; Cho, S.H.; Hong, Y.C. Long working hours and cardiovascular disease. A meta-analysis of epidemiologic studies. J. Occup. Environ. Med. 2012, 54, 532–537. [Google Scholar] [CrossRef]
- Kivimäki, M.; Jokela, M.; Singh-Manoux, A.; Fransson, E.I.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Burr, H.; Casini, A.; Clays, E.; et al. Long working hours and risk of coronary heart disease and stroke: A systematic review and meta-analysis of published and unpublished data for 603,838 individuals. Lancet 2015, 386, 1739–1746. [Google Scholar] [CrossRef]
- Iwasaki, K.; Sasaki, T.; Oka, T.; Hisanaga, N. Effect of working hours on biological functions related to cardiovascular system among salesmen in a machinery manufacturing company. Ind. Health 1998, 36, 361–367. [Google Scholar] [CrossRef]
- Nakanishi, N.; Yoshida, H.; Nagano, K.; Kawashimo, H.; Nakamura, K.; Tatara, K. Long working hours and risk for hypertension in Japanese male white collar workers. J. Epidemiol. Community Health 2001, 55, 316–322. [Google Scholar] [CrossRef] [Green Version]
- Pimenta, A.M.; Beunza, J.J.; Bes-Rastrollo, M.; Alonso, A.; López, C.N.; Velásquez-Meléndez, G.; Martínez-González, M.A. Work hours and incidence of hypertension among Spanish University graduates: The Seguimiento Universidad de Navarra prospective cohort. J. Hypertens. 2009, 27, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Tarumi, K.; Hagihara, A.; Morimoto, K. A prospective observation of onsets of health defects associated with working hours. Ind. Health 2003, 41, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Schnall, P.L.; Jauregui, M.; Su, T.C.; Baker, D. Work hours and self-reported hypertension among working people in California. Hypertension 2006, 48, 744–750. [Google Scholar] [CrossRef]
- Kawakami, N.; Takatsuka, N.; Shimizu, H.; Ishibashi, H. Depressive symptoms and occurrence of type 2 diabetes among Japanese men. Diabetes Care 1999, 22, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, N.; Nishina, K.; Yoshida, H.; Matsuo, Y.; Nagano, K.; Nakamura, K.; Suzuki, K.; Tatara, K. Hours of work and the risk of developing impaired fasting glucose or type 2 diabetes mellitus in Japanese male office workers. Occup. Environ. Med. 2001, 58, 569–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afonso, P.; Fonseca, M.; Pires, J.F. Impact of working hours on sleep and mental health. Occup. Med. 2017, 67, 377–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amagasa, T.; Nakayama, T. Relationship between long working hours and depression: A 3-year longitudinal study of clerical workers. J. Occup. Environ. Med. 2013, 55, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, R.; Seo, E.; Maeno, T.; Ito, M.; Sanuki, M.; Maeno, T. The relationship between long working hours and depression among first-year residents in Japan. BMC Med. Educ. 2018, 18, 50. [Google Scholar] [CrossRef]
- Shields, M. Long Working Hours and Health; Statistics Canada: Ottawa, ON, Canada, 1999; Volume 11, p. 33.
- Virtanen, M.; Ferrie, J.E.; Singh-Manoux, A.; Shipley, M.J.; Stansfeld, S.A.; Marmot, M.G.; Ahola, K.; Vahtera, J.; Kivimäki, M. Long working hours and symptoms of anxiety and depression: A 5-year follow-up of the Whitehall II study. Psychol. Med. 2011, 41, 2485–2494. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.C. Age differences in work stress, exhaustion, well-being, and related factors from an ecological perspective. Int. J. Environ. Res. Public Health 2019, 16, 50. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Suh, C.; Kim, J.E.; Park, J.O. The impact of long working hours on psychosocial stress response among white-collar workers. Ind. Health 2017, 55, 46–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruyama, S.; Morimoto, K. Effects of long workhours on life-style, stress and quality of life among intermediate Japanese managers. Scand. J. Work Environ. Health 1996, 22, 353–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, Y.; Miyake, H.; Thériault, G. Overtime work and stress response in a group of Japanese workers. Occup. Med. 2009, 59, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Kageyam, T.; Nishikido, N.; Kobayashi, T.; Kurokawa, Y.; Kaneko, T.; Kabuto, M. Long commuting time, extensive overtime, and sympathodominant state assessed in terms of short-term heart rate variability among male white-collar workers in the Tokyo megalopolis. Ind. Health 1998, 36, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Mizoue, T.; Reijula, K.; Andersson, K. Environmental tobacco smoke exposure and overtime work as risk factors for sick building syndrome in Japan. Am. J. Epidemiol. 2001, 154, 803–808. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, Y.; Chung, H.K.; Hisanaga, N. Long working hours and subjective fatigue symptoms. Ind. Health 2001, 39, 250–254. [Google Scholar] [CrossRef]
- Sato, K.; Hayashino, Y.; Yamazaki, S.; Takegami, M.; Ono, R.; Otani, K.; Konno, S.; Kikuchi, S.; Fukuhara, S. Headache prevalence and long working hours: The role of physical inactivity. Public Health 2012, 126, 587–593. [Google Scholar] [CrossRef] [Green Version]
- Otsuka, Y.; Tatemaru, M. Working hours and psychological health among Japanese restaurant services workers. Int. J. Psychol. Couns. 2010, 2, 65–71. [Google Scholar]
- Colten, H.R.; Altevogt, B.M. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem; National Academies Press: Washington, WA, USA, 2006. [Google Scholar]
- Hoevenaar-Blom, M.P.; Spijkerman, A.M.; Kromhout, D.; Verschuren, W.M. Sufficient sleep duration contributes to lower cardiovascular disease risk in addition to four traditional lifestyle factors: The MORGEN study. Eur. J. Prev. Cardiol. 2014, 21, 1367–1375. [Google Scholar] [CrossRef]
- Nagai, M.; Hoshide, S.; Kario, K. Sleep duration as a risk factor for cardiovascular disease—A review of the recent literature. Curr. Cardiol. Rev. 2010, 6, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, M.; Morikawa, Y.; Sakurai, M.; Nakamura, K.; Miura, K.; Ishizaki, M.; Kido, T.; Naruse, Y.; Suwazono, Y.; Nakagawa, H. Association between long working hours and sleep problems in white-collar workers. J. Sleep Res. 2011, 20, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, M.; Ferrie, J.E.; Gimeno, D.; Vahtera, J.; Elovainio, M.; Singh-Manoux, A. Long working hours and sleep disturbances: The Whitehall II prospective cohort study. Sleep 2009, 32, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Dembe, A.E.; Erickson, J.B.; Delbos, R.G.; Banks, S.M. The impact of overtime and long work hours on occupational injuries and illnesses: New evidence from the United States. Occup. Environ. Med. 2005, 62, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Lowery, J.T.; Borgerding, J.A.; Zhen, B.; Glazner, J.E.; Bondy, J.; Kreiss, K. Risk factors for injury among construction workers at Denver International Airport. Amer. J. Ind. Med 1998, 34, 113–120. [Google Scholar] [CrossRef]
- Simpson, C.L.; Severson, R.K. Risk of injury in African American hospital workers. J. Occup. Environ. Med. 2000, 42, 1035–1040. [Google Scholar] [CrossRef] [PubMed]
- Burke, R.J.; Cooper, C.L. (Eds.) The Long Work Hours Culture: Causes, Consequences and Choices; Emerald Group Publishing Limited: Bingley, UK, 2008. [Google Scholar]
- Monet. Working to Death in China: A Look at the Nation with the Highest Instance of Death from Overwork in the World. The Diplomat. 26 March 2014. Available online: https://thediplomat.com/2014/03/working-to-death-in-china/ (accessed on 13 June 2018).
- Burger, A.S. Extreme Working Hours in Western Europe and North America: A New Aspect of Polarization. The London School of Economics and Political Science No. 92, 52. 2015. Available online: http://www.lse.ac.uk/europeanInstitute/LEQS%20Discussion%20Paper%20Series/LEQSPaper92.pdf (accessed on 13 June 2018).
- Virtanen, M.; Jokela, M.; Nyberg, S.T.; Madsen, I.E.; Lallukka, T.; Ahola, K.; Alfredsson, L.; Batty, G.D.; Bjorner, J.B.; Borritz, M.; et al. Long working hours and alcohol use: Systematic review and meta-analysis of published studies and unpublished individual participant data. BMJ 2015, 350, g7772. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.J.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E. Socioeconomic inequalities in health in 22 European countries. N. Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef] [PubMed]
- Ravesteijn, B.; van Kippersluis, H.; van Doorslaer, E. The Contribution of Occupation to Health Inequality; Emerald Group Publishing Limited: Bentley, UK, 2013; Volume 21, pp. 311–332. [Google Scholar]
- Akerstedt, T.; Knutsson, A.; Westerholm, P.; Theorell, T.; Alfredsson, L.; Kecklund, G. Sleep disturbances, work stress and work hours: A cross-sectional study. J. Psychosom. Res. 2002, 53, 741–748. [Google Scholar] [CrossRef]
- Beckers, D.G.; van der Linden, D.; Smulders, P.G.; Kompier, M.A.; van Veldhoven, M.J.; van Yperen, N.W. Working overtime hours: Relations with fatigue, work motivation, and the quality of work. J. Occup. Environ. Med. 2004, 46, 1282–1289. [Google Scholar]
- Jeon, S.H.; Leem, J.H.; Park, S.G.; Heo, Y.S.; Lee, B.J.; Moon, S.H.; Jung, D.Y.; Kim, H.C. Association among working hours, occupational stress, and presenteeism among wage workers: Results from the second Korean working conditions survey. Anna. Occup. Environ. Med. 2014, 26, 6. [Google Scholar] [CrossRef] [PubMed]
- MHCNSW. Physical Health and Mental Wellbeing. 2016. Available online: https://nswmentalhealthcommission.com.au/sites/default/files/publication-documents/Physical%20health%20and%20wellbeing%20-%20final%208%20Apr%202016%20WEB.pdf (accessed on 8 May 2018).
- Van Achterberg, T.; Huisman-de Waal, G.G.; Ketelaar, N.A.; Oostendorp, R.A.; Jacobs, J.E.; Wollersheim, H.C. How to promote healthy behaviours in patients? An overview of evidence for behaviour change techniques. Health Promot. Int. 2010, 26, 148–162. [Google Scholar] [CrossRef] [Green Version]
- Conner, M.; Norman, P. Health behaviour: Current issues and challenges. Psychol. Health 2017, 32, 895–906. [Google Scholar] [CrossRef] [Green Version]
- Wirtz, A.; Lombardi, D.A.; Willetts, J.L.; Folkard, S.; Christiani, D.C. Gender differences in the effect of weekly working hours on occupational injury risk in the United States working population. Scand. J. Work Environ. Health 2012, 38, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutherland, V.J.; Cooper, C.L. Stress and Accidents in the Offshore Oil and Gas Industry; Gulf Publishing Company: Houston, TX, USA, 1991. [Google Scholar]
- Wan, J.J.; Morabito, D.J.; Khaw, L.; Knudson, M.M.; Dicker, R.A. Mental illness as an independent risk factor. J. Trauma 2006, 61, 1299–1304. [Google Scholar] [CrossRef] [PubMed]
- Clarke, P.; Crawford, C.; Steele, F.; Vignoles, A. The Choice Between Fixed and Random Effects Models: Some Considerations for Educational Research. IZA Discussion Paper No. 5287. 2010. Available online: http://ftp.iza.org/dp5287.pdf (accessed on 11 June 2019).
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
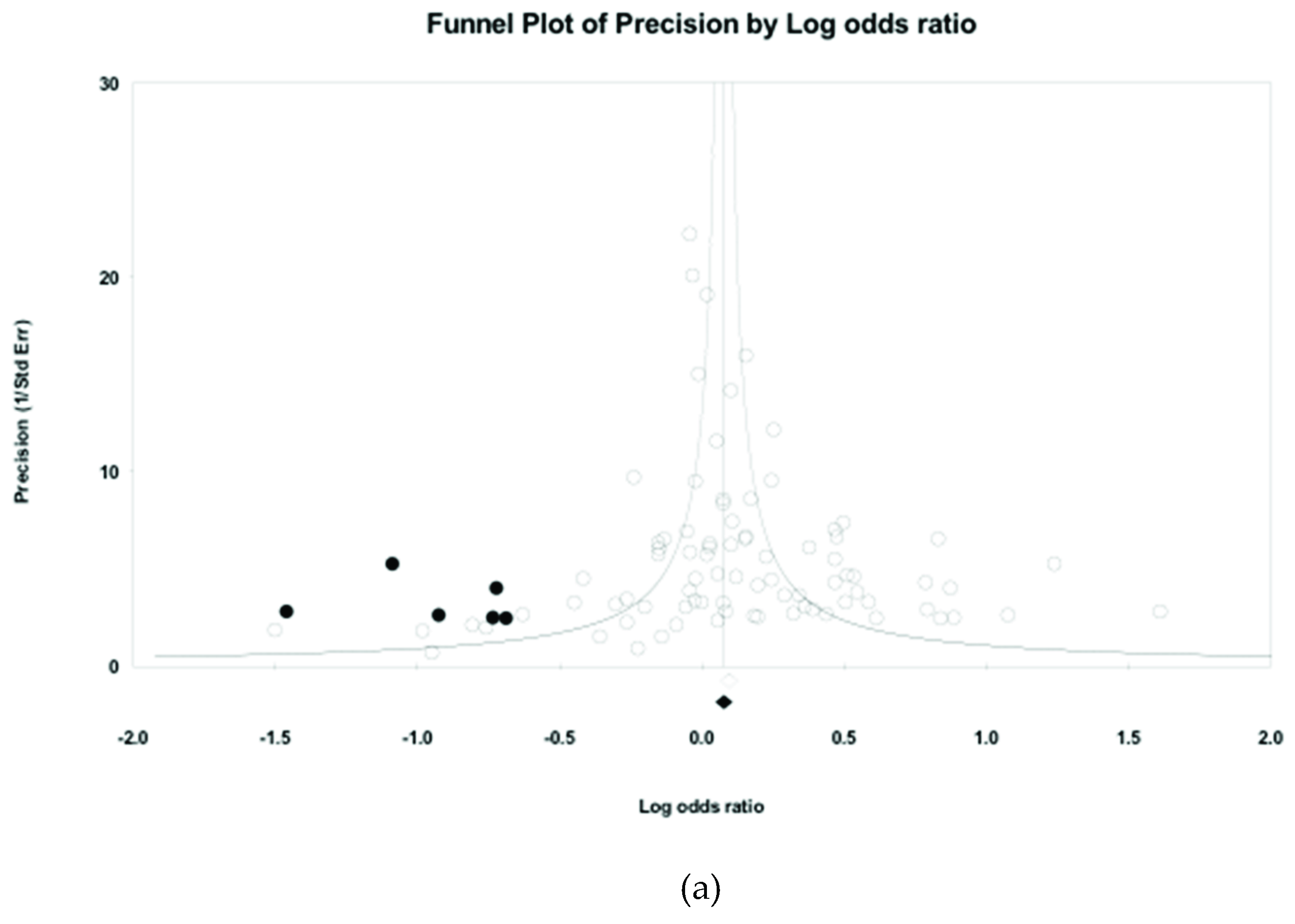
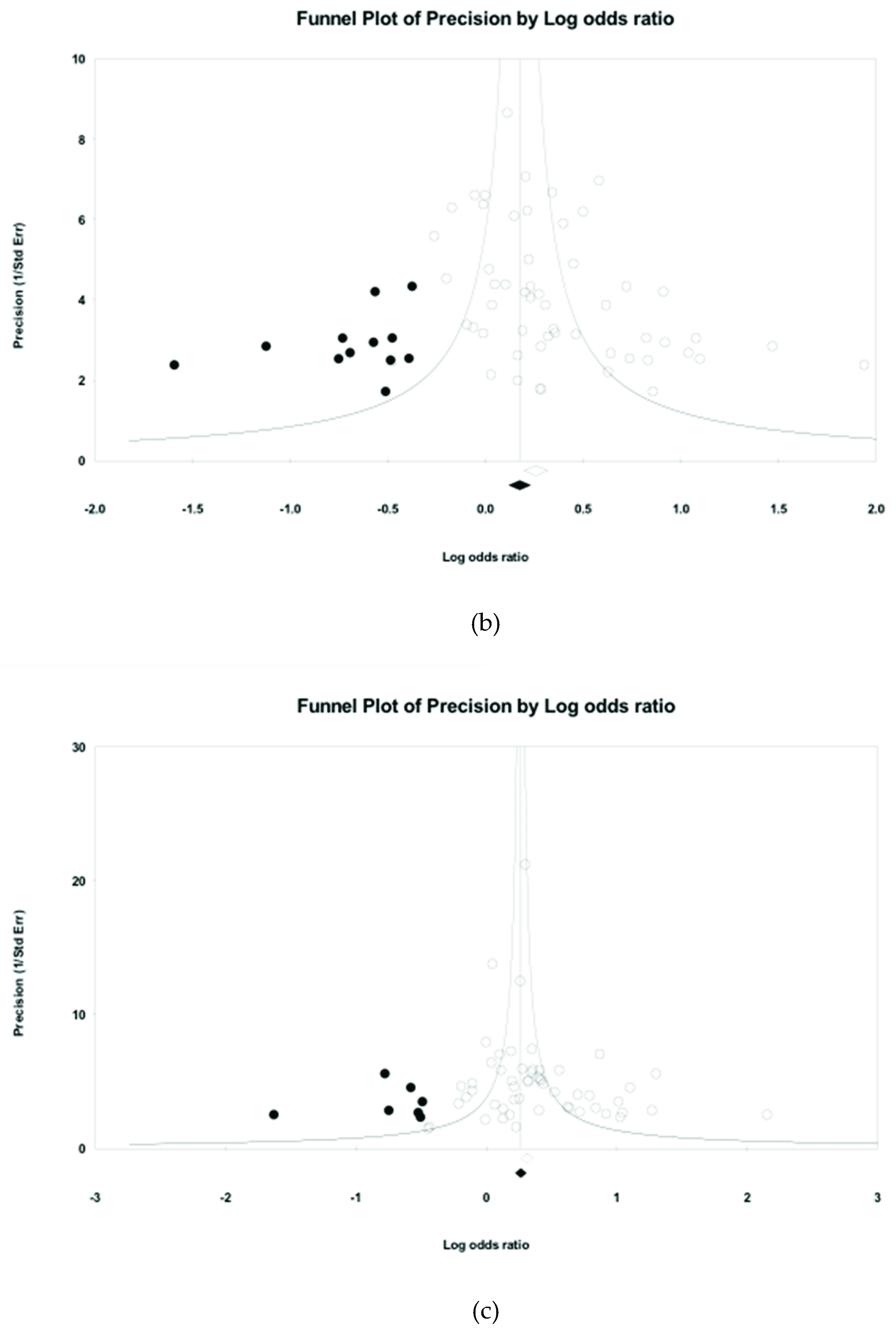
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Borenstein, M.; Higgin, J.P. Meta-analysis and subgroups. Prev. Sci. 2013, 14, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.D.; Cheng, T.J.; Lin, Y.C.; Hsiao, S.T. Job categories and acute ischemic heart disease: A hospital-based, case-control study in Taiwan. Am. J. Ind. Med. 2007, 50, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Tomioka, K.; Morita, N.; Saeki, K.; Okamoto, N.; Kurumatani, N. Working hours, occupational stress and depression among physicians. Occup. Med. 2011, 61, 163–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kivimäki, M.; Virtanen, M.; Kawachi, I.; Nyberg, S.T.; Alfredsson, L.; Batty, G.D.; Bjorner, J.B.; Borritz, M.; Brunner, E.J.; Burr, H.; et al. Long working hours, socioeconomic status, and the risk of incident type 2 diabetes: A meta-analysis of published and unpublished data from 222,120 individuals. Lancet 2015, 3, 27–34. [Google Scholar]
- O’ Reilly, D.; Rosato, M. Worked to death? A census-based longitudinal study of the relationship between the numbers of hours spent working and mortality risk. Int. J. Epidemiol. 2013, 42, 1820–1830. [Google Scholar] [CrossRef] [PubMed]
- Tayama, J.; Li, J.; Munakata, M. Working long hours is associated with higher prevalence of diabetes in urban male Chinese workers: The rosai karoshi study. Stress Health 2014, 32, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Ohtsu, T.; Kaneita, Y.; Aritake, S.; Mishima, K.; Uchiyama, M.; Akashiba, T.; Uchimura, N.; Nakaji, S.; Munezawa, T.; Kokaze, A.; et al. A cross-sectional study of the association between working hours and sleep duration among the Japanese working population. J. Occup. Health 2013, 4, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Basner, M.; Fomberstein, K.M.; Razavi, F.M.; Banks, S.; William, J.H.; Rosa, R.R.; Dinges, D.F. American time use survey: Sleep time and its relationship to waking activities. Sleep 2007, 30, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Burazeri, G.; Gofin, J.; Kark, J.D. Over 8 hours of sleep—marker of increased mortality in Mediterranean population: Follow-up population study. Croat. Med. J. 2003, 44, 193–198. [Google Scholar]
- Krueger, P.M.; Friedman, E.M. Sleep duration in the United States: A cross-sectional population-based study. Am. J. Epidemiol. 2009, 169, 1052–1063. [Google Scholar] [CrossRef]
- Bianchi, S.M. Maternal employment and time with children: Dramatic change or surprising continuity? Demography 2000, 37, 410–414. [Google Scholar] [CrossRef]
- Sayer, L.C. Gender, time and inequality: Trends in women’s and men’s paid work, unpaid work and free time. Soc. Forces 2005, 84, 285–303. [Google Scholar] [CrossRef]
- Ropponen, A.; Härmä, M.; Bergbom, B.; Nätti, J.; Sallinen, M. The vicious circle of working hours, sleep, and recovery in expert work. Int. J. Environ. Res. Public Health 2018, 15, 1361. [Google Scholar] [CrossRef] [PubMed]
- Heslop, P.; Smith, G.D.; Metcalfe, C.; Macleod, J.; Hart, C. Sleep duration and mortality: The effect of short or long sleep duration on cardiovascular and all-cause mortality in working men and women. Sleep Med. 2002, 3, 305–314. [Google Scholar] [CrossRef]
- Ayas, N.T.; White, D.P.; Manson, J.E.; Stampfer, M.J.; Speizer, F.E.; Malhotra, A.; Hu, F.B. A prospective study of sleep duration and coronary heart disease in women. Arch. Intern. Med. 2003, 163, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Chandola, T.; Ferrie, J.E.; Perski, A.; Akbaraly, T.; Marmot, M.G. The effect of short sleep duration on coronary heart disease risk is greatest among those with sleep disturbance: A prospective study from the Whitehall II cohort. Sleep 2010, 33, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Cizza, G.; Skarulis, M.; Mignot, E. A link between short sleep and obesity: Building the evidence for causation. Sleep 2005, 28, 1217–1220. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, K.; Tasali, E.; Leproult, R.; Van Cauter, E. Effects of poor and short sleep on glucose metabolism and obesity risk. Nat. Rev. Endocrinol 2009, 5, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Stranges, S.; Cappuccio, F.P.; Kandala, N.B.; Miller, M.A.; Taggart, F.M.; Kumari, M.; Ferrie, J.E.; Shipley, M.J.; Brunner, E.J.; Marmot, M.G. Cross-sectional versus prospective associations of sleep duration with changes in relative weight and body fat distribution: The Whitehall II study. Amer. J. Epidemiol. 2008, 167, 321–329. [Google Scholar] [CrossRef]
- Gangwisch, J.E.; Heymsfield, S.B.; Boden-Albala, B.; Buijs, R.M.; Kreier, F.; Pickering, T.G.; Rundle, A.G.; Zammit, G.K.; Malasphina, D. Short sleep duration as a risk factor for hypertension. Hypertension 2006, 47, 833–839. [Google Scholar] [CrossRef]
- Knutson, K.L.; Ryden, A.M.; Mander, B.A.; Van Cauter, E. Role of sleep duration and quality in the risk and severity of type 2 diabetes mellitus. Arch. Intern. Med. 2006, 166, 1768–1774. [Google Scholar] [CrossRef]
- Yaggi, H.K.; Araujo, A.B.; McKinlay, J.B. Sleep duration as a risk factor for the development of type 2 diabetes. Diabetes Care 2006, 29, 657–661. [Google Scholar] [CrossRef]
- Gandi, J.C.; Wai, P.S.; Karick, H.; Dagona, Z.K. The role of stress and level of burnout in job performance among nurses. Mental Health Fam. Med. 2011, 8, 181–194. [Google Scholar]
- Pan, G. The effects of burnout on task performance and turnover intention of new generation of skilled workers. JHRSS 2017, 5, 156–166. [Google Scholar] [CrossRef]
- Ritacco, G.; Jamkome, P.K.; Mangori, M. The impact of stress and burnout on employees’ performance at botswana power corporation. Int. J. Contemp. Res. 2013, 5, 795–824. [Google Scholar]
- Shamsafrouz, H.; Haghverdi, H. The effect of burnout on teaching performance of male and female EFL teachers in L2 context. IJFLTR 2015, 3, 47–58. [Google Scholar]
- Cormier, R.E. Sleep Disturbances. Clinical Methods: The History, Physical, and Laboratory Examinations, 3rd ed.; Butterworths: Boston, UK, 1990. [Google Scholar]
- Krystal, A.D.; Thakur, M.; Roth, T. Sleep disturbance in psychiatric disorders: Effects on function and quality of life in mood disorders, alcoholism, and schizophrenia. Ann. Clin. Psycharity 2008, 20, 39–46. [Google Scholar] [CrossRef]
- Rumble, M.E.; White, K.H.; Benca, R.M. Sleep Disturbances in Mood Disorders. Psychiatr. Clin. 2015, 38, 743–759. [Google Scholar]
- Medic, G.; Wille, M.; Hemels, M.E.H. Short-and Long-Term Health Consequences of Sleep Disruption. Nat. Sci. Sleep 2017, 9, 151–161. [Google Scholar] [CrossRef]
- Caruso, C.C. Negative impacts of shiftwork and long work hours. Rehabil. Nurs. 2014, 39, 16–25. [Google Scholar] [CrossRef]
- Shin, K.S.; Chung, Y.K.; Kwon, Y.J.; Son, J.S.; Lee, S.H. The effect of long working hours on cerebrovascular and cardiovascular disease; A case-crossover study. Am. J. Ind. Med. 2017, 60, 753–761. [Google Scholar] [CrossRef]
- Yu, J. Relationship Between Long Working Hours and Metabolic Syndrome Among Korean Workers. Asian Nurs. Res. 2017, 11, 36–41. [Google Scholar] [CrossRef] [Green Version]
- Son, M.; Kong, J.O.; Koh, S.B.; Kim, J.; Härmä, M. Effects of long working hours and the night shift on severe sleepiness among workers with 12-hour shift systems for 5 to 7 consecutive days in the automobile factories of Korea. J. Sleep Res. 2008, 17, 385–394. [Google Scholar] [CrossRef]
- Lombardi, D.A.; Folkard, S.; Willetts, J.L.; Smith, G.S. Daily sleep, weekly working hours, and risk of work-related injury: US national health interview survey (2004–2008). Chronobiol. Int. 2010, 27, 1013–1030. [Google Scholar] [CrossRef]
- Sedgwick, P. Case-control studies: Advantages and disadvantages. BMJ 2014, 348, f7707. [Google Scholar] [CrossRef]
- Mishra, V.; Smyth, R. Work hours in Chinese enterprises: Evidence from matched employer-employee data. Ind. Relat. 2013, 44, 55–77. [Google Scholar]
- Tsai, M.C.; Nitta, M.; Kim, S.W.; Wang, W. Working Overtime in East Asia: Convergence or Divergence? J. Contemp. Asia 2016, 46, 700–722. [Google Scholar] [CrossRef]
- Kondo, N.; Oh, J. Suicide and karoshi (death from overwork) during the recent economic crises in Japan: The impacts, mechanisms and political responses. J. Epidemiol. Community Health 2010, 64, 649–650. [Google Scholar] [CrossRef]
- Lin, C.K.; Lin, R.T. Overwork and its impact on workers’ health: A cross-country comparison of overwork-related cardiovascular mortalities and its reflection in the Taiwanese situation. Occup. Environ. Med. 2017, 74. [Google Scholar] [CrossRef]
- Lin, R.T.; Lin, C.K.; Christiani, D.C.; Kawachi, I.; Cheng, Y.; Verguet, S.; Jong, S. The impact of the introduction of new recognition criteria for overwork-related cardiovascular and cerebrovascular diseases: A cross-country comparison. Sci. Rep. 2017, 7, 167. [Google Scholar] [CrossRef]
- Park, J.; Kim, Y.; Cheng, Y.; Horie, S. A comparison of the recognition of overwork-related cardiovascular disease in Japan, Korea, and Taiwan. Ind. Health 2012, 50, 17–23. [Google Scholar] [CrossRef]
- Petroff, A. German Workers Win Right to 28-Hour Week. CNN Money. 2018. Available online: http://money.cnn.com/2018/02/07/news/economy/germany-28-hour-work-week/index.html (accessed on 13 June 2018).
- Ng, Y.; Leung, R. Will Hong Kong’s Problem with Long Working Hours Ever Come to an End? South China Morning Post. 10 March 2018. Available online: http://www.scmp.com/news/hong-kong/politics/article/2136552/will-hong-kongs-problem-long-working-hours-ever-come-end (accessed on 13 June 2018).
- Schreuder, K.J.; Roelen, C.A.; Koopmans, P.C.; Groothoff, J.W. Job demands and health complaints in white and blue collar workers. Work 2008, 31, 425–432. [Google Scholar]
- Virtanen, M.; Ferrie, J.E.; Singh-Manoux, A.; Shipley, M.J.; Vahtera, J.; Marmot, M.G.; Kivimäki, M. Overtime work and incident coronary heart disease: The Whitehall II prospective cohort study. Eur. Heart J. 2010, 31, 1737–1744. [Google Scholar] [CrossRef]
- Jeong, I.; Rhie, J.; Kim, I.; Ryu, I.; Jung, P.K.; Park, Y.S.; Lim, Y.S.; Kim, S.G.; Park, S.G.; Im, H.L.; et al. Working hours and cardiovascular disease in Korean workers: A case-control study. J. Occup. Health 2013, 55, 385–391. [Google Scholar] [CrossRef]
- Ma, Y.; Wang, Y.J.; Chen, B.R.; Shi, H.J.; Wang, H.; Khurwolah, M.R.; Li, Y.F.; Xie, Z.Y.; Yang, Y.; Wang, L.S. Study on association of working hours and occupational physical activity with the occurrence of coronary heart disease in a Chinese population. PLoS ONE 2017, 12, e0185598. [Google Scholar] [CrossRef]
- Poleshuck, E.L.; Green, C.R. Socioeconomic disadvantage and pain. Pain 2008, 136, 235–238. [Google Scholar] [CrossRef]
- Giorgi, G.; Arcangeli, G.; Mucci, N.; Cupelli, V. Economic stress in the workplace: The impact of fear of this crisis on mental health. Work 2015, 51, 135–142. [Google Scholar] [CrossRef]
- Mucci, N.; Giorgi, G.; Roncaioli, M.; Fiz Perez, J.; Arcangeli, G. The correlation between stress and economic crisis: A systematic review. Neuropsychiatr. Dis. Treat 2016, 12, 983–993. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Percentage |
|---|---|
| Publication years | |
| 1998–2007 | 26.09 |
| 2008–2018 | 73.91 |
| Origin | |
| Asian countries | 61.59 |
| Western countries | 38.41 |
| Gender | |
| Males | 58.73 |
| Females | 41.27 |
| Study design | |
| Case-control study | 10.87 |
| Cross-sectional study | 54.35 |
| Prospective cohort study | 34.78 |
| Diagnosis method | |
| Self-report | 63.04 |
| Health or medical examination | 36.96 |
| Occupational Health Condition | Number of Records | Effect Size and 95% Interval | Heterogeneity | Adjustment for Publication Bias | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Overall OR | Lower Limit | Upper Limit | p-Value | I-Squared | Data Points Imputed | Overall OR | Lower Limit | Upper Limit | ||
| PH | 85 | 1.177 | 1.102 | 1.257 | 0.000 | 67.131 | 6 | 1.118 | 1.041 | 1.200 |
| MH | 55 | 1.366 | 1.238 | 1.507 | 0.000 | 55.733 | 12 | 1.197 | 1.072 | 1.336 |
| HB | 35 | 1.100 | 1.004 | 1.204 | 0.000 | 59.660 | 0 | 1.100 | 1.004 | 1.204 |
| RH | 54 | 1.465 | 1.332 | 1.611 | 0.000 | 68.678 | 7 | 1.323 | 1.188 | 1.473 |
| NH | 14 | 1.065 | 0.942 | 1.204 | 0.001 | 63.539 | 0 | 1.065 | 0.942 | 1.204 |
| Overall | 243 | 1.245 | 1.195 | 1.298 | 0.000 | 67.574 | ||||
| Moderator | Effect Size and 95% Interval | Test of Null | Test to Model | |||||
|---|---|---|---|---|---|---|---|---|
| Odds Ratio | 95% Lower | 95% Upper | Z-Value | 2-Sided p-Value | Q-Value | df (Q) | Meta-Regression p-Value | |
| Gender | 5.797 | 2.000 | 0.055 | |||||
| Males | 1.280 | 1.176 | 1.394 | 5.711 | 0.000 | |||
| Females | 1.135 | 1.053 | 1.222 | 3.332 | 0.001 | |||
| Diagnosis method | 1.579 | 1.000 | 0.209 | |||||
| Self-report | 1.263 | 1.205 | 1.324 | 9.735 | 0.000 | |||
| Health or medical examination | 1.188 | 1.094 | 1.291 | 4.086 | 0.000 | |||
| Study design | 56.377 | 2.000 | 0.000 ** | |||||
| Case-control study ** | 1.811 | 1.466 | 2.239 | 5.499 | 0.000 | |||
| Cross-sectional study ** | 1.338 | 1.267 | 1.414 | 10.465 | 0.000 | |||
| Prospective cohort study | 1.049 | 0.997 | 1.104 | 1.826 | 0.068 | |||
| Cut-off point for long working hours | 57.331 | 2.000 | 0.000 ** | |||||
| >50 h/week or >10 h/day ** | 1.420 | 1.337 | 1.508 | 11.446 | 0.000 | |||
| ≤50 h/week or ≤10 h/day ** | 1.097 | 1.035 | 1.162 | 3.130 | 0.002 | |||
| Working class | 1.318 | 2.000 | 0.517 | |||||
| White collar occupations | 1.095 | 1.043 | 1.149 | 3.668 | 0.000 | |||
| Pink collar occupations | 1.168 | 1.002 | 1.360 | 1.992 | 0.046 | |||
| Blue collar occupations | 1.275 | 0.907 | 1.792 | 1.400 | 0.161 | |||
| Country of origin | 35.043 | 12.000 | 0.000 ** | |||||
| Asian Countries ** | 1.321 | 1.231 | 1.418 | 7.741 | 0.000 | |||
| China ** | 1.745 | 1.428 | 2.132 | 5.441 | 0.000 | |||
| China and Japan | 1.569 | 0.817 | 3.013 | 1.352 | 0.176 | |||
| Japan ** | 1.333 | 1.191 | 1.492 | 5.010 | 0.000 | |||
| Korea ** | 1.237 | 1.124 | 1.361 | 4.351 | 0.000 | |||
| Western countries ** | 1.180 | 1.126 | 1.237 | 6.854 | 0.000 | |||
| Australia and New Zealand * | 1.230 | 1.050 | 1.442 | 2.801 | 0.010 | |||
| Denmark | 1.091 | 0.840 | 1.418 | 0.656 | 0.512 | |||
| Finland | 1.063 | 0.966 | 1.170 | 1.250 | 0.211 | |||
| Italy | 1.341 | 0.993 | 1.811 | 1.915 | 0.055 | |||
| Spain * | 1.248 | 1.131 | 1.377 | 4.404 | 0.000 | |||
| Sweden | 1.198 | 0.937 | 1.532 | 1.438 | 0.150 | |||
| The UK * | 1.083 | 1.008 | 1.163 | 2.187 | 0.029 | |||
| The US ** | 1.274 | 1.108 | 1.465 | 3.393 | 0.001 | |||
| Health measure | ||||||||
| Physiological health | 35.773 | 4.000 | 0.000 ** | |||||
| All-cause mortality | 0.975 | 0.924 | 1.029 | −0.920 | 0.358 | |||
| Cardiovascular heart diseases ** | 1.539 | 1.324 | 1.789 | 5.607 | 0.000 | |||
| Metabolic syndrome ** | 1.100 | 1.025 | 1.182 | 2.630 | 0.009 | |||
| Poor physical health | 1.408 | 0.893 | 2.221 | 1.471 | 0.141 | |||
| Type 2 diabetes | 0.855 | 0.497 | 1.472 | −0.565 | 0.572 | |||
| Mental health | 5.074 | 5.000 | 0.407 | |||||
| Anxiety | 1.308 | 1.041 | 1.644 | 2.301 | 0.021 | |||
| Depressive symptoms | 1.489 | 1.220 | 1.817 | 3.915 | 0.000 | |||
| Poor mental health | 1.239 | 1.018 | 1.510 | 2.134 | 0.033 | |||
| Psychiatric morbidity | 1.398 | 1.184 | 1.651 | 3.952 | 0.000 | |||
| Psychological distress | 1.110 | 0.878 | 1.403 | 0.870 | 0.384 | |||
| Psychological stress | 1.512 | 1.123 | 2.034 | 2.727 | 0.006 | |||
| Health behaviours | 2.255 | 3.000 | 0.521 | |||||
| Heavy drinking | 1.083 | 0.943 | 1.244 | 1.134 | 0.257 | |||
| Physical inactivity | 1.234 | 1.002 | 1.520 | 1.978 | 0.048 | |||
| Smoking | 1.055 | 0.890 | 1.251 | 0.620 | 0.535 | |||
| Unhealthy food habits | 0.990 | 0.796 | 1.230 | −0.094 | 0.925 | |||
| Related health | 9.604 | 4.000 | 0.048 * | |||||
| Fatigue ** | 1.439 | 1.149 | 1.803 | 3.169 | 0.002 | |||
| Injury ** | 1.276 | 1.091 | 1.492 | 3.047 | 0.002 | |||
| Poor sleep quality ** | 1.276 | 1.128 | 1.444 | 3.880 | 0.000 | |||
| Short sleep duration ** | 1.909 | 1.502 | 2.427 | 5.281 | 0.000 | |||
| Sleep disturbance * | 1.395 | 1.052 | 1.850 | 2.312 | 0.021 | |||
| Nonspecified health | - | - | - | |||||
| Poor health status | 1.065 | 0.942 | 1.204 | 1.000 | 0.317 | |||
| Working Class | Odds Ratio | 95% Lower | 95% Upper | Z-Value | 2-Sided p-Value | Q-Value | df (Q) | Meta-Regression p-Value |
|---|---|---|---|---|---|---|---|---|
| Physiological health | 1.449 | 2.000 | 0.485 | |||||
| White collar occupations | 1.145 | 1.007 | 1.303 | 2.065 | 0.039 | |||
| Pink collar occupations | 0.986 | 0.792 | 1.226 | −0.130 | 0.896 | |||
| Blue collar occupations | 1.192 | 0.747 | 1.902 | 0.737 | 0.461 | |||
| Mental health | 1.037 | 2.000 | 0.595 | |||||
| White collar occupations | 1.310 | 1.166 | 1.473 | 4.546 | 0.000 | |||
| Pink collar occupations | 1.760 | 0.961 | 3.223 | 1.831 | 0.067 | |||
| Blue collar occupations | 1.250 | 0.962 | 1.624 | 1.672 | 0.095 | |||
| Health behaviours | 3.069 | 2.000 | 0.216 | |||||
| White collar occupations | 0.988 | 0.915 | 1.066 | −0.316 | 0.752 | |||
| Pink collar occupations | 1.102 | 0.745 | 1.629 | 0.487 | 0.626 | |||
| Blue collar occupations | 1.250 | 0.962 | 1.624 | 1.672 | 0.095 | |||
| Related health | 13.143 | 2.000 | 0.001 * | |||||
| White collar occupations | 0.887 | 0.713 | 1.104 | −1.075 | 0.282 | |||
| Pink collar occupations | 0.989 | 0.940 | 1.040 | −0.438 | 0.662 | |||
| Blue collar occupations * | 1.366 | 1.144 | 1.631 | 3.445 | 0.001 | |||
| Nonspecified health | 3.649 | 2.000 | 0.161 | |||||
| White collar occupations | 0.970 | 0.853 | 1.103 | −0.463 | 0.643 | |||
| Pink collar occupations | 0.881 | 0.666 | 1.165 | −0.890 | 0.374 | |||
| Blue collar occupations | 1.115 | 0.987 | 1.260 | 1.745 | 0.081 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, K.; Chan, A.H.S.; Ngan, S.C. The Effect of Long Working Hours and Overtime on Occupational Health: A Meta-Analysis of Evidence from 1998 to 2018. Int. J. Environ. Res. Public Health 2019, 16, 2102. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122102
Wong K, Chan AHS, Ngan SC. The Effect of Long Working Hours and Overtime on Occupational Health: A Meta-Analysis of Evidence from 1998 to 2018. International Journal of Environmental Research and Public Health. 2019; 16(12):2102. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122102
Chicago/Turabian StyleWong, Kapo, Alan H. S. Chan, and S. C. Ngan. 2019. "The Effect of Long Working Hours and Overtime on Occupational Health: A Meta-Analysis of Evidence from 1998 to 2018" International Journal of Environmental Research and Public Health 16, no. 12: 2102. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122102