New Patterns of Information and Communication Technologies Usage at Work and Their Relationships with Visual Discomfort and Musculoskeletal Diseases: Results of a Cross-Sectional Study of Spanish Organizations

 , , , and
, , , and
Abstract
:1. Introduction
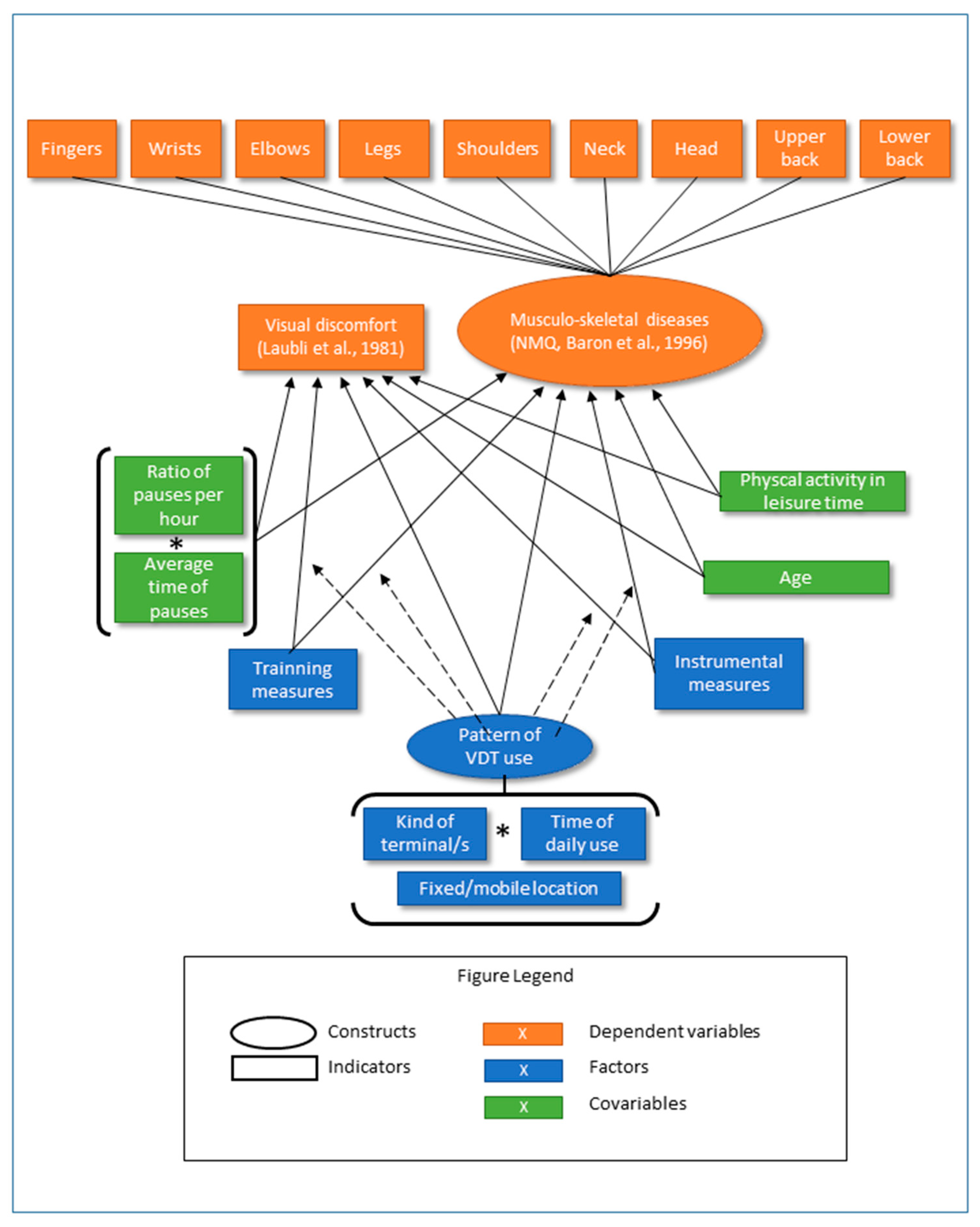
2. Conceptual Framework and Hypothesis
3. Materials and Methods
3.1. Subjects
3.2. Variables and Instruments
3.3. Procedure
3.4. Data Analysis
4. Results
4.1. Descriptive Statistics and Reliability Results
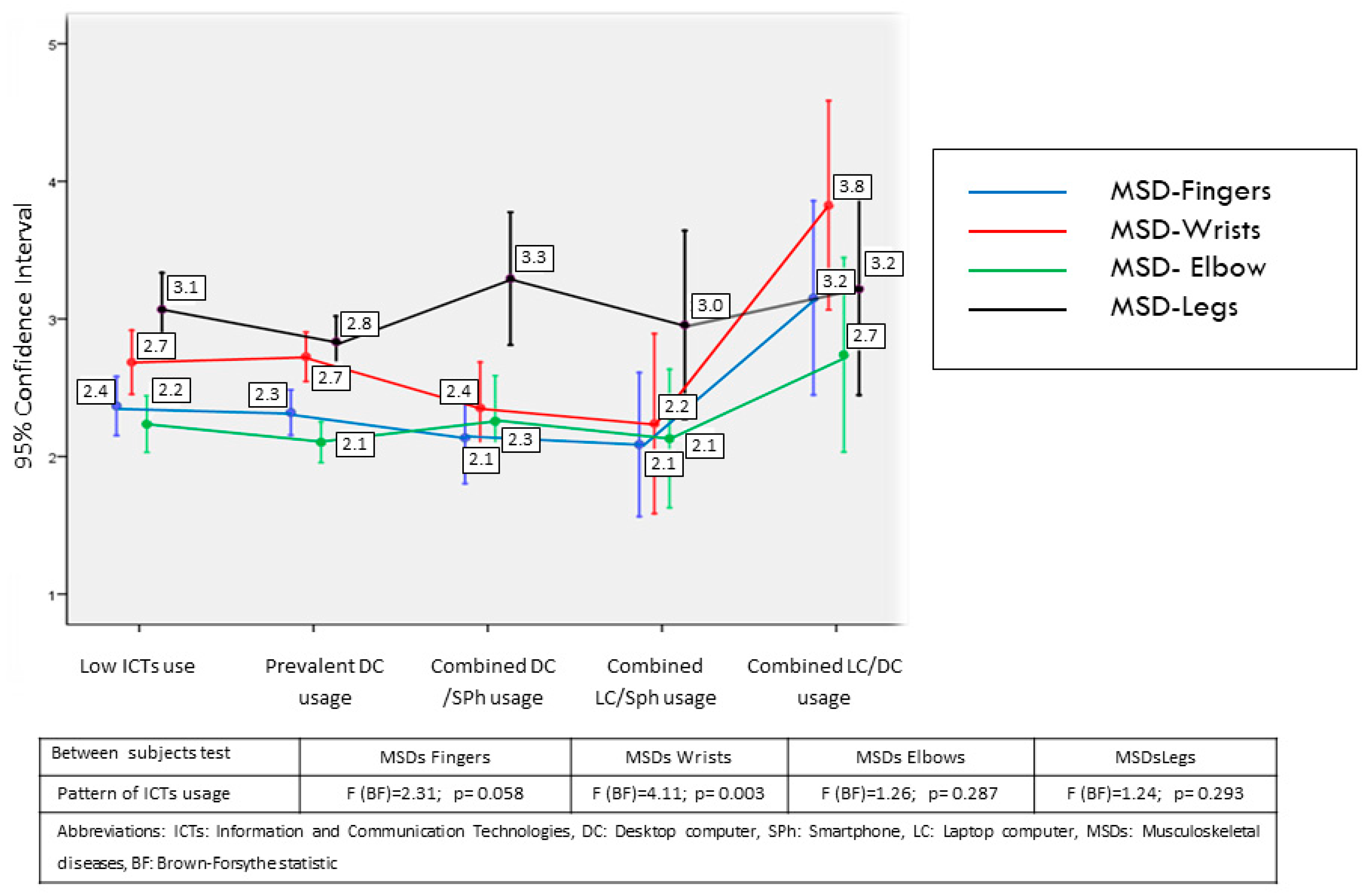
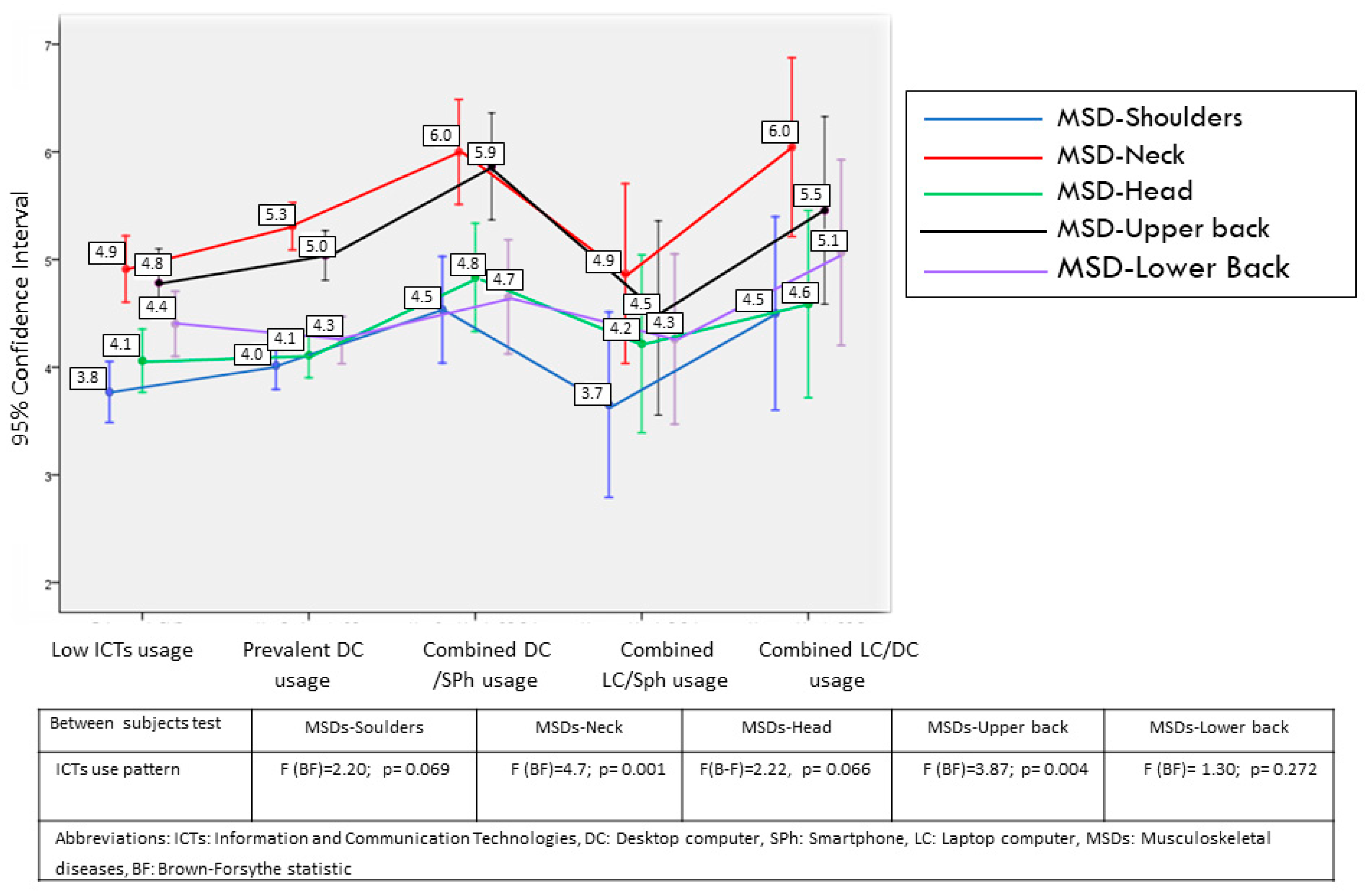
4.2. Cluster Analysis of the Usage Patterns of ICTs
- Low ICT Usage: Group of workers who do not use ICTs very much, with one third of workers in a fixed post.
- Preferred use of DC: group of workers that preferentially uses the DC and works in a predominantly fixed post.
- Combined use of DC and SPh: group of workers who use the DC and SPh equally with almost one half of the workers in a fixed post.
- Combined use of LC and SPh: Group of workers that uses a LC and a SPh equally, with a large majority of the workers in a mobile post.
- Combined use of DC and LC: Group of workers who use a DC and a LC equally, with one third of the workers in a fixed post.
4.3. Relationships of Usage Patterns with MSDs and Visual Discomfort
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ICT Usage Pattern | ||||||
|---|---|---|---|---|---|---|
| Socio-Demographic Characteristics and Job Profile | Low ICT Usage | Preferred Use of DC | Combined Use of DC and SPh | Combined Use of LC and SPh | Combined Use of DC and LC | |
| % (n) | % (n) | % (n) | % (n) | % (n) | ||
| Sex (LR = 6.47; p = 0.165) | Male | 47.7 (174) | 42.3 (283) | 36.8(49) | 47.8 (22) | 50.0 (23) |
| Female | 52.3 (191) | 57.7 (386) | 63.2 (84) | 52.2 (24) | 50.0 (23) | |
| Type of job (LR = 155.0; p < 0.001) | Management, administration, reception | 43.3 (158) | 75.9 (508) + | 62.4 (83) | 37.0 (17) − | 47.8 (22) − |
| Production, operator | 9.6 (35) | 1.5 (10) − | 3.8 (5) | 6.5 (3) | 6.5 (3) | |
| Commercial department | 1.6 (6) | 1.5 (10) | 4.5 (6) + | 4.3 (2) | 4.3 (2) | |
| Services and activities | 8.2 (30) | 2.5 (17) − | 2.3 (3) | 15.2 (7) + | 8.7 (4) | |
| Others | 37.3 (136) | 18.5 (124) − | 27.1 (36) | 37.0 (17) | 32.6 (15) | |
| Sector of activity (LR = 15.3; p = 0.146) | Agriculture | 3.3 (12) | 2.8(19) | 2.3 (3) | 2.2 (1) | 0.0 (0) |
| Construction | 12.3 (45) | 9.3(62) | 6.0 (8) | 13.0 (6) | 6.5 (3) | |
| Industry | 15.1 (55) | 20.2(135) | 18.8 (25) | 10.9 (5) | 10.9 (5) | |
| Services | 69.3 (253) | 67.7(453) | 72.9 (97) | 73.9 (34) | 82.6 (38) + | |
| Job tenure (LR = 23.5; p = 0.100) | Less than 1 year | 4.9 (18) | 3.4(23) | 3.0 (4) | 2.2 (1) | 8.7 (4) |
| 1−5 years | 27.1 (99) | 29.6(198) | 34.6 (46) | 45.7 (21) + | 21.7 (10) | |
| 6−10 years | 12.3 (45) | 13.5(90) | 15.0 (20) | 10.9 (5) | 15.2 (7) | |
| 11−15 years | 18.4 (67) | 15.2(102) | 15.0 (20) | 26.1 (12) | 15.2 (7) | |
| >15 years | 37.3 (136) | 38.3 (256) | 32.3 (43) | 15.2 (7) − | 39.1 (18) | |
| Age (F = 1.95; p = 0.035) | Mean (SD) | Mean (SD) | SD | Mean (SD) | Mean (SD) | |
| 44.68 (8.6) | 42.89 (9.28) | 43.56 (8.68) | 41.50 (9.00) | 41.87 (8.65) | ||
| Dependent Variables | Factors | Covariates |
|---|---|---|
| Visual discomfort MSDs | ICT usage pattern TM1. Appropriate devices or equipment for the task being performed TM2. The company carried out a specific occupational hazard assessment for working with these devices TM3. Furniture that allows adopting an adequate posture to perform the task TM4. Lecterns, footrests, or other contributing elements to improve posture in front of the computer TM5. Accessory Element(s) (Lecterns, stands ...) in order to adopt an appropriate position when using smartphones/tablets TRM1. General training on prevention of occupational hazards TRM2. Training related to computer use TRM3. Training related to the use of other devices ICT usage pattern TM1 ICT usage pattern TM2 ICT usage pattern TM3 ICT usage pattern TM4 ICT usage pattern TM5 ICT usage pattern TRM1 ICT usage pattern TRM2 ICT usage pattern TRM3 | Age Physical activity outside the work setting Average pause time Ratio pauses per hour Average pause time ratio pauses per hour |
References
- European Agency for Safety and Health at Work (EU-DCHA). Review of Drivers and Trends of Change in Information and Communication Technologies and Work Location. 2016. Available online: https://osha.europa.eu/en/tools-and-publications/publications/key-trends-and-drivers-change-information-and-communication (accessed on 10 October 2018).
- European Agency for Safety and Health at Work (EU-DCHA). Key Trends and Drivers of Change in Information and Communication Technologies and Work Location. 2017. Available online: https://osha.europa.eu/es/tools-and-publications/publications/key-trends-and-drivers-change-information-and-communication/view (accessed on 10 October 2018).
- Derks, D.; Bakker, A.B.; Peters, P.; van Wingerden, P. Work-related smartphone use, work–family conflict and family role performance: The role of segmentation preference. Hum. Relat. 2016, 69, 1045–1068. [Google Scholar] [CrossRef]
- Xie, Y.; Ma, H.; Zhou, Z.E.; Tang, H. Work-related use of information and communication technologies after hours (W_ICTs) and emotional exhaustion: A mediated moderation model. Comput. Hum. Behav. 2018, 79, 94–104. [Google Scholar] [CrossRef]
- So, C.B.; Cheng, S.A.; Szeto, P.G. Cumulative IT Use Is Associated with Psychosocial Stress Factors and Musculoskeletal Symptoms. Int. J. Environ. Res. Public Health 2017, 14, 1541. [Google Scholar] [CrossRef] [PubMed]
- Woo, E.H.C.; White, P.; Lai, C.W.K. Musculoskeletal impact of the use of various types of electronic devices on university students in Hong Kong: An evaluation by means of self-reported questionnaire. Man. Ther. 2016, 26, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, Y.; Ferdous, A.S.; Sekiguchi, T.; Sugianto, L.F. The effect of mobile technology usage on work engagement and emotional exhaustion in Japan. J. Bus. Res. 2016, 69, 3315–3323. [Google Scholar] [CrossRef]
- Gold, J.E.; Driban, J.B.; Thomas, N.; Chakravarty, T.; Channell, V.; Komaroff, E. Postures, typing strategies, and gender differences in mobile device usage: An observational study. Appl. Ergon. 2012, 43, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, E.; Coenen, P.; Campbell, A.; Straker, L. Texting with touchscreen and keypad phones—A comparison of thumb kinematics, upper limb muscle activity, exertion, discomfort, and performance. Appl. Ergon. 2018, 70, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, E.; Thomée, S.; Grimby-Ekman, A.; Hagberg, M. Texting on mobile phones and musculoskeletal disorders in young adults: A five-year cohort study. Appl. Ergon. 2017, 58, 208–214. [Google Scholar] [CrossRef]
- Ciccarelli, M.; Straker, L.; Mathiassen, S.E.; Pollock, C. Posture variation among office workers when using different information and communication technologies at work and away from work. Ergonomics 2014, 57, 1678–1686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, K.; Ciccarelli, M.; Falkmer, T.; Parsons, R. Associations between exposure to information and communication technology (ICT) and reported discomfort among adolescents. Work 2014, 48, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Szeto, G.; Dai, J. Prevalence and risk factors associated with musculoskeletal complaints among users of mobile handheld devices: A systematic review. Appl. Ergon. 2017, 59, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Christensen, J.O.; Nielsen, M.B.; Finne, L.B.; Knardahl, S. Comprehensive profiles of psychological and social work factors as predictors of site-specific and multi-site pain. Scand. J. Work Environ. Health 2018, 44, 291–302. [Google Scholar] [CrossRef] [Green Version]
- Olson, C.L. Practical considerations in choosing a MANOVA test statistic: A rejoinder to Stevens. Psychol. Bull. 1979, 86, 1350–1352. [Google Scholar] [CrossRef]
- Bates, P.; Huws, U. Modelling eWork in Europe: Estimates, Models and Forecasts from the EMERGENCE Project. IES Report. Grantham Book Services, 2002. Available online: http://www.employment-studies.co.uk (accessed on 10 October 2018).
- Paridon, H.M.; Hupke, M. Psychosocial Impact of Mobile Telework: Results from an Online Survey. Eur. J. Psychol. 2009, 5. [Google Scholar] [CrossRef]
- Robertson, M.M.; Huang, Y.-h.; Larson, N. The relationship among computer work, environmental design, and musculoskeletal and visual discomfort: Examining the moderating role of supervisory relations and co-worker support. Int. Arch. Occup. Environ. Health 2016, 89, 7–22. [Google Scholar] [CrossRef]
- Delp, L.; Wang, P.C. Musculoskeletal disorders among clerical workers in Los Angeles: A labor management approach. Am. J. Ind. Med. 2013, 56, 1072–1081. [Google Scholar] [CrossRef] [PubMed]
- Klussmann, A.; Gebhardt, H.; Liebers, F.; Rieger, M.A. Musculoskeletal symptoms of the upper extremities and the neck: A cross-sectional study on prevalence and symptom-predicting factors at visual display terminal (VDT) workstations. BMC Musculoskelet. Disord. 2008, 9, 96. [Google Scholar] [CrossRef]
- Oha, K.; Animägi, L.; Pääsuke, M.; Coggon, D.; Merisalu, E. Individual and work-related risk factors for musculoskeletal pain: A cross-sectional study among Estonian computer users. BMC Musculoskelet. Disord. 2014, 15, 181. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; He, L.; Li, J.; Wang, J.; Wang, S. Visual Display Terminal Use Increases the Prevalence and Risk of Work-related Musculoskeletal Disorders among Chinese Office Workers: A Cross-sectional Study. J. Occup. Health 2012, 54, 34–43. [Google Scholar] [CrossRef]
- Brewer, S.; Van Eerd, D.; Amick, B.C.; Irvin, E.; Daum, K.M.; Gerr, F.; Moore, J.S.; Cullen, K.; Rempel, D. Workplace interventions to prevent musculoskeletal and visual symptoms and disorders among computer users: A systematic review. J. Occup. Rehabil. 2006, 16, 325–358. [Google Scholar] [CrossRef]
- Molina Aragonés, J.M.; Forns Carbonell, J.; Rodriguez Moreno, J.M.; Vidiella, S.; Manuel, J.; López Pérez, C. Revisión sistemática sobre las alteraciones óculo-visuales y músculo-esqueléticas asociadas al trabajo con pantallas de visualización de datos [Systematic review of occular-visual and musculoskeletal disorders associated with working with visual display terminals]. Med. Segur. Trab. 2017, 63, 167–205. [Google Scholar]
- Bongers, P.M.; Ijmker, S.; van den Heuvel, S.; Blatter, B.M. Epidemiology of work related neck and upper limb problems: Psychosocial and personal risk factors (part I) and effective interventions from a bio behavioural perspective (part II). J. Occup. Rehabil. 2006, 16, 279–302. [Google Scholar] [CrossRef] [PubMed]
- Stock, S.R.; Nicolakakis, N.; Vezina, N.; Vezina, M.; Gilbert, L.; Turcot, A.; Sultan-Taieb, H.; Sinden, K.; Denis, M.A.; Delga, C.; et al. Are work organization interventions effective in preventing or reducing work-related musculoskeletal disorders? A systematic review of the literature. Scand. J. Work Environ. Health 2018, 44, 113–133. [Google Scholar] [CrossRef] [PubMed]
- Blehm, C.; Vishnu, S.; Khattak, A.; Mitra, S.; Yee, R.W. Computer vision syndrome: A review. Surv. Ophthalmol. 2005, 50, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Rojas-Rueda, D.; Alonso, J.; Antó, J.M.; Cardona, P.J.; Fernández, E.; Garcia-Basteiro, A.L.; Benavides, F.G.; Glenn, S.D.; Krish, V.; et al. La carga de enfermedad en España: Resultados del Estudio de la Carga Global de las Enfermedades 2016. Med. Clin. 2018, 151, 171–190. [Google Scholar] [CrossRef]
- Mikkelsen, S.; Lassen, C.F.; Vilstrup, I.; Kryger, A.I.; Brandt, L.P.A.; Thomsen, J.F.; Gerster, M.; Grimstrup, S.; Andersen, J.H. Does computer use affect the incidence of distal arm pain? A one-year prospective study using objective measures of computer use. Int. Arch. Occup. Environ. Health 2012, 85, 139–152. [Google Scholar] [CrossRef] [PubMed]
- Wærsted, M.; Hanvold, T.N.; Veiersted, K.B. Computer work and musculoskeletal disorders of the neck and upper extremity: A systematic review. BMC Musculoskelet. Disord. 2010, 11, 79. [Google Scholar] [CrossRef]
- Taib, M.F.; Bahn, S.; Yun, M.H. The effect of psychosocial stress on muscle activity during computer work: Comparative study between desktop computer and mobile computing products. Work 2016, 54, 543–555. [Google Scholar] [CrossRef] [Green Version]
- Fogleman, M.; Lewis, R.J. Factors associated with self-reported musculoskeletal discomfort in video display terminal (VDT) users. Int. J. Ind. Ergon. 2002, 29, 311–318. [Google Scholar] [CrossRef]
- Dalkılınç, M.; Kayihan, H. Efficacy of Web-Based [E-Learning] Office Ergonomics Training: A Test Study. J. Musculoskelet. Pain 2014, 22, 275–285. [Google Scholar] [CrossRef]
- Mani, K.; Provident, I.; Eckel, E. Evidence-based ergonomics education: Promoting risk factor awareness among office computer workers. Work 2016, 55, 913–922. [Google Scholar] [CrossRef] [PubMed]
- Rasoulzadeh, Y.; Gholamnia, R. Effectiveness of an Ergonomics Training Program on Decreasing Work-Related Musculoskeletal Disorders Risk among Video Display Terminals Users. Health Promot. Perspect. 2012, 2, 89–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanaeinasab, H.; Saffari, M.; Valipour, F.; Alipour, H.R.; Sepandi, M.; Al Zaben, F.; Koenig, H.G. The effectiveness of a model-based health education intervention to improve ergonomic posture in office computer workers: A randomized controlled trial. Int. Arch. Occup. Environ. Health 2018, 91, 951–962. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N.; Elovainio, M.; De Nardis, I.; Heponiemi, T.; Bergamaschi, A. Environmental discomfort and musculo-skeletal disorders. Occup. Med. 2011, 61, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Chirico, F.; Rulli, G. Thermal comfort and indoor air quality in some of the Italian State Police workplaces. G. Ital. Med. Lav. Ergon. 2017, 39, 230–239. [Google Scholar] [PubMed]
- Magnavita, N. Perceived job strain, anxiety, depression and musculo-skeletal disorders in social care workers. G. Ital. Med. Lav. Ergon. 2009, 31 (1 Suppl. A), A24–A29. [Google Scholar] [PubMed]
- Smith, M.J. Psychosocial aspects of working with video display terminals (VDTs) and employee physical and mental health. Ergonomics 1997, 40, 1002–1015. [Google Scholar] [CrossRef] [PubMed]
- NRC. Musculoskeletal Disorders, the Workplace: Low Back, Upper Extremities; National Academy Press: Washington, DC, USA, 2001.
- Magnavita, N. Work-related symptoms in indoor environments: A puzzling problem for the occupational physician. Int. Arch. Occup. Environ. Health 2015, 88, 185–196. [Google Scholar] [CrossRef]




| Socio-demographic data: | Sex, age |
| Job data: | Sector of activity, type of job, job tenure. |
| ICT usage in the work activity: | Average daily usage time (hours) of the following types of technologies for work-related activities: desktop, laptop, tablet, and smartphone. Average number of daily pauses in ICT usage (informed by subjects) Average duration of pauses in ICT usage (informed by subjects) Place of usage of ICT devices (Only fixed posts at work; home office; other spaces at home, public places; other spaces) |
| Preventive measures taken | Technical measures (TM): Check-list (Yes/No) about the availability of:
|
Training measures: (TRM): check-list (Yes/No) about the availability in the company of:
| |
| Indicators of occupational health | Visual discomfort: rating scale from 1 (lowest intensity) to 10 (highest intensity) of seven descriptives to collect a subjective rating of visual discomfort after device use (Laubli, Hunting, & Grandjean, 1981; Saito et al., 1994): (a) “My eyes feel tired (visual fatigue)”; (b) “Eyes dry, irritated or burning”; (c) “Eye pain”; (d) “Hard to focus”; (e) “Double vision on screen”; (f) “Flicker vision”; and (g) “Headache”. |
| Musculo skeletal disorders (MSDs): Nordic Musculoskeletal Questionnaire (NMQ), (Baron, Hales & Hurrell, 1996). Check-list of 9 items referring to pain or discomfort perceived by workers in different body parts suffered for seven days following the use of ICTs. Response scale ranging from 1 (no pain or discomfort) to 10 (maximum intensity of pain or discomfort). | |
| Performance of physical activity out of the work setting: | Item that shows the extent to which workers practice hobbies or intensive sports activities, play musical instruments or practice activities with instruments that produce vibrations (lawnmower, motor saw, DIY tools, etc.) in their free time. Scale from 0 to 10 points. |
| ICT Usage | Mean | Standard Deviation |
|---|---|---|
| Average time (hours) of daily usage of desktop computer | 4.44 | 2.99 |
| Average time (hours) of daily usage of laptop | 1.15 | 2.14 |
| Average time (hours) of daily usage of Tablet | 0.21 | 0.83 |
| Average time (hours) of daily usage of Smartphone | 1.79 | 2.47 |
| Pause ratio for total hours of ICT usage (pauses/hour) | 0.73 | 1.05 |
| Average time per pause (minutes) in ICT usage | 3.87 | 17.39 |
| Preventive Measures | No | Yes | ||
|---|---|---|---|---|
| n | % | n | % | |
| Technical Measures (TM) | ||||
| TM1. Appropriate devices or equipment for the task being performed | 490 | (39.0%) | 765 | (61.0%) |
| TM2. The company carried out a specific occupational hazard assessment for working with these devices | 535 | (42.6%) | 720 | (57.4%) |
| TM3. Furniture that allows adopting an adequate posture to perform the task | 412 | (32.8%) | 843 | (67.2%) |
| TM4. Lecterns, footrests or other contributing elements to improve posture in front of the computer | 743 | (60.0%) | 496 | (40.0%) |
| TM5. accessory element/s (lecterns, stands...) that allow adopting an adequate posture when using smartphones/tablets | 1024 | (81.6%) | 231 | (18.4%) |
| Training measures (TRM) | ||||
| TRM1. General training on prevention of occupational hazards | 199 | (15.8%) | 1060 | (84.2%) |
| TRM2. Training related to computer use | 748 | (59.4%) | 511 | (40.6%) |
| TRM3. Training related to the use of other devices | 1067 | (84.7%) | 192 | (15.3%) |
| Visual Discomfort and MSDs Measures | Mean | Standard Deviation | Reliability (Cronbach’s Alpha) | |
|---|---|---|---|---|
| Visual discomfort: From 1 (lowest intensity) to 10 (highest intensity) | 3.60 | 2.25 | 0.905 | |
| MSDs: From 1 (no pain or discomfort) to 10 (maximum intensity of pain or discomfort) | MSDs Fingers | 2.34 | 2.12 | - |
| MSDs Wrists | 2.70 | 2.30 | - | |
| MSDs Elbows | 2.18 | 1.97 | - | |
| MSDs Shoulders | 4.00 | 2.89 | - | |
| MSDs Neck | 5.28 | 2.92 | - | |
| MSDs Head | 4.19 | 2.82 | - | |
| MSDs Upper Back | 5.05 | 3.04 | - | |
| MSDs Lower Back | 4.37 | 2.91 | - | |
| MSDs Legs | 2.97 | 2.53 | - | |
| ICT Usage Pattern | ||||||
|---|---|---|---|---|---|---|
| Usage of Specific Devices and Mobility | Low ICT Usage | Preferential DC Usage | Combined DC-Sph Usage | Combined LC-Sph Usage | Combined DC-LP Usage | |
| Total Frequency | Row% (n) | 29.0 (365) | 53.1 (669) | 10.6 (133) | 3.7 (46) | 3.7 (46) |
| Mean | Mean | Mean | Mean | Mean | ||
| Average usage time (hours) of different devices at work | Desk Computer | 0.7 | 6.3 | 6.6 | .5 | 5.2 |
| Laptop Computer | 2.2 | 0.2 | 0.6 | 5.3 | 5.0 | |
| Tablet | 0.2 | 0.1 | 0.3 | 1.6 | 0.8 | |
| Smart Phone | 1.3 | 0.6 | 6.7 | 7.7 | 2.6 | |
| % (n) | % (n) | % (n) | % (n) | % (n) | ||
| Mobility in the work post | 100% in a fixed physical post | 32.9 (120) | 69.5 (465) | 47.4 (63) | 19.6 (9) | 32.6 (15) |
| 75% fixed-25% mobile | 20.8 (76) | 19.7 (132) | 21.8 (29) | 19.6 (9) | 28.3 (13) | |
| 50% fixed-50% mobile | 26.3 (96) | 9.9 (66) | 21.8 (29) | 37.0 (17) | 32.6 (15) | |
| 25% fixed-75% mobile | 12.9 (47) | 0.9 (6) | 4.5 (6) | 15.2 (7) | 6.5 (3) | |
| 100% Mobile | 7.1 (26) | 0.0 (0) | 4.5 (6) | 8.7 (4) | 0.0 (0) | |
| Dependent Variables | Factors/Covariates with Relevant Relationships | Multivariate Tests (Global Relationship with Dependent Variables) |
|---|---|---|
| Visual Discomfort MSDs | FACTORS | |
| ICT Usage Pattern | F = 37.78 (p < 0.001) | |
| TM1. Adequate ICT devices adapted to task requirements | F = 5.56 (p < 0.001) | |
| TM4. Accessory elements that improve posture | F = 3.63 (p < 0.001) | |
| TRM1. General hazard prevention training | F = 2.65 (p = 0.003) | |
| TRM3. Specific ICT hazard prevention training | F = 2.09 (p = 0.031) | |
| TRM3. Specific ICT hazard prevention training | F = 1.43 (p = 0.039) | |
| COVARIATES | ||
| Age | F = 6.46 (p < 0.001) | |
| Ratio of pauses per hour | F = 2.05 (p = 0.026) | |
| Intense exercise out of work | F = 2.40 (p = 0.008) |
| Preventive Measures | Visual Discomfort | MSDs Fingers | MSDs Wrists | MSDs Elbows | MSDs Legs | |
|---|---|---|---|---|---|---|
| Mean | Mean | Mean | Mean | Mean | ||
| TM1. Appropriate devices or equipment for the task being performed | No | 3.96 | 2.70 | 3.18 | 2.38 | 3.39 |
| Yes | 3.36 | 2.09 | 2.38 | 2.05 | 2.69 | |
| F (B-F) | 20.8 | 23.26 | 33.79 | 8.42 | 21.97 | |
| p < 0.001 | p < 0.001 | p < 0.001 | p = 0.004 | p < 0.001 | ||
| TM4. Lecterns, footrests, or other elements contributing to improve posture in front of the computer | No | 3.50 | 2.39 | 2.63 | 2.20 | 2.92 |
| Yes | 3.76 | 2.26 | 2.82 | 2.17 | 3.04 | |
| F (B-F) | 3.78 | 1.08 | 2.20 | 0.045 | 0.651 | |
| p = 0.052 | p = 0.297 | p = 0.138 | p = 0.831 | p = 0.420 | ||
| TRM1. General Training | No | 4.20 | 2.68 | 3.03 | 2.56 | 3.12 |
| Yes | 3.48 | 2.27 | 2.63 | 2.11 | 2.94 | |
| F(B-F) | 17.77 | 5.31 | 4.22 | 7.22 | 0.84 | |
| p < 0.001 | p = 0.022 | p = 0.041 | p = 0.008 | p = 0.362 | ||
| TRM3. Training related to the use of other devices | No | 3.65 | 2.37 | 2.74 | 2.19 | 3.04 |
| Yes | 3.32 | 2.15 | 2.44 | 2.16 | 2.55 | |
| F(B-F) | 3.82 | 2.08 | 2.96 | 0.033 | 7.31 | |
| p = 0.052 | p = 0.150 | p = 0.086 | p = 0.855 | p = 0.007 | ||
| Preventive Measures | MSDs Shoulders | MSDs Neck | MSDs Head | MSDs Upper Back | MSDs Lower Back | |
|---|---|---|---|---|---|---|
| Mean | Mean | Mean | Mean | Mean | ||
| P 8.1.1 Devices or equipment appropriate for the task being performed | No | 4.53 | 5.86 | 4.69 | 5.48 | 4.91 |
| Yes | 3.67 | 4.91 | 3.88 | 4.77 | 4.01 | |
| F(B-F) | 26.26 | 32.14 | 24.63 | 16.12 | 28.55 | |
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | ||
| P 8.1.4 Lecterns. footrests or other elements contributing to improve posture in front of the computer | No | 3.92 | 5.17 | 4.20 | 4.88 | 4.42 |
| Yes | 4.20 | 5.51 | 4.22 | 5.31 | 4.30 | |
| F(B-F) | 2.76 | 3.79 | 0.012 | 5.90 | 0.466 | |
| p = 0.097 | p = 0.052 | p = 0.914 | p = 0.015 | p = 0.420 | ||
| P8.3.1 General Training | No | 4.52 | 6.04 | 4.95 | 5.49 | 4.91 |
| Yes | 3.91 | 5.14 | 4.05 | 4.96 | 4.27 | |
| F(B-F) | 7.09 | 15.93 | 16.28 | 4.90 | 8.31 | |
| p = 0.008 | p < 0.001 | p < 0.001 | p = 0.028 | p = 0.004 | ||
| P 8.3.3 Training related to the use of other devices | No | 4.06 | 5.35 | 4.30 | 5.14 | 4.47 |
| Yes | 3.71 | 4.90 | 3.60 | 4.51 | 3.80 | |
| F(B-F) | 2.46 | 4.00 | 11.09 | 7.30 | 9.10 | |
| p = 0.118 | p = 0.046 | p = 0.001 | p = 0.007 | p = 0.003 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soria-Oliver, M.; López, J.S.; Torrano, F.; García-González, G.; Lara, Á. New Patterns of Information and Communication Technologies Usage at Work and Their Relationships with Visual Discomfort and Musculoskeletal Diseases: Results of a Cross-Sectional Study of Spanish Organizations. Int. J. Environ. Res. Public Health 2019, 16, 3166. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173166
Soria-Oliver M, López JS, Torrano F, García-González G, Lara Á. New Patterns of Information and Communication Technologies Usage at Work and Their Relationships with Visual Discomfort and Musculoskeletal Diseases: Results of a Cross-Sectional Study of Spanish Organizations. International Journal of Environmental Research and Public Health. 2019; 16(17):3166. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173166
Chicago/Turabian StyleSoria-Oliver, María, Jorge S. López, Fermín Torrano, Guillermo García-González, and Ángel Lara. 2019. "New Patterns of Information and Communication Technologies Usage at Work and Their Relationships with Visual Discomfort and Musculoskeletal Diseases: Results of a Cross-Sectional Study of Spanish Organizations" International Journal of Environmental Research and Public Health 16, no. 17: 3166. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173166