Clinical Effectiveness and Cost-Effectiveness of Oral-Health Promotion in Dental Caries Prevention among Children: Systematic Review and Meta-Analysis

Abstract
:1. Introduction
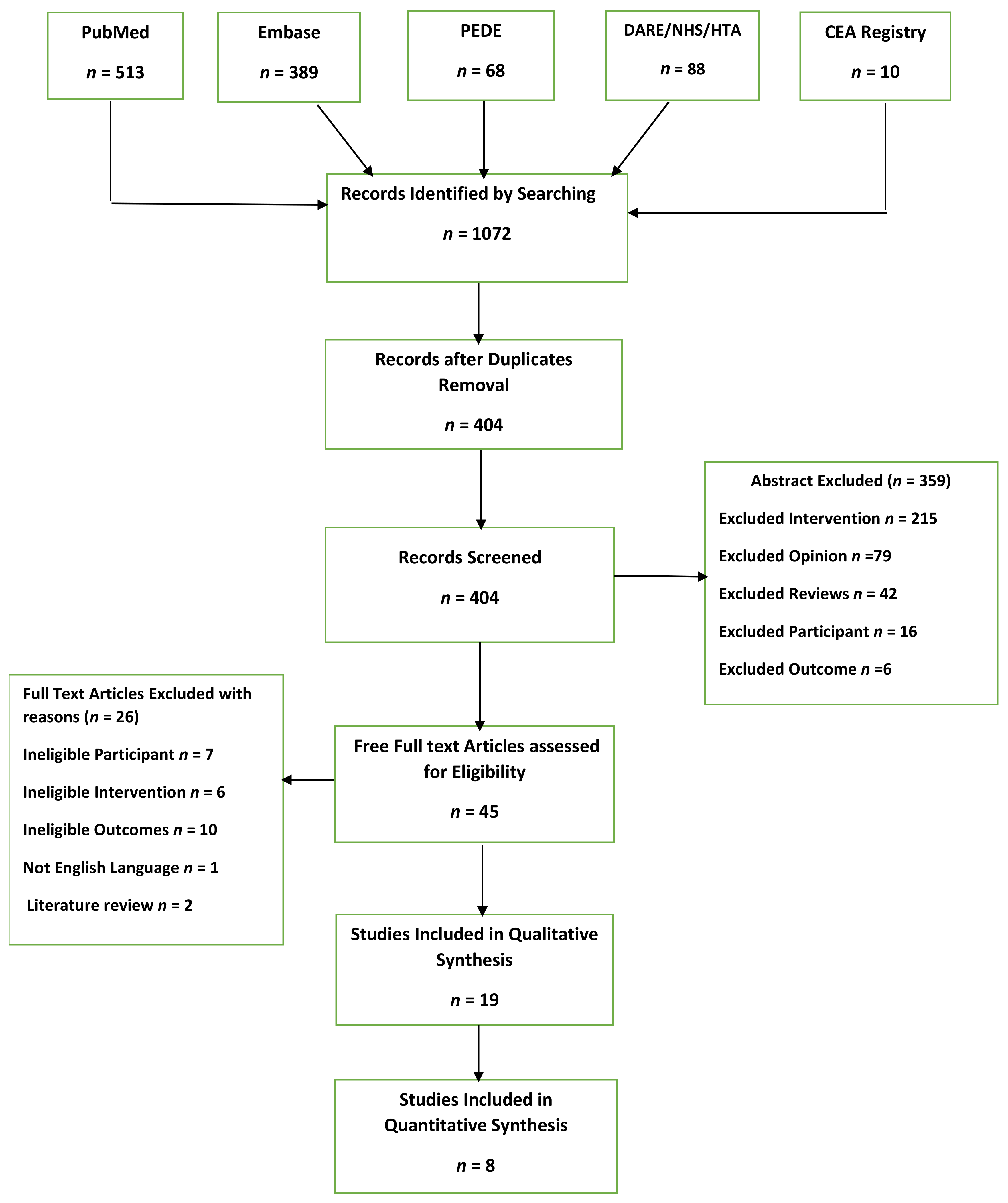
2. Materials and Methods
2.1. Type of Studies
2.2. Included Participant, Intervention, Comparator, and Outcome (PICO) Terms
- Children aged from 0 to 12 years old who were healthy without health-related diseases except for dental caries.
- Studies of mixed populations of parents and children were included where the data of children were presented separately.
- Community-based oral-health education/training programs related to healthy oral habits.
- Screening of children’s teeth.
- Supervised toothbrushing technique through the provision of toothbrushes, an appropriate amount of fluoride toothpaste, and topical fluoride.
- Advice on dietary control, such as limitation of sugar or carbohydrates consumption, and enhanced fortified nutrition with an appropriate amount of calcium intake.
- Reducing the “Decayed, Missing, Filled Teeth (DMFT) Index for permanent teeth or (DMFT) Index for deciduous teeth” among children.
- OHPP cost, incremental cost (difference between mean costs of intervention and mean costs of the comparator), and cost-effectiveness analysis (CEA).
3. Results
3.1. According to the Review, to Summarize the Studies That Met the Inclusion Criteria
3.1.1. Strong-Quality “Model-Based” Economic Evaluation Studies
3.1.2. Moderate Quality “Model-Based” Economic Evaluation Studies
3.1.3. Strong-Quality “Trial-Based” Economic Evaluation Studies
3.1.4. Moderat Quality “Trial-Based” Economic Evaluation Studies
3.1.5. Limited Economic-Evaluation Outcomes of Moderate Qualified “Trial-Based’ Economic-Evaluation Studies and “Model-Based” Economic-Evaluation Studies”
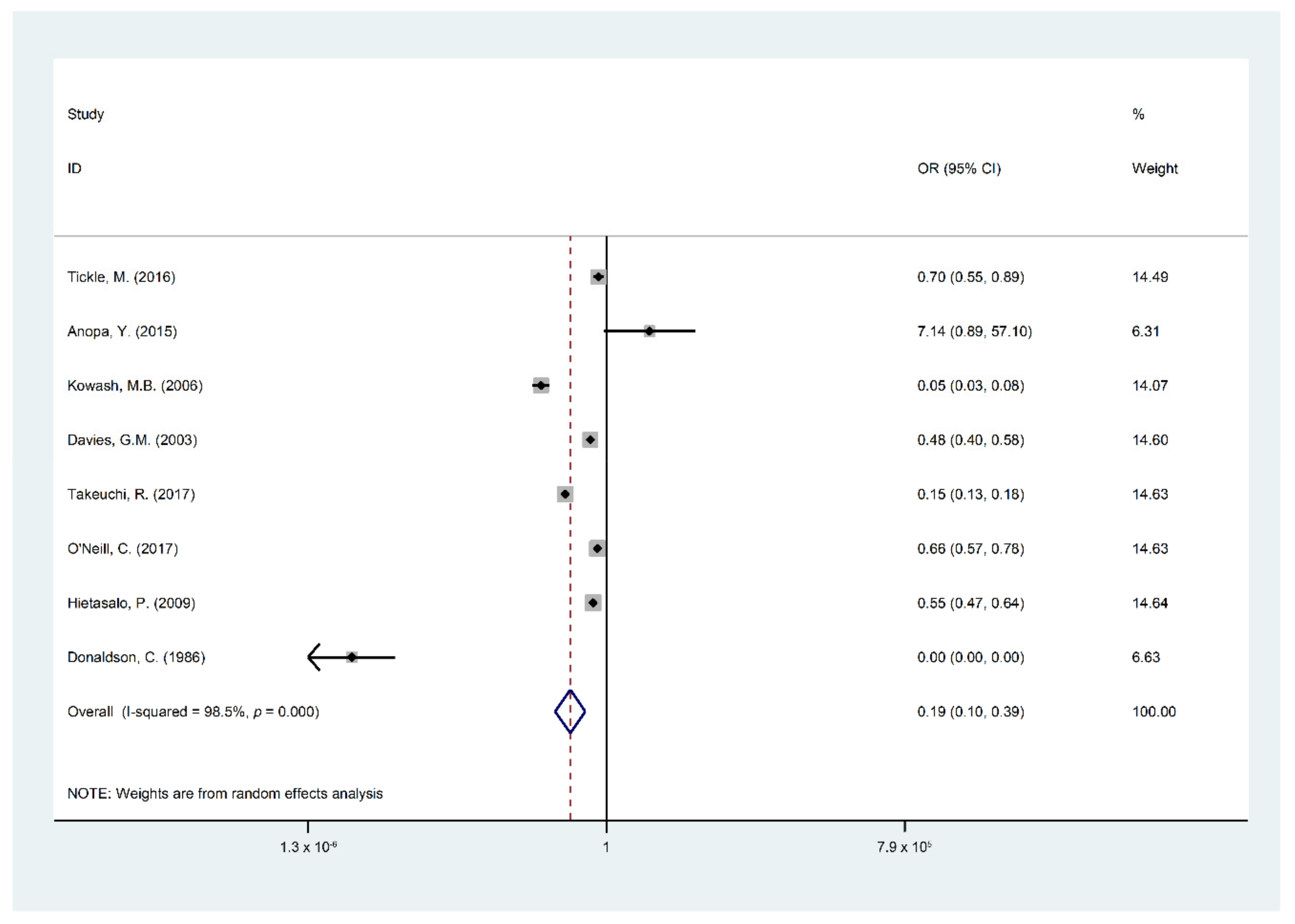
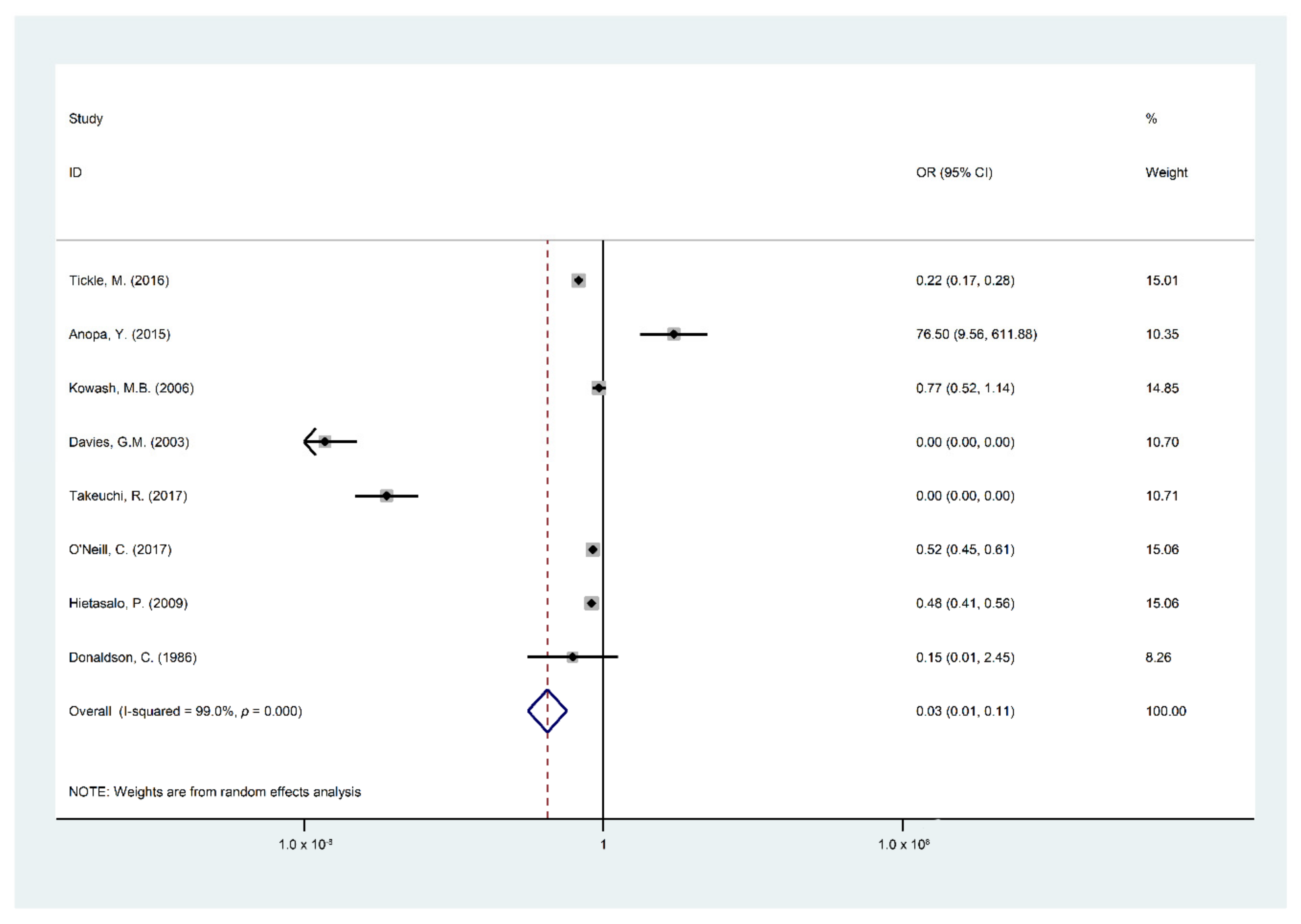
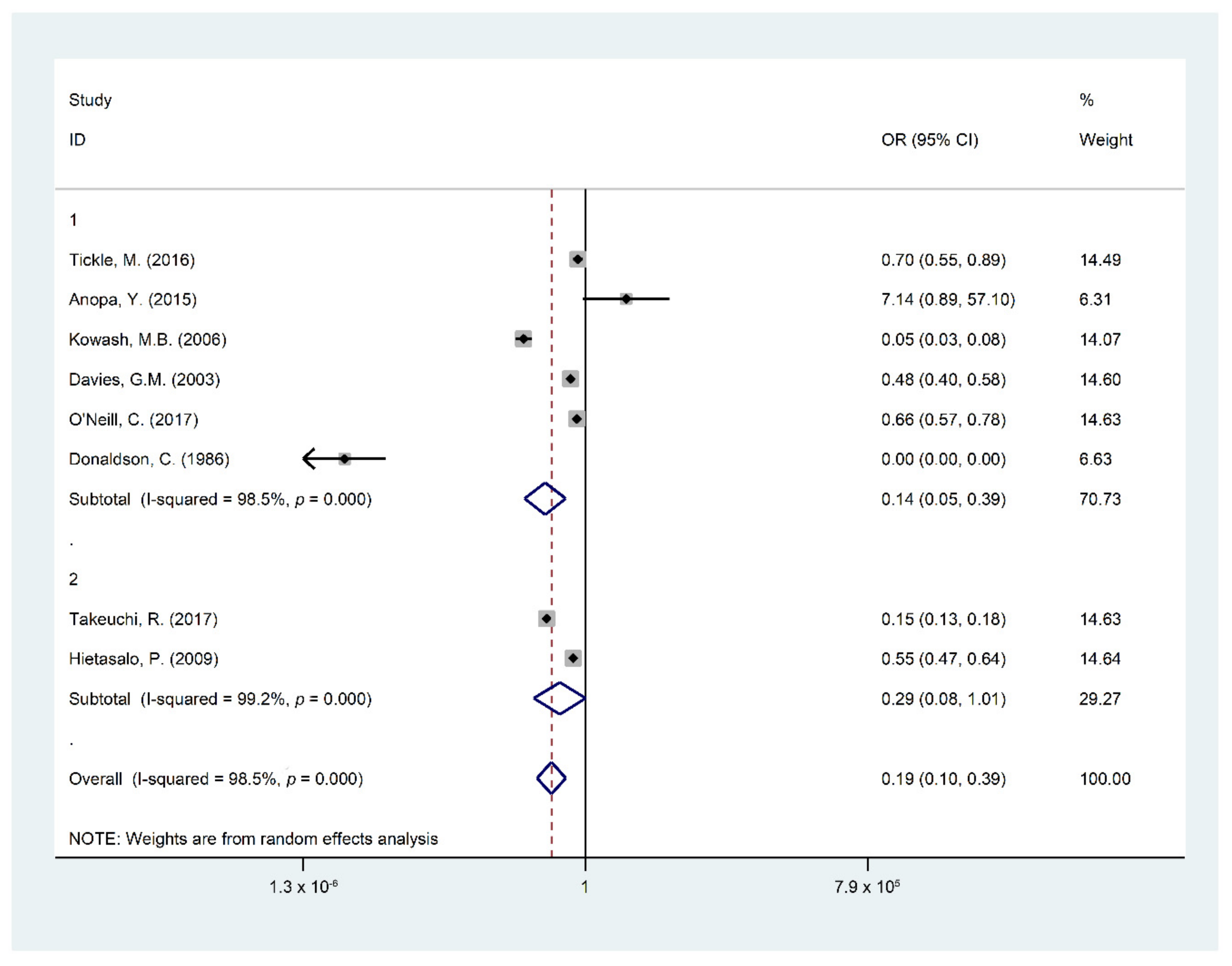
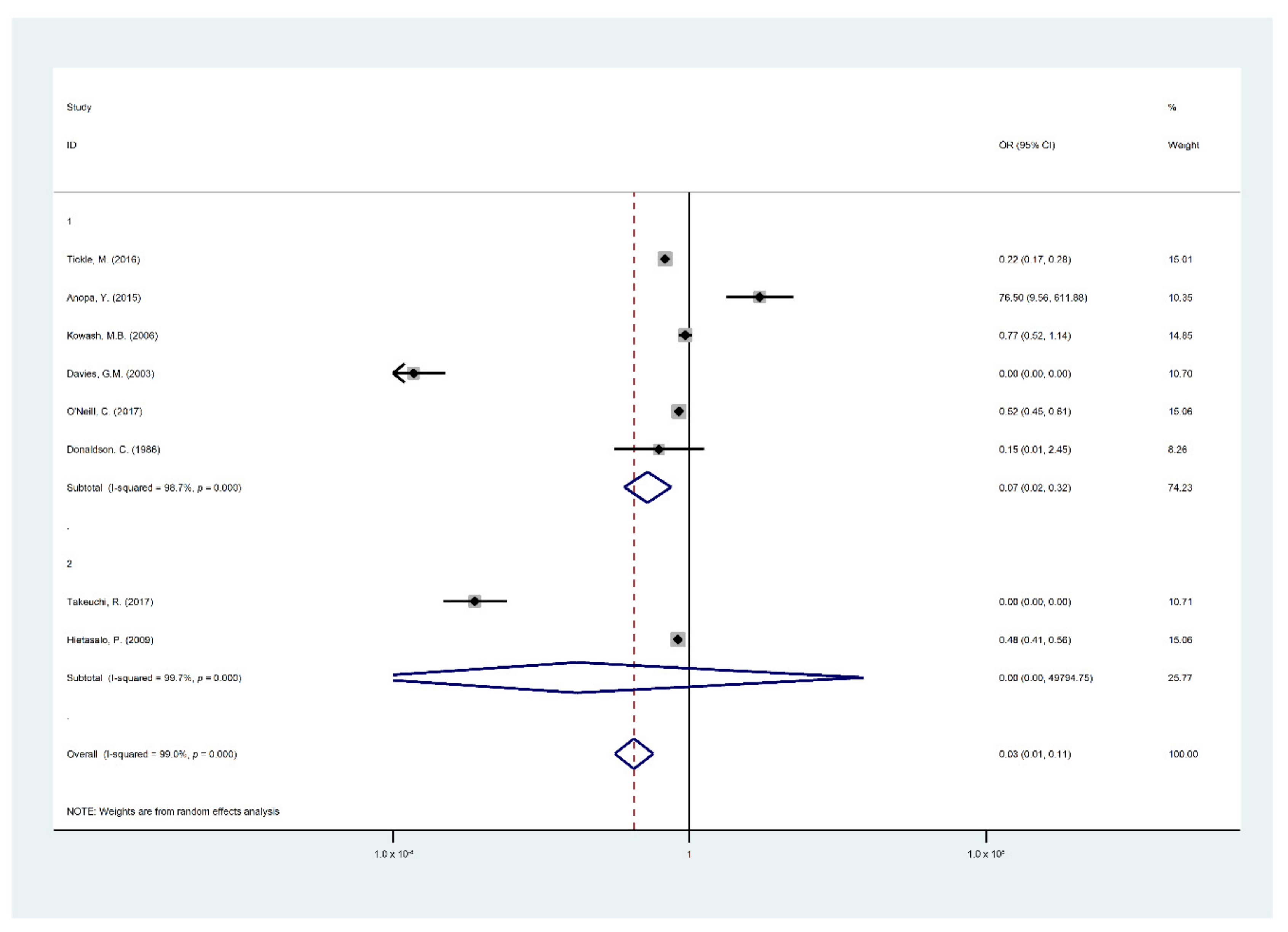
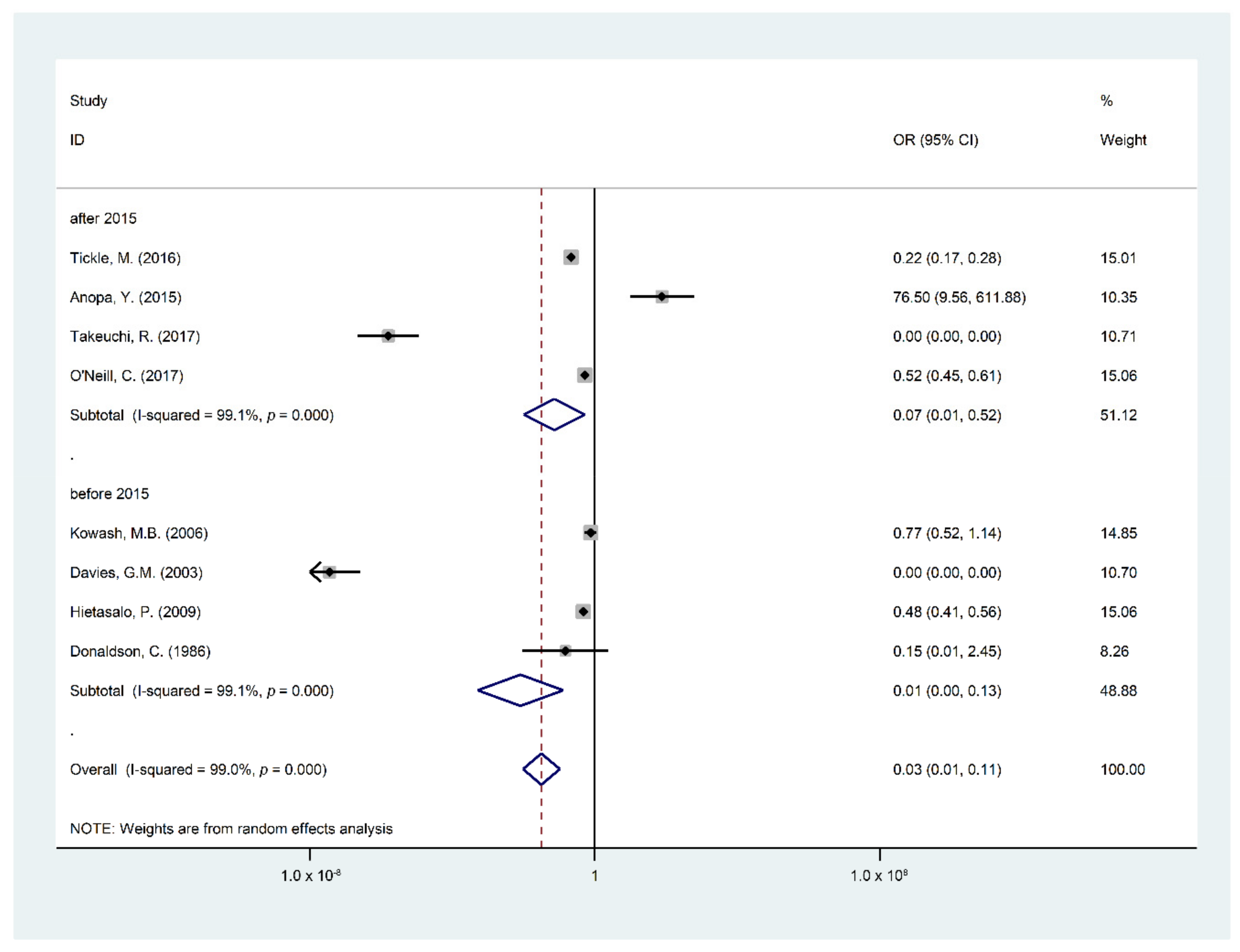
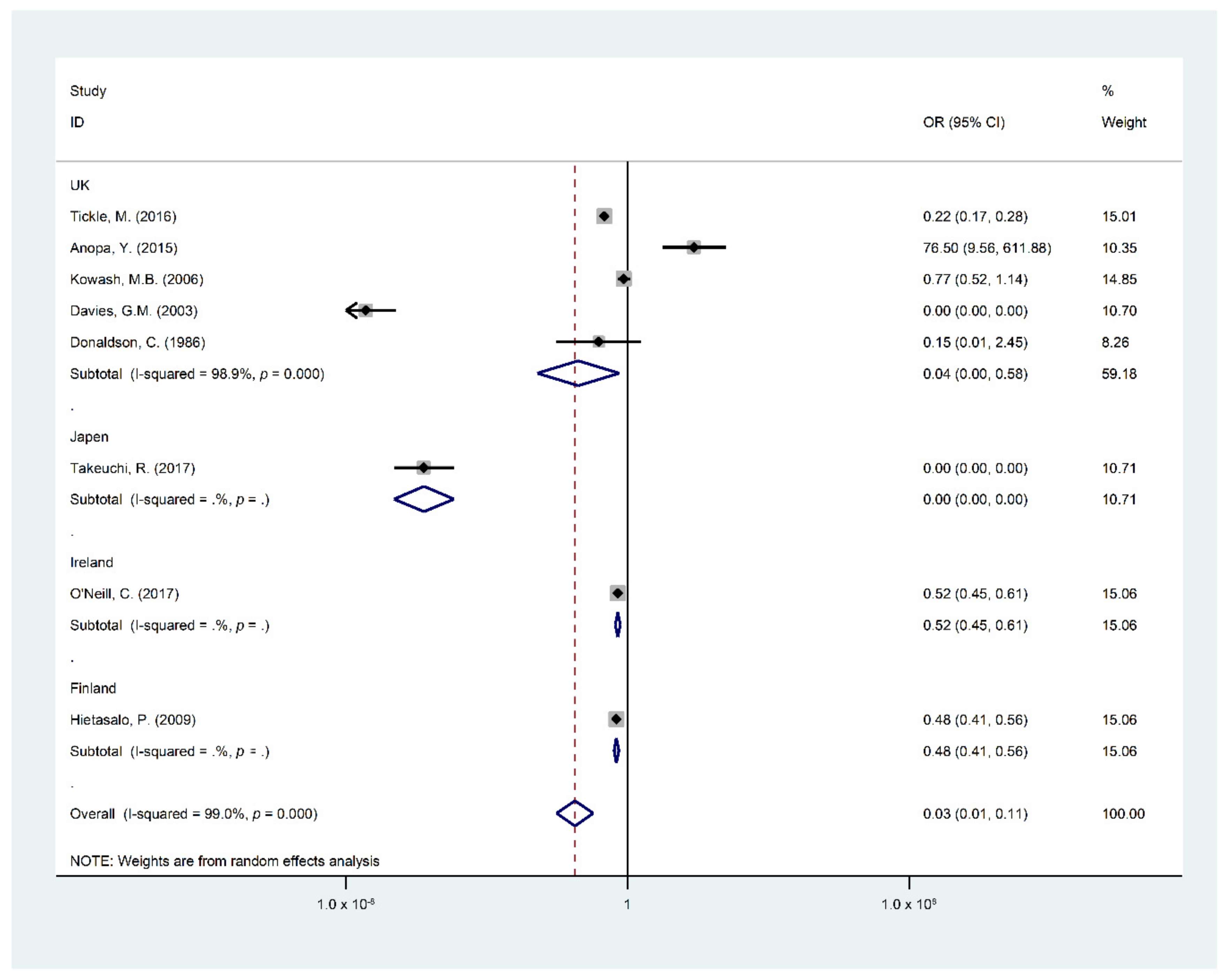
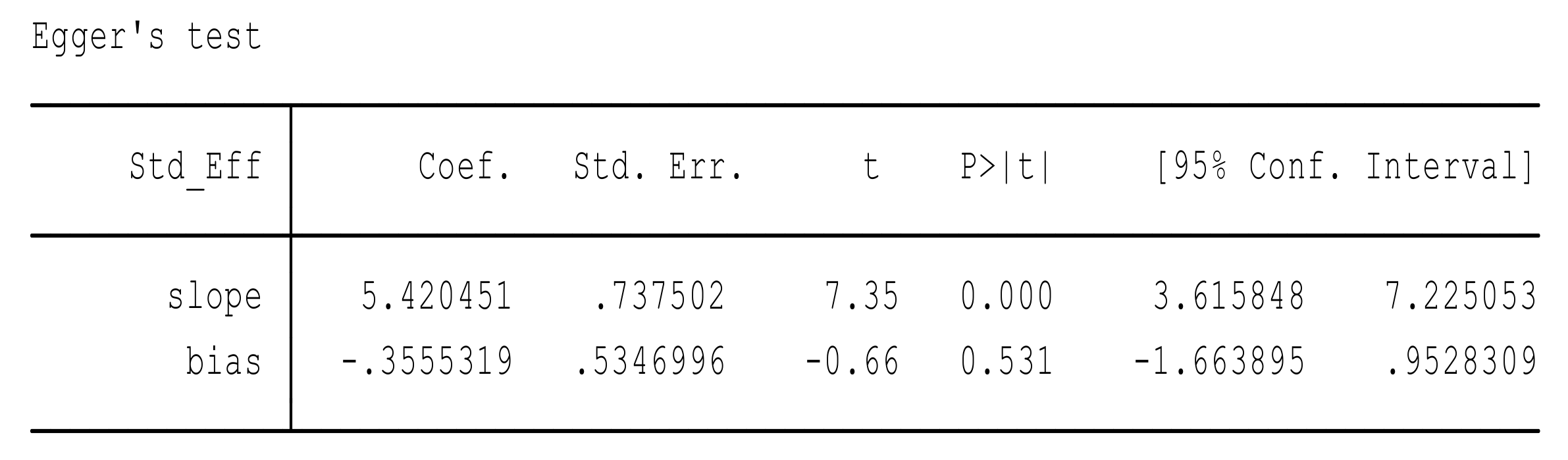
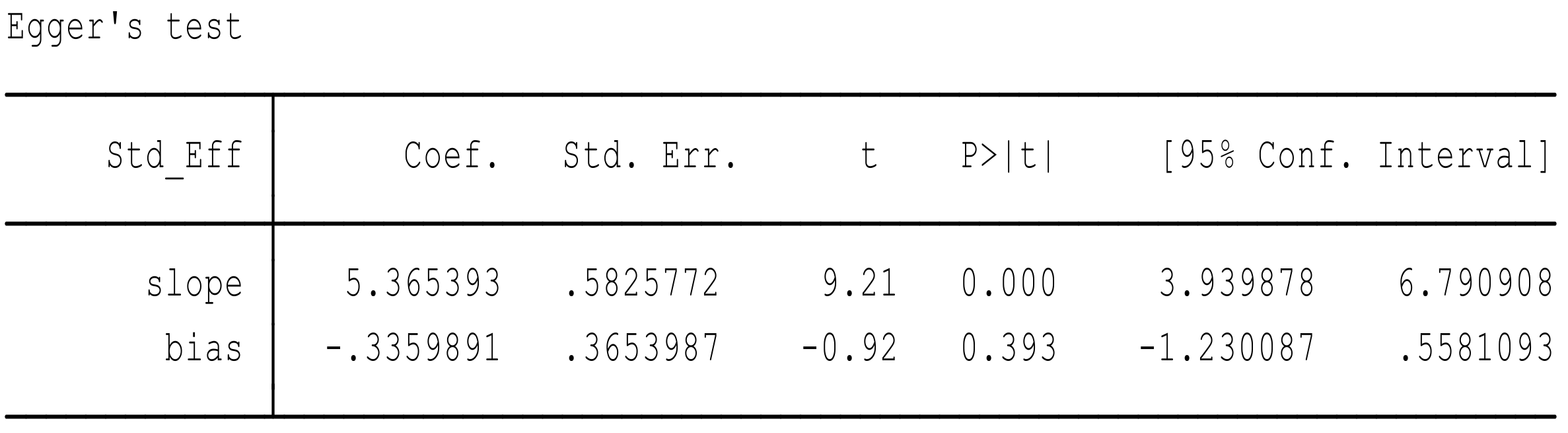
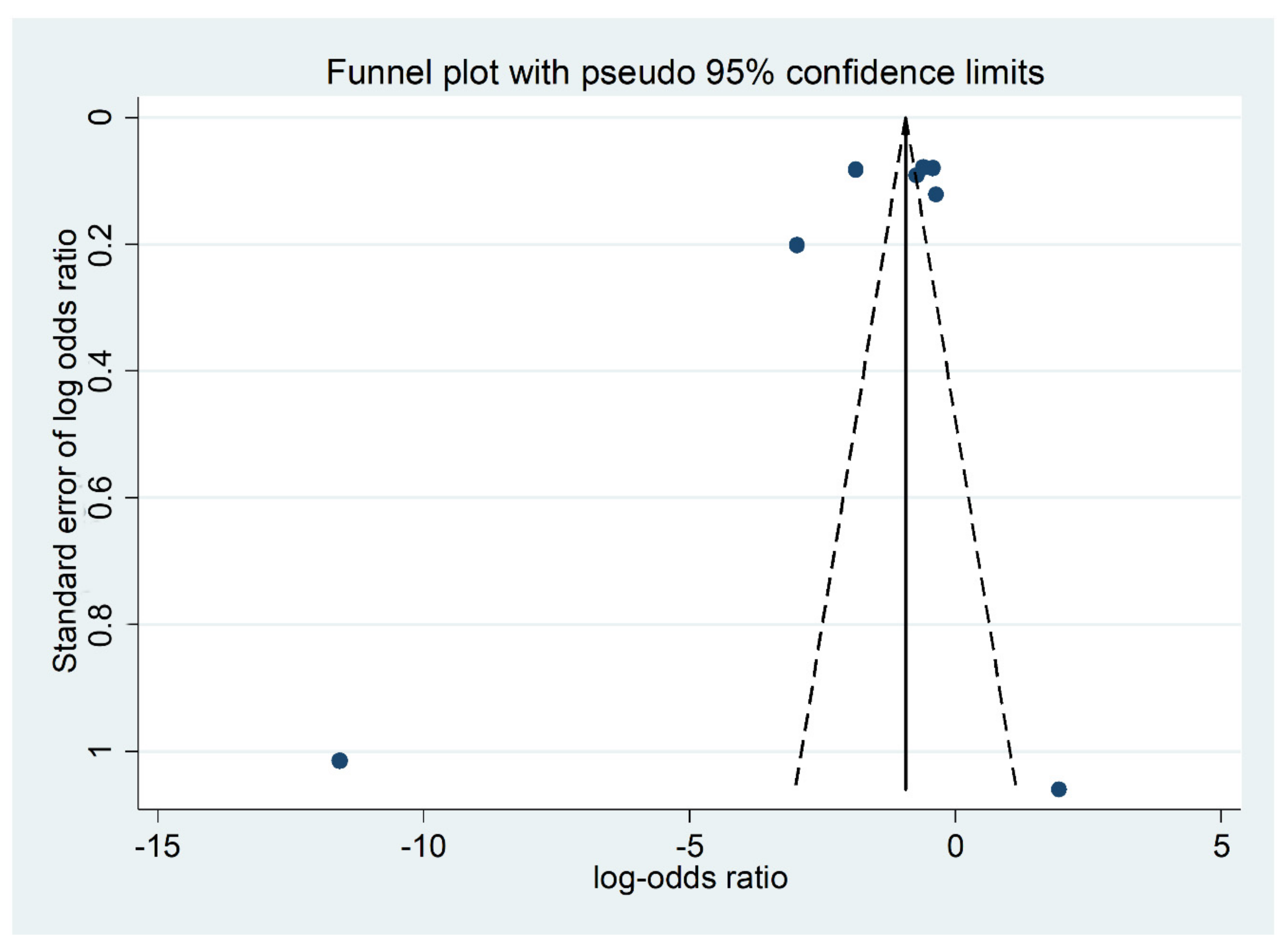
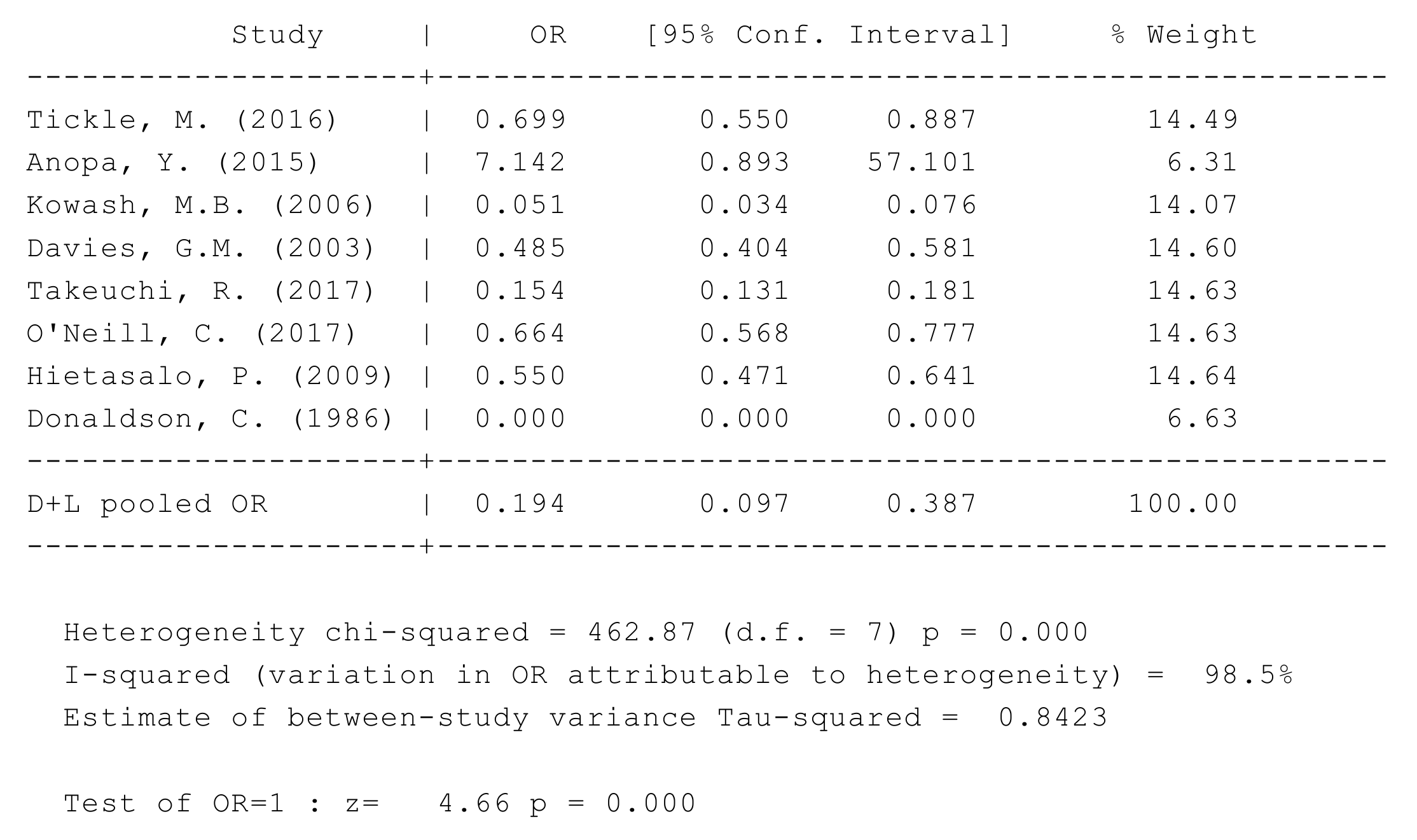
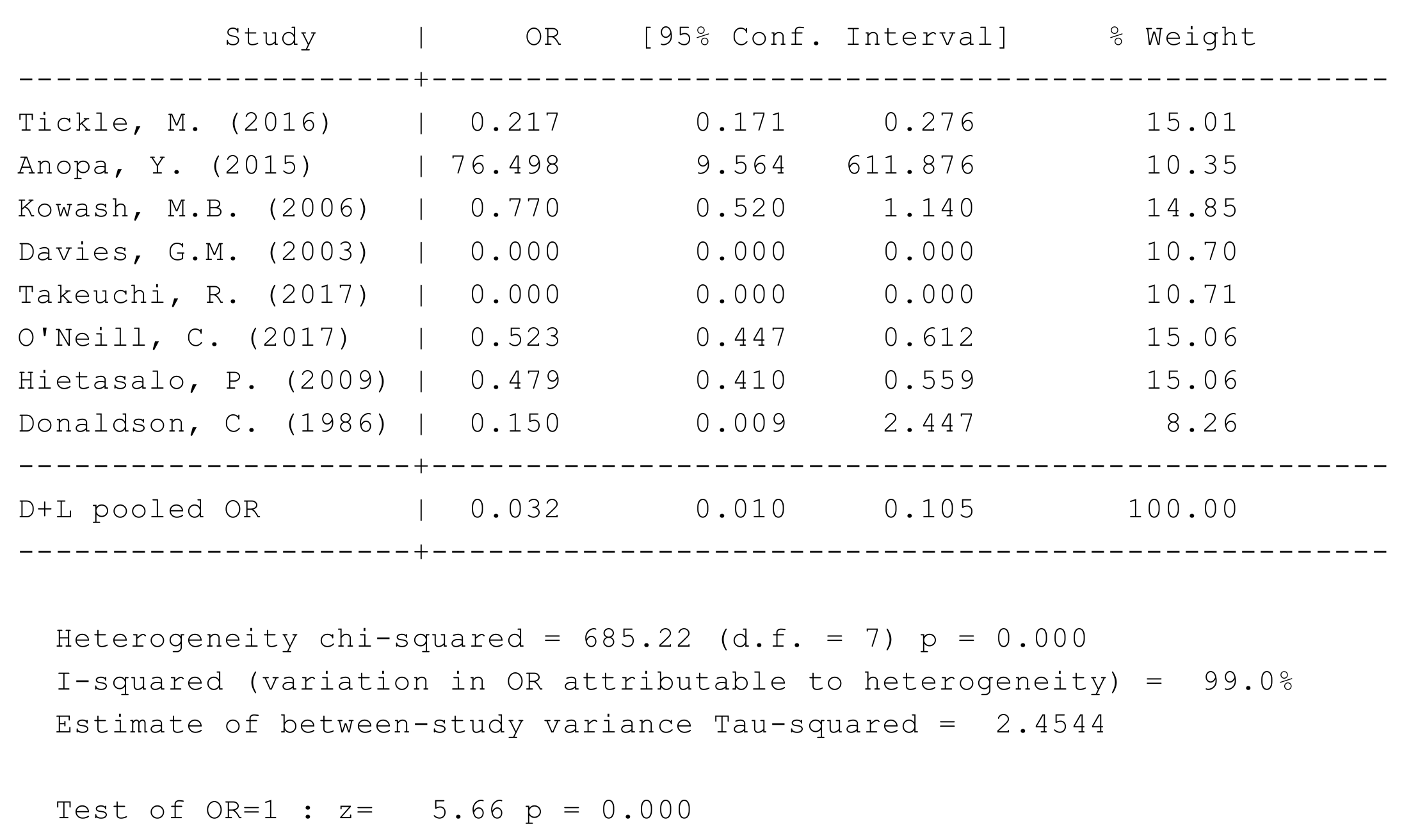
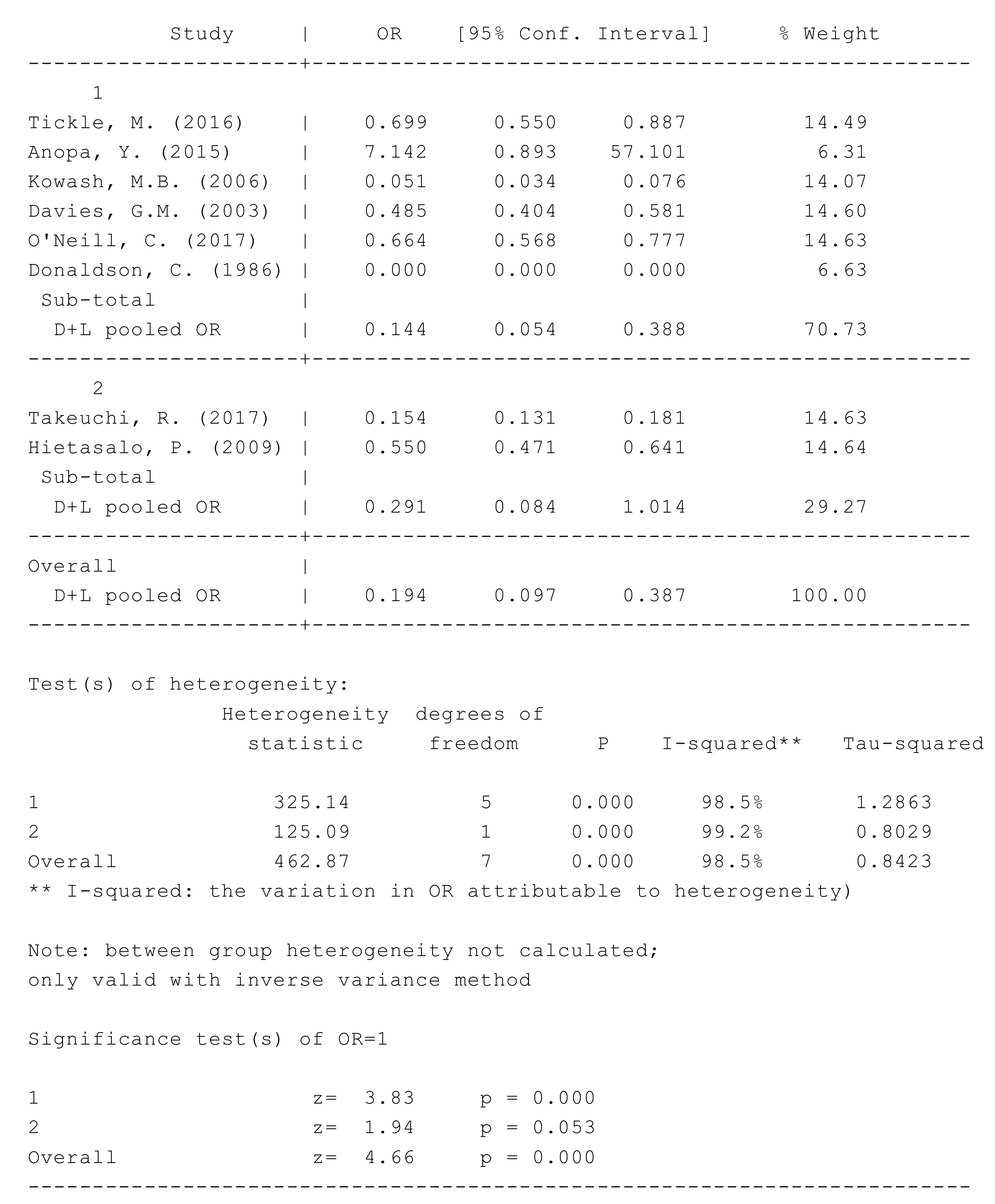
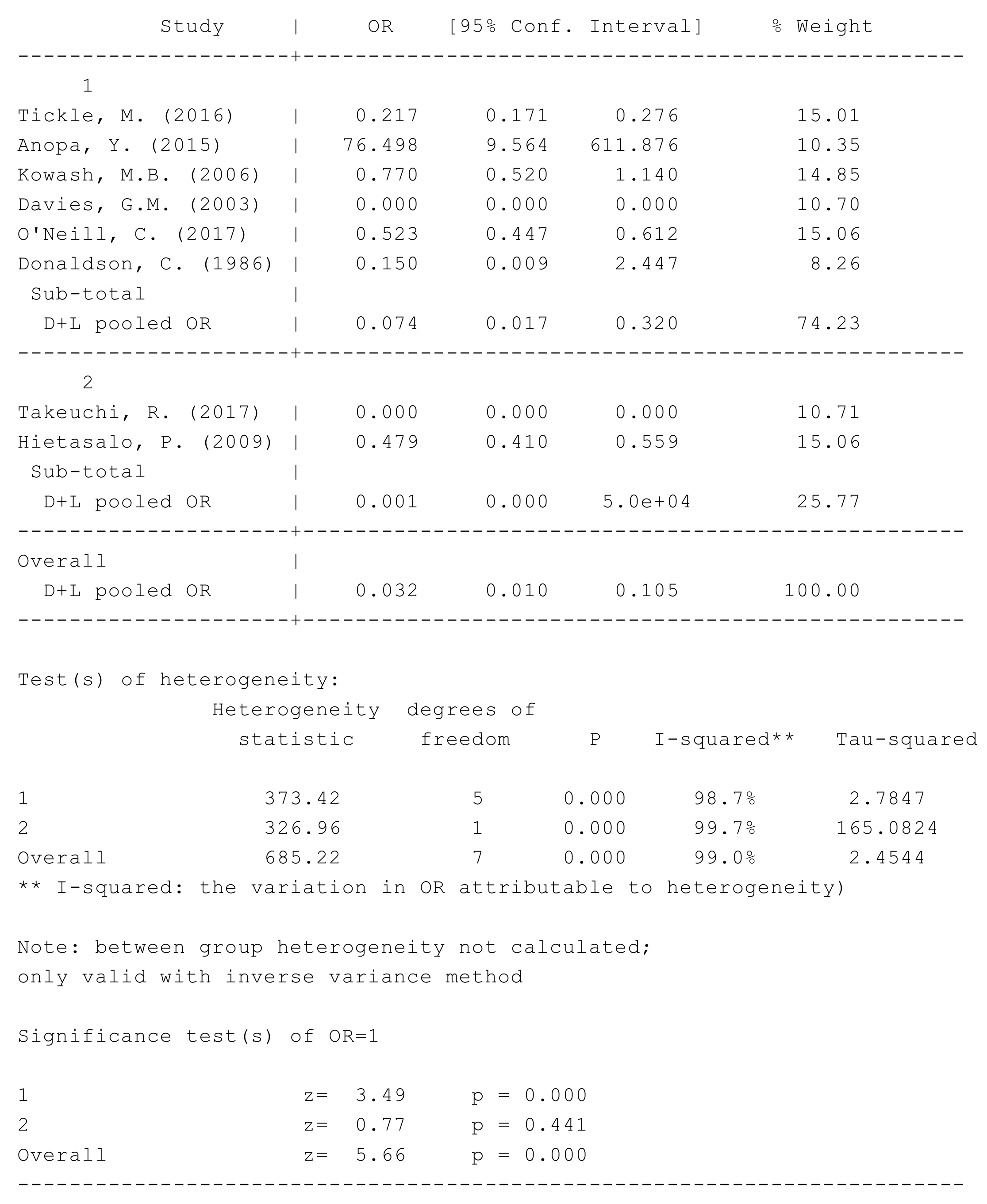
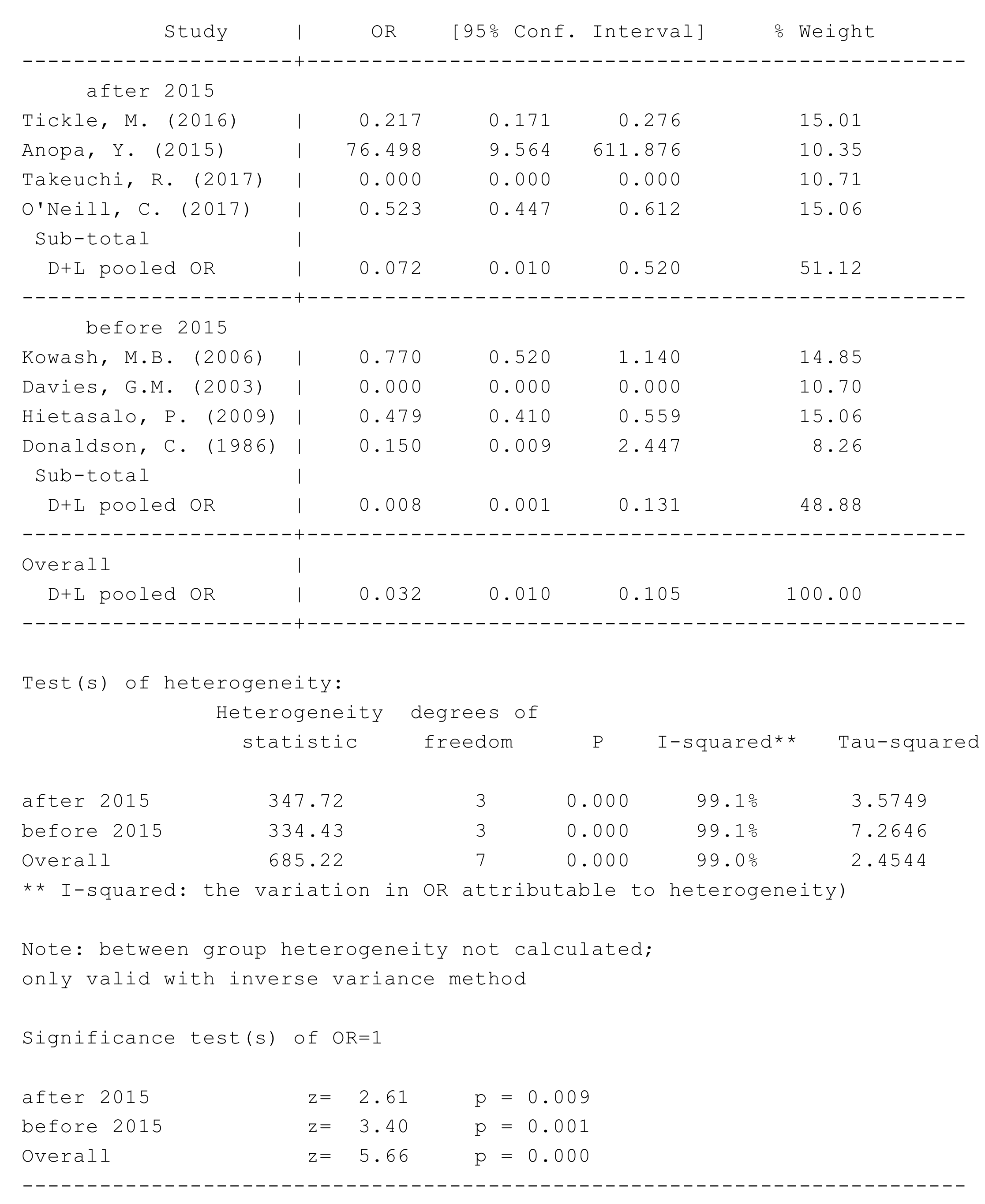
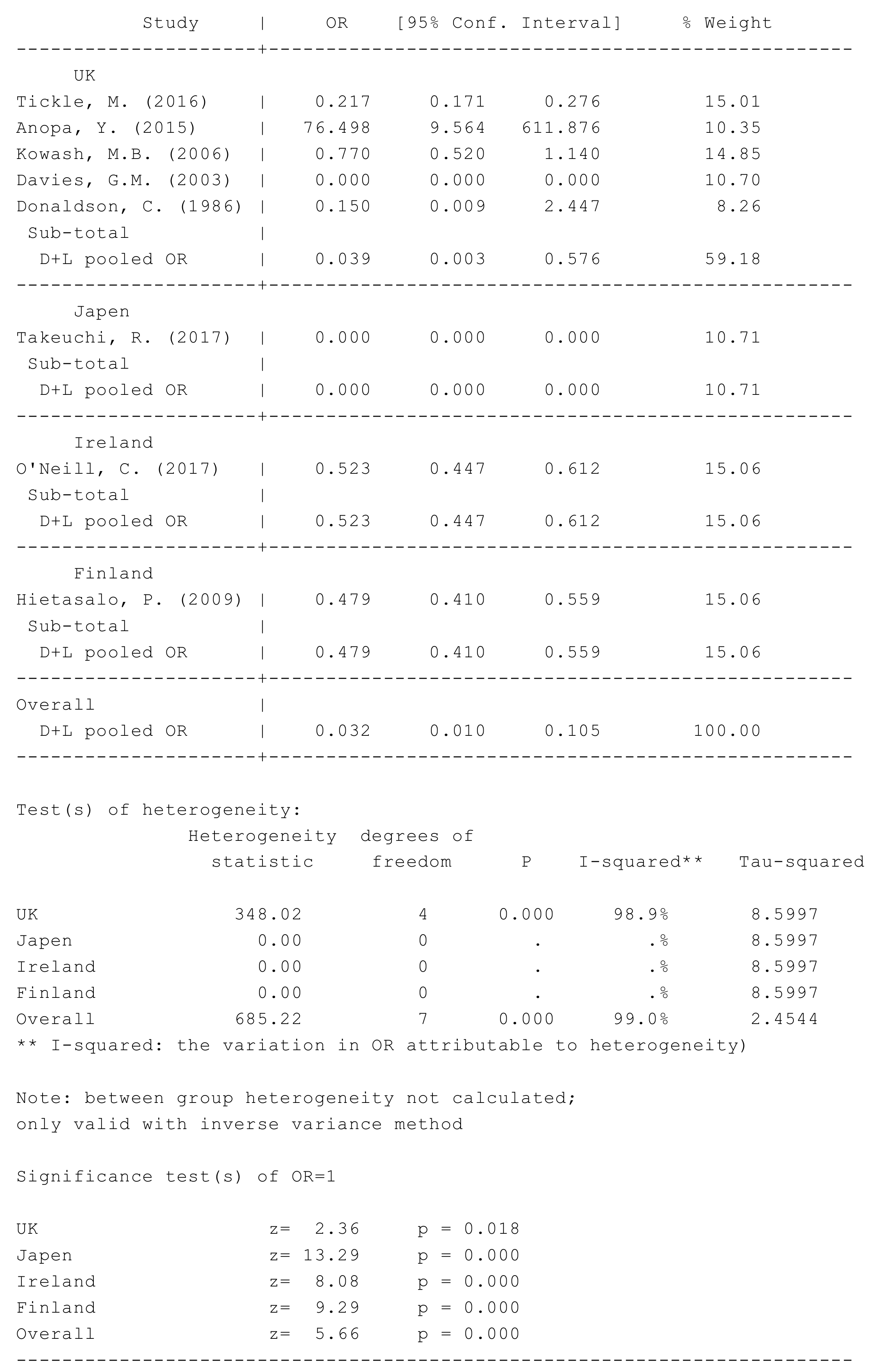
3.2. Meta-Analysis
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S.no | Lead Author | Year | Country | Study Design | Participant | Mean Age (Year) | Intervention | Main Conclusion | Source of Funding | Quality Assessment |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Hietasalo, P. [5] | 2009 | Finland | Trial-Based | 497 children who had at least one active initial caries lesion at baseline of the study | 11.5 | 1. Designed a centered regimen for caries Control 2. Fluoride Varnish | The experimental regimen would be more cost-effective than standard care if the follow-up the period had been longer | Finnish Dental Society Apollonia, the Yrjo Jahnsson Foundation | Strong Quality |
| 2. | Kowash, M.B. [15] | 2006 | United Kingdom | Model-Based | 7000 infants aged 8 months | 0.6666 | Long-term dental health education program through home visits | Dental Health Education program of home visits with mothers of young infants to prevent early childhood caries gave better benefit-costs and cost-effectiveness ratios than other preventive programs. | British National Health Service (UK) fees | Strong Quality |
| 3. | Pukallus, M. [16] | 2013 | Australia | Model-Based | Mothers in the intervention group were telephoned when their children were aged approximately 6, 12 and 18 months | 1 | A telephone Oral Health prevention program | A telephone intervention likely to generate considerable benefits and cost savings to the public dental health service in disadvantaged communities | Australian Centre for Health Services Innovation | Strong Quality |
| 4. | Anopa, Y. [19] | 2015 | United Kingdom | Model-Based | Hypothetical cohorts of 1000 children aged 5 years | 5 | Nursery tooth brushing program | Tooth brushing program represents a preventative spend of both reduced costs and health gains in child oral health outcomes. | E-Government through NHS payments | Strong Quality |
| 5. | Blaikie, D.C. [20] | 1977 | Australia | Model-Based | Community School Children | NA | Free for an Oral screening program compared with Regular community dental health branch | Dental Health Branch was more cost-effective than the proposed fee-for-service alternative. | Department of Public Health ledger listings | Strong Quality |
| 6. | Tickle, M. [24] | 2016 | United Kingdom | Trial-Based | Children aged 2–3 years, who were caries free at baseline | 3.1 | 1. Oral Health advice 2. providing Toothbrushes and Toothpaste 3. Flouride Varnish | The intervention was unlikely to be cost-effective in terms of either keeping children caries free. | The National Institute for Health Research (NIHR) Health Technology Assessment program | Strong Quality |
| 7. | Quinonez, R.B [17] | 2006 | United Kingdom | Model-Based | Application of universal fluoride varnish at 9, 18, 24, and 36 months the cycles extended to 42 months to account for benefits incurred after the last Fluoride varnish application at the 36-month well-child visit. | 2.1250 | Application of fluoride varnish at different times. | Fluoride varnish used in the medical setting is effective in reducing ECC in low-income populations but is not cost saving in the first 42 months of life. | Supported by grant (R01DE013949) National Institute of Dental and Craniofacial Research | Strong Quality |
| 8. | Reiss, M.L. [27] | 1976 | United States of America | Trial-Based | 51 children who needed immediate dental care (determined by dental screening at a local school). | 4 | 1. Oral Health Note. 2. Telephone Contact, Home Visit Oral Health education | The 3 Prompt and 1 Prompt plus 5 Incentive was significantly more effective in initiating dental visits than the Note-Only procedure | Not Reported | Moderate Quality |
| 9. | Donaldson, C. [25] | 1986 | United Kingdom | Trial-Based | 161 children who entered the program and attended continuously for a period of 4 years. | 7 | Personal health education, oral fluoride supplements applications of acid phosphate fluoride gel and pit and fissure sealing. | There is a need for further study measuring dental outcome which combine aspects of both the quality and length of life of teeth. | Chief Scientist Office of the Scottish Home and Health Department. | Strong Quality |
| 10. | O’Neill, C. [26] | 2017 | Ireland | Trial-Based | 1096 children aged 2 to 3 year attending general practice assigned in 2-arm parallel group to measure the cost-effectiveness of caries prevention program | 2.5 | 1. Fluoride varnish 2. Toothbrush 3. Oral health advice | This trial raises concerns about the cost-effectiveness of a fluoride-based intervention delivered at the practice level in the context of a state-funded dental service | A state-funded dental service | Strong Quality |
| 11. | Koh, R. [28] | 2015 | Australia | Trial-Based | 296 Children aged 6–60 months. 188 home visit interventions; 58 telephone contact interventions; 40 reference controls: usual home care. | 3.25 | A home visit relative to a telephone call Oral Health advises | Both the home visits and telephone calls were highly cost-effective than no intervention in preventing early childhood caries | National Health and Medical Research Council of Australia | Moderate Quality |
| 12. | Samnaliev, M. [21] | 2015 | United States of America | Model-Based | 518 Children younger than 60 months with active caries or a history of caries | 2.5 | Oral Disease management program | The program appears cost-effective and has the potential to reduce health care costs | Health care costs were obtained from the hospital finance department. And non-health care costs were estimated through a parent survey | Strong Quality |
| 13. | Plonka, K.A. [23] | 2013 | Australia | Model-Based | 325 children were recruited from community health centers, randomly assigned to receive either a home visit or telephone call. | 0.1150 | Oral Health education by the home visit and Telephone call. | Home visits and telephone contacts conducted every 6 months from birth are effective in reducing ECC prevalence by 24 months. | The Dental Board of Queensland and the following Queensland Health Departments | Moderate Quality |
| 14. | Stearns, S.C. [18] | 2012 | United States of America | Model-Based | 209,285 Medicaid enrolled children at age 6 months. | 3.25 | 1. Screening and risk assessment 2. Parental counseling, topical fluoride. 3. Topical fluoride application. | The program is cost-effective with 95% certainty if Medicaid is willing to pay 2331 per hospital episode avoided. | Lead Author is independent of any commercial funder | Strong Quality |
| 15. | Takeuchi, R. [22] | 2017 | Japan | Model-Based | Tongan schoolchildren | 12 | 1. Enforcement of lectures application of fluoride. 2. Instructions on toothbrushing Oral health education. 3. Application of fluoride | The materials for fluoride mouth rinsing and Tooth brushes are lower than for the treatment of caries. | These activities were supported by the JICA | Moderate Quality |
| 16. | Davies, G.M [29] | 2003 | United Kingdom | Trial-Based | A cohort of children aged 12 months was recruited from a high caries risk population in 9 health districts. | 3 | Children received toothpaste 1450 ppm fluoride | The program achieved a significant caries reduction in children who received 1450 fluoride toothpaste. | Not Reported | Moderate Quality |
| 17. | Folayan, M.O. [30] | 2016 | Nigeria | Model-Based | Children living with their biological parents or legal guardians | 6.5 | Dental health education program of home visits | The use of a combination of fluoridated toothpaste and twice-daily tooth brushing had the largest effect on reducing the chance for caries in children resident in Ile-Ife, Nigeria. | Not Reported | Moderate Quality |
| 18. | Lai, B. [31] | 2018 | Singapore | Trial-Based | 90 children and their caregivers participated in the program, and 64 children were recruited as the control group. | 2 | Oral program includes tooth brushing, fluoride use and topical fluoride varnish | The odds of severe early childhood caries in the control group were 3 times higher than that for the intervention group | Not Reported | Moderate Quality |
| 19. | Gibbs, L. [32] | 2015 | Australia | Trial-Based | Families with 1–4-year-old children, 197children in the intervention group and 144 children in the control group Residing in Melbourne. | 2.5 | 1. Community education sessions 2. Follow-up health messages | The Teeth Tales intervention was promising in terms of improving oral hygiene and parent knowledge of tooth brushing technique | Australian Research Council Linkage grant | Moderate Quality |
| Author | Economic Study Design | Year to Which Costs Applied | Currency Used to Which Cost Applied | Outcome: Cost-Effectiveness of the Standardized Year 2015 and USD Currency | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cost of Study Intervention | Cost of Study Control | Incremental Cost | Type of the Outcomes | Effect of Intervention | Effect of Control | |ICER| | Cost Saving | Indirect Cost | Total Program Cost | ||||
| Tickle, M. [24] | Trial-Based | 2015 | £ | $242.76 | $75.15 | $167.61 | DMFT | 1.15 | 1.64 | 342.06 | NA | $1341.93 | $2872.75 |
| Anopa, Y. [19] | Model Based | 2009 | £ | $24.6 | $235.23 | (−) $210.63 | DMFT | 0.08332 | NA | 1621.7 | $737,453.43 | NA | $274,762.01 |
| Koh R. [28] | Trial-Based | 2013 | $ | $354,983.72 | $185,039.65 | (−) $169,944.07 | QALY | 540 | 547 | 24,277.7 | $317,174.06 | $2197.64 | $747,775.07 |
| Reiss, M.L. [27] | Trial-Based | 1976 | $ | $180.95 | $65.65 | $115.30 | Dental Visits | 0.846483 | NA | 32.7 | $208.28 | $122.76 | $66.19 |
| Kowash, M.B. [15] | Model Based | 1995 | £ | $10,046.06 | $46,670.13 | (−) $36.63 | DMFT | 0.29 | 1.75 | 25,085 | $56,716.19 | NA | $20,093.67 |
| Pukallus, M. [16] | Model Based | 2012 | £ | $31,059.39 | $140,146.01 | (−) $109,086.63 | No. of caries teeth prevented | 11 | 54 | 2537 | $109,086.63 | NA | $31,059.39 |
| Quinonez, R.B. [17] | Model Based | 2003 | $ | $234 | $219.92 | $14.08 | cavity free months | 31.49 | 29.97 | 9.26 | NA | NA | $3816.75 |
| Davies, G.M. [29] | Trial-Based | 1992 | £ | $232,664.49 | NA | NA | DMFT | 2.15 | 2.57 | 61.728 | $1845.89 | $16,111.88 | $755,737.89 |
| Hietasalo, P. [5] | Trial-Based | 2004 | € | $602.74 | $518.36 | $84.38 | DMFS | 2.56 | 4.6 | 41.363 | $48.56 | NA | $278,717.29 |
| Takeuchi, R. [22] | Model Based | 2006 | $ | $2806.96 | NA | NA | DMFT | 2.2 | 4.86 | NA | NA | $52.91 | $2859.86 |
| Folayan, M.O. [30] | Model Based | 2015 | ₦ | NA | NA | NA | Probability of less cost | 98.60% | 61.50% | NA | NA | NA | NA |
| Samnaliev, M. [21] | Model Based | 2011 | $ | $71.65 | $8901.61 | (−) $8829.96 | Caries% | 4.15% | 22.50% | 48,119 | $952.54 | $120.73 | $8969.92 |
| Plonka, K.A. [23] | Model Based | NA | $ | NA | NA | NA | Caries% | 2% | 15% | NA | NA | NA | NA |
| Lai, B. [31] | Trial-Based | 2012 | $ | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Blaikie, D.C. [20] | Model Based | 1976 | $ | $13,578,891.38 | $12,640,528.99 | $938,362.38 | Cost-effectiveness ratios | 1.07 | 1.47 | 563,175 | $6,179,117.15 | $278,349.66 | NA |
| O’Neill, C. [26] | Trial-Based | 2014 | £ | $1601.31 | $1271.45 | $329.86 | DMFS | 2.6 | 3.9 | 253.7 | $329.86 | $2429.37 | $2872.75 |
| Stearns, S.C. [18] | Model Based | 2006 | $ | $64.44 | $336.01 | (−) $271.58 | No. of IMB visits | 4 | 0 | 68 | $39.55 | NA | $40.96 |
| Gibbs, L. [32] | Trial-Based | 2012 | $ AU | NA | NA | NA | Percentage of not having debris | 56% | Referent | NA | NA | NA | $296,651.45 |
| Donaldson, C. [25] | Trial-Based | 1974 | £ | NA | NA | $346.01 | DMFT | 0.37 | 2.47 | 3.4 | NA | NA | NA |
| Drummond Checklist/Study Authors | Anopa, Y. [19] | Blaikie, D.C. [20] | Kowash, M.B. [15] | Stearns, S.C. [18] | Samnaliev, M. [21] | Pukallus, M. [16] | Quinoez, R.B. [17] | Plonka, K.A. [23] | Folayan, M.O. [30] | Takeuchi, R. [22] |
|---|---|---|---|---|---|---|---|---|---|---|
| Was a Well-Defined Question Posed in an Answerable Form? | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes |
| Was a Comprehensive Description of the Competing Alternatives Given? | yes | yes | yes | yes | yes | yes | yes | yes | yes | no |
| Was the Effectiveness of the Program Established? | yes | yes | yes | yes | yes | yes | no | yes | yes | yes |
| Were All the Important and Relevant Costs and Consequences for Each Alternative Identified? | yes | yes | yes | yes | yes | yes | yes | no | NA | no |
| Were Costs and Consequences Measured Accurately in Appropriate Physical Units? | yes | yes | yes | yes | yes | yes | yes | NA | NA | yes |
| Were Costs and Consequences Valued Credibly? | yes | yes | yes | yes | yes | yes | yes | NA | NA | yes |
| Were Costs and Consequences Adjusted for Differential Timing? | yes | yes | no | yes | NA | yes | yes | NA | NA | NA |
| Was an Incremental Analysis of Costs and Consequences of Alternatives Performed? | yes | yes | yes | yes | yes | yes | yes | NA | NA | NA |
| Was Allowance Made for Uncertainty in the Estimates of Costs and Consequences? | no | no | no | yes | NA | no | no | NA | NA | NA |
| Did the Presentation and Discussion of Study Results Include All Issues of Concern to Users? | yes | yes | yes | yes | yes | yes | yes | yes | yes | Yes |
| Score | 9 from 10 | 9 from 10 | 7 form 10 | 10 from 10 | 8 from 10 | 9 from 10 | 8 from 10 | 4 from 10 | 4 from 10 | 5 from 10 |
| Drummond Checklist/Study Authors | Donaldson, C. [25] | Davies, G.M. [29] | Koh R. [28] | Hietasalo P. [5] | O’Neill, C. [26] | Tickle, M. [24] | Reiss, M.L. [27] | Lai, B. [31] | Gibbs, L. [32] |
|---|---|---|---|---|---|---|---|---|---|
| Was a Well-Defined Question Posed in an Answerable Form? | yes | yes | yes | yes | yes | yes | yes | yes | yes |
| Was a Comprehensive Description of the Competing Alternatives Given? | yes | no | yes | yes | yes | yes | yes | yes | no |
| Was the Effectiveness of the Program Established? | yes | yes | yes | yes | no | no | yes | yes | yes |
| Were All the Important and Relevant Costs and Consequences for Each Alternative Identified? | no | no | yes | yes | yes | yes | no | NA | yes |
| Were Costs and Consequences Measured Accurately in Appropriate Physical Units? | yes | yes | yes | yes | yes | yes | yes | NA | yes |
| Were Costs and Consequences Valued Credibly? | yes | yes | yes | yes | yes | yes | yes | NA | yes |
| Were Costs and Consequences Adjusted for Differential Timing? | yes | yes | no | NA | yes | NA | No | NA | NA |
| Was an Incremental Analysis of Costs and Consequences of Alternatives Performed? | yes | no | yes | yes | yes | yes | No | NA | NA |
| Was Allowance Made for Uncertainty in the Estimates of Costs and Consequences? | yes | NA | yes | yes | yes | yes | NA | NA | NA |
| Did the Presentation and Discussion of Study Results Include All Issues of Concern to Users? | no | No | yes | yes | yes | yes | yes | yes | no |
| Score | 8 from 10 | 5 from 10 | 9 from 10 | 9 from10 | 9 from 10 | 8 from 10 | 6 from 10 | 4 from 10 | 5 from 10 |
Appendix B






References
- Petersen, P.E. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century—The approach of the WHO Global Oral Health Programme. Commun. Dent. Oral Epidemiol. 2003, 31, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Artnik, B. Health Promotion and Disease Prevention: A Handbook for Teachers, Researchers, Health Professionals and Decision Makers; Hans Jacobs Publishing Company: Lage, Germany, 2008; pp. 1–13. [Google Scholar]
- Grossi, S.G.; Genco, R.J. Periodontal disease and diabetes mellitus: A two-way relationship. Ann. Periodontol. 1998, 3, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Listl, S.; Birch, S. International Health Economics Association, 9th World Congress on Health Economics: Celebrating Health Economics; Dental Health Economics: Sydney, Australia, 2013. [Google Scholar]
- Hietasalo, P.; Seppa, L.; Lahti, S.; Niinimaa, A.; Kallio, J.; Aronen, P.; Sintonen, H.; Hausen, H. Cost-effectiveness of an experimental caries-control regimen in a 3.4-yr randomized clinical trial among 11–12-yr-old Finnish schoolchildren. Eur. J. Oral Sci. 2009, 117, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef]
- Newacheck, P.W.; Hughes, D.C.; Hung, Y.Y.; Wong, S.; Stoddard, J.J. The unmet health needs of America’s children. Pediatrics 2000, 105, 989–997. [Google Scholar] [PubMed]
- Colombo, S.; Ferrazzan, G.F.; Beretta, M.; Paglia, L. Dental Caries Prevention: A Review on the Use of Dental Sealants. Available online: http://www.dentalmedjournal.it/files/2018/12/[email protected] (accessed on 23 July 2019).
- Bagramian, R.A.; Garcia-Godoy, F.; Volpe, A.R. The global increase in dental caries. A pending public health crisis. Am. J. Dent. 2009, 22, 3–8. [Google Scholar] [PubMed]
- Asvall, J.E. The Health for All Policy Framework for the Who European Region. European Health for All Series, No.6; WHO, Regional Office for Europe: Copenhagen, Denmark, 1998; pp. 11–34. [Google Scholar]
- Robles, A.; Upegui, A.; Simbaqueba, E.; Zarama, P. A First study to determine the economic impact of Dental Cavities in Colombia for 2011. Value Health J. 2015, 18, A180. [Google Scholar] [CrossRef]
- Brown, E. Children’s Dental Visits and Expenses, United States, 2003; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2006; pp. 1–7. [Google Scholar]
- Luhnen, M.; Prediger, B.; Neugebauer, E.A.M.; Mathes, T. Systematic reviews of health economic evaluations: A protocol for a systematic review of characteristics and methods applied. Syst. Rev. 2017, 6, 238. [Google Scholar] [CrossRef] [PubMed]
- Charles, J.; Edwards, R.T. A Guide to Health Economics for Those Working in Public Health; Bangor University: Bangor, UK, 2016; pp. 2–27. [Google Scholar]
- Kowash, M.B.; Toumba, K.J.; Curzon, M.E. Cost-effectiveness of a long-term dental health education program for the prevention of early childhood caries. Eur. Arch. Paediatr. Dent. 2006, 7, 130–135. [Google Scholar] [CrossRef]
- Pukallus, M.; Plonka, K.; Kularatna, S.; Gordon, L.; Barnett, A.G.; Walsh, L.; Seow, W.K. Cost-effectiveness of a telephone-delivered education programme to prevent early childhood caries in a disadvantaged area: A cohort study. BMJ Open 2013, 3. [Google Scholar] [CrossRef]
- Quinonez, R.B.; Stearns, S.C.; Talekar, B.S.; Rozier, R.G.; Downs, S.M. Simulating cost-effectiveness of fluoride varnish during well-child visits for medicaid-enrolled children. Arch. Pediatr. Adolesc. Med. 2006, 160, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Stearns, S.C.; Rozier, R.G.; Kranz, A.M.; Pahel, B.T.; Quiñonez, R.B. Cost-effectiveness of preventive oral health care in medical offices for young medicaid enrollees. Arch. Pediatr. Adolesc. Med. 2012, 166, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Anopa, Y.; McMahon, A.D.; Conway, D.I.; Ball, G.E.; McIntosh, E.; Macpherson, L.M.D. Improving child oral health: Cost analysis of a national nursery toothbrushing programme. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Blaikie, D.C. The cost of school dental care: A preliminary economic analysis. Aust. Dent. J. 1977, 23, 146–151. [Google Scholar] [CrossRef]
- Samnaliev, M.; Wijeratne, R.; Kwon, E.G.; Ohiomoba, H.; Ng, M.W. Cost-effectiveness of a disease management program for early childhood caries. J. Public Health Dent. 2015, 75, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, R.; Kawamura, K.; Kawamura, S.; Endoh, M.; Uchida, C.; Taguchi, C.; Nomoto, T.; Hiratsuka, K.; Fifita, S.; Fakakovikaetau, A.; et al. Evaluation of the child oral health promotion ‘MaliMali’ Programme based on schools in the Kingdom of Tonga. Int. Dent. J. 2017, 67, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Plonka, K.A.; Pukallus, M.L.; Barnett, A.; Holcombe, T.F.; Walsh, L.J.; Seow, W.K. A controlled, longitudinal study of home visits compared to telephone contacts to prevent early childhood caries. Int. J. Paediatr. Dent. 2013, 23, 23–31. [Google Scholar] [CrossRef]
- Tickle, M.; O’Neill, C.; Donaldson, M.; Birch, S.; Noble, S.; Killough, S.; Murphy, L.; Greer, M.; Brodison, J.; Verghis, R.; et al. A randomised controlled trial to measure the effects and costs of a dental caries prevention regime for young children attending primary care dental services: The Northern Ireland Caries Prevention In Practice (NIC-PIP) trial. Health Technol. Assess. 2016, 20, 1–96. [Google Scholar] [CrossRef]
- Donaldson, C.; Forbes, J.F.; Smalls, M.; Boddy, F.A.; Stephen, K.W.; McCall, D. Preventive dentistry in a health centre: Effectiveness and cost. Soc. Sci. Med. 1986, 23, 861–868. [Google Scholar] [CrossRef]
- O’Neill, C.; Worthington, H.V.; Donaldson, M.; Birch, S.; Noble, S.; Killough, S.; Murphy, L.; Greer, M.; Brodison, J.; Verghis, R.; et al. Cost-effectiveness of caries prevention in practice: A randomized controlled trial. J. Dent. Res. 2017, 96, 875–880. [Google Scholar] [CrossRef]
- Reiss, M.L.; Piotrowski, W.D.; Bailey, J.S. Behavioral community psychology: Encouraging low-income parents to seek dental care for their children. J. Appl. Behav. Anal. 1976, 9, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Koh, R.; Pukallus, M.; Kularatna, S.; Gordon, L.G.; Barnett, A.G.; Walsh, L.J.; Seow, W.K. Relative cost-effectiveness of home visits and telephone contacts in preventing early childhood caries. Commun. Dent. Oral Epidemiol. 2015, 43, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Davies, G.M.; Worthington, H.V.; Ellwood, R.P.; Blinkhorn, A.S.; Taylor, G.O.; Davies, R.M.; Considine, J. An assessment of the cost effectiveness of a postal toothpaste programme to prevent caries among five-year-old children in the North West of England. Commun. Dent. Health 2003, 20, 207–210. [Google Scholar] [PubMed]
- Folayan, M.O.; Kolawole, K.A.; Chukwumah, N.M.; Oyedele, T.; Agbaje, H.O.; Onyejaka, N.; Oziegbe, E.O.; Oshomoji, O.V. Use of caries prevention tools and associated caries risk in a suburban population of children in Nigeria. Eur. Arch. Paediatr. Dent. 2016, 17, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Lai, B.; Tan, W.K.; Lu, Q.S. Clinical efficacy of a two-year oral health programme for infants and toddlers in Singapore. Singapore Med. J. 2018, 59, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Gibbs, L.; Waters, E.; Christian, B.; Gold, L.; Young, D.; de Silva, A.; Calache, H.; Gussy, M.; Watt, R.; Riggs, E.; et al. Teeth tales: A community-based child oral health promotion trial with migrant families in Australia. BMJ Open 2015, 5, e007321. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Centres, S.; Galloway, J.; Mossey, P.A.; Marcenes, W. Global economic impact of dental diseases. J. Dent. Res. 2015, 94, 1355–1361. [Google Scholar] [CrossRef]










© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fraihat, N.; Madae’en, S.; Bencze, Z.; Herczeg, A.; Varga, O. Clinical Effectiveness and Cost-Effectiveness of Oral-Health Promotion in Dental Caries Prevention among Children: Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2668. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152668
Fraihat N, Madae’en S, Bencze Z, Herczeg A, Varga O. Clinical Effectiveness and Cost-Effectiveness of Oral-Health Promotion in Dental Caries Prevention among Children: Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(15):2668. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152668
Chicago/Turabian StyleFraihat, Nadine, Saba Madae’en, Zsuzsa Bencze, Adrienn Herczeg, and Orsolya Varga. 2019. "Clinical Effectiveness and Cost-Effectiveness of Oral-Health Promotion in Dental Caries Prevention among Children: Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 15: 2668. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152668