The Relationship between Functional Health Literacy, Self-Rated Health, and Social Support between Younger and Older Adults in Ghana


Abstract
:1. Introduction
Social Support, Health Literacy, and Age
2. Methods
2.1. Study Design and Data Collection
2.2. Measures
2.2.1. Outcome Variable: Self-Rated Health Status
2.2.2. Independent Variable: FHL
2.2.3. Moderator: Social Support
2.2.4. Covariates
2.3. Analytical Strategy
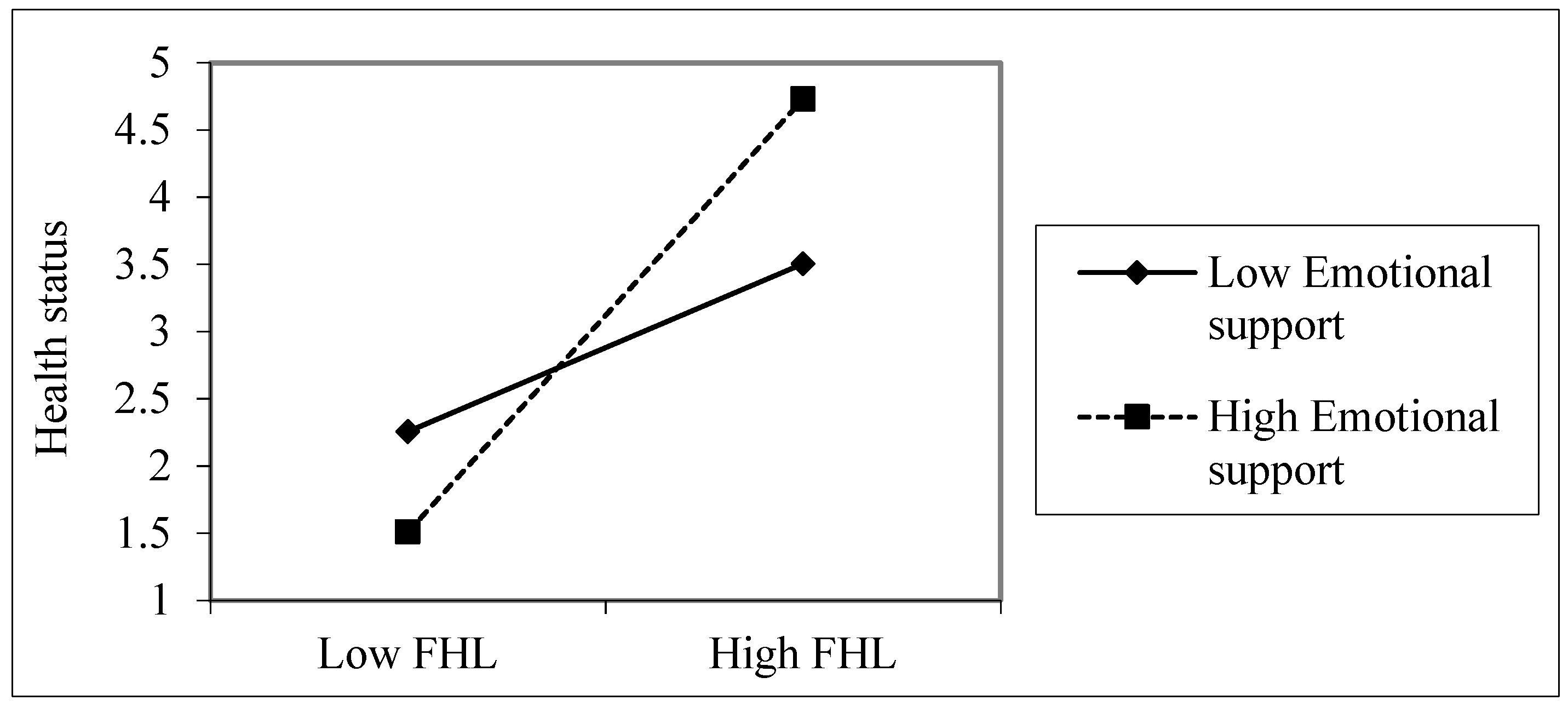
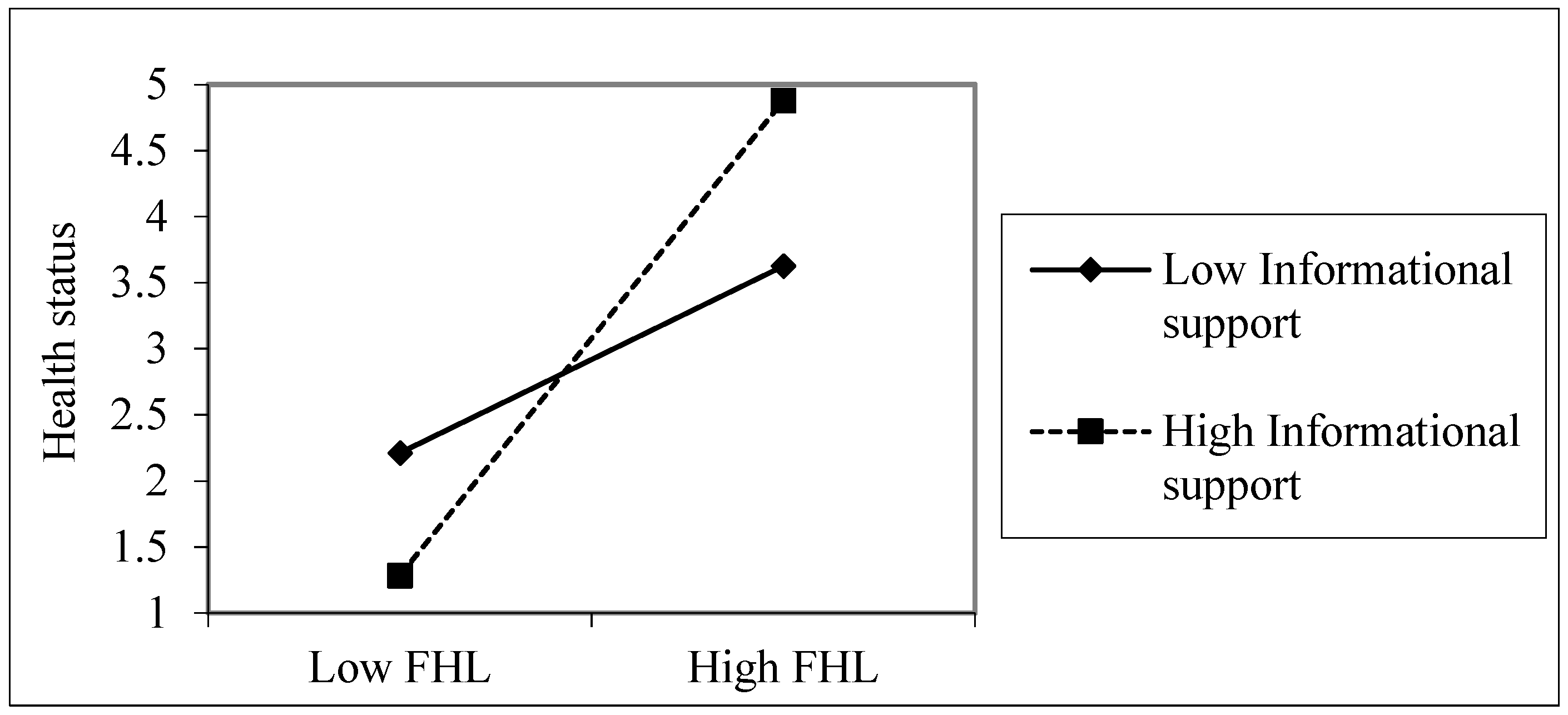
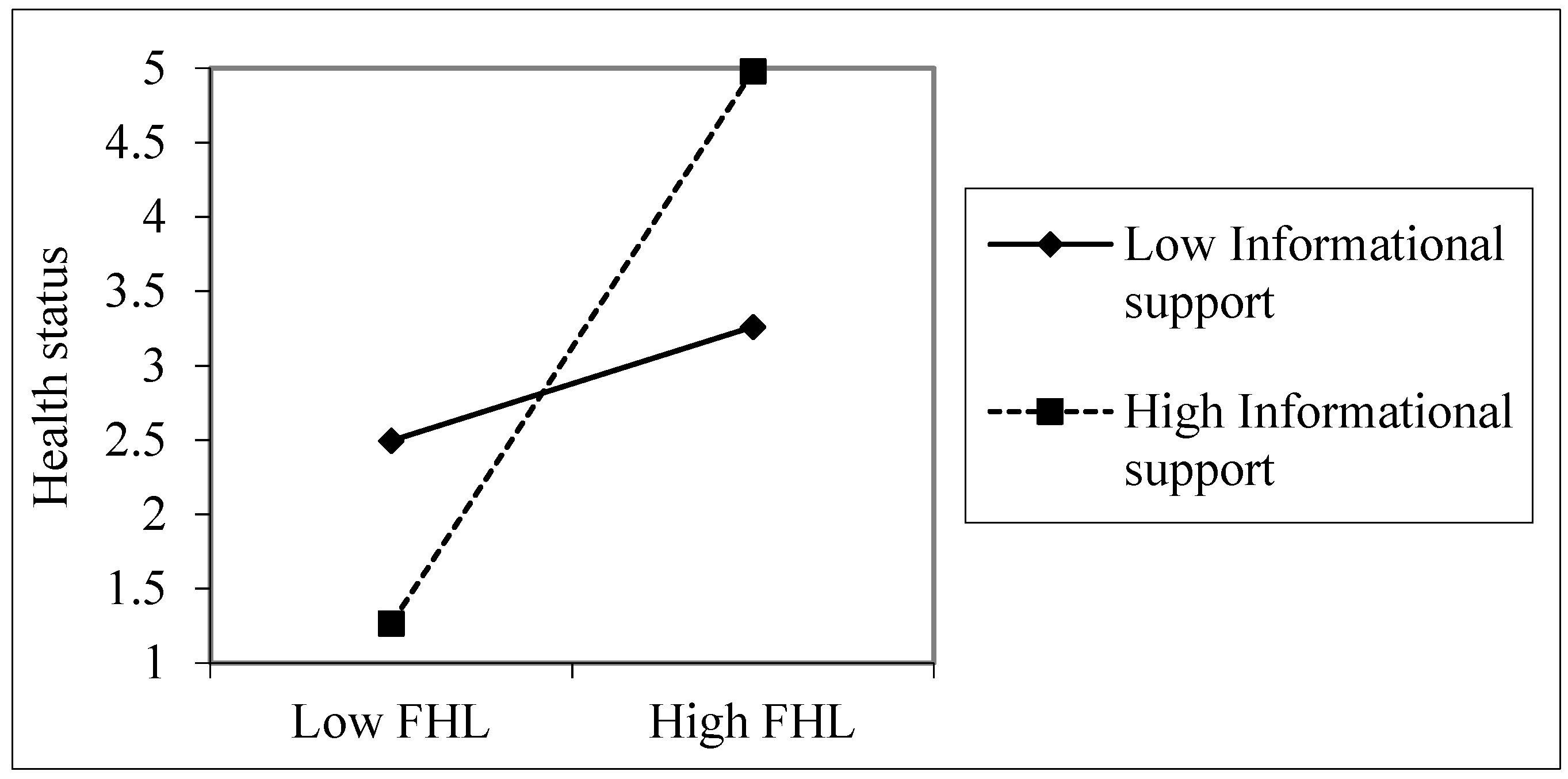
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Conflicts of Interest
References
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef] [PubMed]
- Paasche-Orlow, M.K.; Wolf, M.S. The causal pathways linking health literacy to health outcomes. Am. J. Health Behav. 2007, 31, S19–S26. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low Health Literacy and Health Outcomes: An Updated Systematic Review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Amoah, P.A.; Phillips, D.R. Health literacy and health: Rethinking the strategies for universal health coverage in Ghana. Public Health 2018, 159, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Weld, K.K.; Padden, D.; Ramsey, G.; Garmon Bibb, S.C. A framework for guiding health literacy research in populations with universal access to healthcare. ANS Adv. Nurs. Sci. 2008, 31, 308–318. [Google Scholar] [CrossRef]
- Baker, D.W.; Wolf, M.S.; Feinglass, J.; Thompson, J.A. Health Literacy, Cognitive Abilities, and Mortality Among Elderly Persons. J. Gen. Intern. Med. 2008, 23, 723–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amoah, P.A.; Phillips, D.R.; Gyasi, R.M.; Koduah, A.O.; Edusei, J. Health literacy and self-perceived health status among street youth in Kumasi, Ghana. Cogent Med. 2017, 4, 1275091. [Google Scholar] [CrossRef]
- Amoah, P.A.; Koduah, A.O.; Gyasi, R.; Gwenzi, G.; Anaduaka, S.U. The relationship between functional health literacy, health-related behaviors and sociodemographic characteristics of street-involved youth in Ghana. Int. J. Health Promot. Educ. 2019, 57, 116–132. [Google Scholar] [CrossRef]
- Nielsen-Bohlman, L.; Panzer, A.M.; Kindig, D.A. Health Literacy: A Prescription to End Confusion; Institute of Medicine of The National Academies: Washington, DC, USA, 2004. [Google Scholar]
- Berkman, L.F.; Kawachi, I.; Glymour, M.M. Social Epidemiology, 2nd ed.; Oxford University Press: Oxford, UK, 2014. [Google Scholar]
- Lockwood, N.M.; Lypen, K.; Shalabi, F.; Kumar, M.; Ngugi, E.; Harper, G.W. ‘Know that You are not Alone.’ Influences of Social Support on Youth Newly Diagnosed with HIV in Kibera, Kenya: A Qualitative Study Informing Intervention Development. Int. J. Environ. Res. Public Health 2019, 16, 775. [Google Scholar] [CrossRef]
- Gyasi, R.M.; Phillips, D.R.; Amoah, P.A. Multidimensional Social Support and Health Services Utilization Among Noninstitutionalized Older Persons in Ghana. J. Aging Health 2018. [Google Scholar] [CrossRef]
- Amoah, P.A.; Koduah, A.O.; Gyasi, R.M. “Who’ll do all these if I’m not around?”: Bonding Social Capital and Health and Well-being of Inpatients. Int. J. Qual. Stud. Health Well-Being 2018, 13, 1435108. [Google Scholar] [CrossRef]
- Gazmararian, J.; Baker, D.; Parker, R.; Blazer, D.G. A multivariate analysis of factors associated with depression: Evaluating the role of health literacy as a potential contributor. Arch. Intern. Med. 2000, 160, 3307–3314. [Google Scholar] [CrossRef] [PubMed]
- Stewart, D.W.; Reitzel, L.R.; Correa-Fernández, V.; Cano, M.Á.; Adams, C.E.; Cao, Y.; Li, Y.; Waters, A.J.; Wetter, D.W.; Vidrine, J.I. Social support mediates the association of health literacy and depression among racially/ethnically diverse smokers with low socioeconomic status. J. Behav. Med. 2014, 37, 1169–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, S.; Diederichs, C.D.; Dollmann, S.D.; Neuhauser, H.N. Health literacy, general health and social support. Results from the survey ‘German Health Update’: Susanne Jordan. Eur. J. Public Health 2017, 27 (Suppl. 3), ckx187.106. [Google Scholar] [CrossRef]
- Bruhn, J. The Group Effect: Social Cohesion and Health Outcomes; Springer: New York, NY, USA, 2009. [Google Scholar]
- Thoits, P.A. Stress, Coping, and Social Support Processes: Where Are We? What Next? J. Health Soc. Behav. 1995, 35, 53–79. [Google Scholar] [CrossRef]
- Harpham, T. The measurement of community social capital through surveys. In Social Capital and Health; Kawachi, I., Subramanian, S.V., Kim, D., Eds.; Springer: New York, NY, USA, 2008; pp. 51–62. [Google Scholar]
- Kawachi, I.; Berkman, L.F. Social ties and mental health. J. Urban Health 2001, 78, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Sisson, K.L. Theoretical explanations for social inequalities in oral health. Community Dent. Oral Epidemiol. 2007, 35, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, I.; Subramanian, S.V.; Kim, D. Social Capital and Health: A decade of progress and Beyond. In Social Capital and Health; Kawachi, I., Subramanian, S.V., Kim, D., Eds.; Springer Science: New York, NY, USA, 2008. [Google Scholar]
- Thoits, P.A. Mechanisms Linking Social Ties and Support to Physical and Mental Health. J. Health Soc. Behav. 2011, 52, 145–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuen, E.Y.N.; Knight, T.; Ricciardelli, L.A.; Burney, S. Health literacy of caregivers of adult care recipients: A systematic scoping review. Health Soc. Care Community 2016, 26, 191–206. [Google Scholar] [CrossRef]
- Peker, A.; Karaöz, S. The Effects of Social Support and Hope in the Healing of Diabetic Foot Ulcers Treated with Standard Care. Popul. Health Manag. 2017, 20, 507. [Google Scholar] [CrossRef]
- Furlong, A. Youth Studies: An Introduction; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Kafetsios, K.; Sideridis, G.D. Attachment, social support and well-being in young and older adults. J. Health Psychol. 2006, 11, 863–875. [Google Scholar] [CrossRef] [PubMed]
- Knoll, N.; Schwarzer, R. Gender and Age Differences in Social Support: A Study of East German Migrants. In Heart Disease: Environment, Stress and Gender; Weidner, G., Kopp, M.S., Kristenson, M., Eds.; IOS Press: Amsterdam, The Netherlands, 2002; pp. 198–210. [Google Scholar]
- Hsieh, C.-M.; Tsai, B.-K. Effects of Social Support on the Stress-Health Relationship: Gender Comparison among Military Personnel. Int. J. Environ. Res. Public Health 2019, 16, 1317. [Google Scholar] [CrossRef] [PubMed]
- Amoah, P.A.; Jørgensen, S.H. Social Capital, Health and Health Care among Street Children: A Case Study of Street Children in Kumasi Metropolitan Area, Ghana. Dev. Ctry. Stud. 2014, 4, 119–132. [Google Scholar]
- Amoah, P.A.; Phillips, D.R. Strengthening the Referral System through Social Capital: A Qualitative Inquiry in Ghana. Healthcare 2017, 5, 80. [Google Scholar] [CrossRef] [PubMed]
- Apt, N. Older People in Rural Ghana: Health and Health Seeking Behaviours. In Aging and Health in Africa; Maharaj, P., Ed.; Springer: Boston, MA, USA, 2013; pp. 103–119. [Google Scholar]
- Amoah, P.A.; Edusei, J.; Amuzu, D. Social Networks and Health: Understanding the Nuances of Healthcare Access between Urban and Rural Populations. Int. J. Environ. Res. Public Health 2018, 15, 973. [Google Scholar] [CrossRef] [PubMed]
- Aboderin, I. Decline in Material Family Support for Older People in Urban Ghana, Africa: Understanding Processes and Causes of Change. J. Gerontol. Ser. B 2004, 59, S128–S137. [Google Scholar] [CrossRef] [Green Version]
- Amoah, P.A. Social participation, health literacy, and health and well-being: A cross-sectional study in Ghana. SSM-Popul. Health 2018, 4, 263–270. [Google Scholar] [CrossRef]
- Lori, J.R.; Dahlem, C.H.Y.; Ackah, J.V.; Adanu, R.M.K. Examining Antenatal Health Literacy in Ghana. J. Nurs. Scholarsh. 2014, 46, 432–440. [Google Scholar] [CrossRef]
- Amoah, P.A.; Phillips, D.R. Socio-Demographic and Behavioral Correlates of Health Literacy: A Gender Perspective in Ghana. Women Health 2019, 59, 1–17. [Google Scholar] [CrossRef]
- Kobayashi, L.C.; Wardle, J.; Wolf, M.S.; von Wagner, C. Cognitive Function and Health Literacy Decline in a Cohort of Aging English Adults. J. Gen. Intern. Med. 2015, 30, 958–964. [Google Scholar] [CrossRef] [Green Version]
- Simon, M.A.; Li, Y.; Dong, X. Levels of health literacy in a community-dwelling population of Chinese older adults. J. Gerontol.—Ser. A Biol. Sci. Med. Sci. 2014, 69, S54–S60. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.C.; Lim, J.Y.; Park, K. Effects of Health Literacy and Social Capital on Health Information Behavior. J. Health Commun. 2015, 20, 1084–1094. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-Y.D.; Arozullah, A.M.; Cho, Y.I.; Crittenden, K.; Vicencio, D. Health Literacy, Social Support, and Health Status Among Older Adults. Educ. Gerontol. 2009, 35, 191–201. [Google Scholar] [CrossRef]
- Mayberry, L.S.; Rothman, R.L.; Osborn, C.Y. Family members’ obstructive behaviors appear to be more harmful among adults with type 2 diabetes and limited health literacy. J. Health Commun. 2014, 19 (Suppl. 2), 132–143. [Google Scholar] [CrossRef] [PubMed]
- Brabers, A.E.M.; de Jong, J.D.; Groenewegen, P.P.; van Dijk, L. Social support plays a role in the attitude that people have towards taking an active role in medical decision-making. BMC Health Serv. Res. 2016, 16, 502. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-Y.D.; Gazmararian, J.A.; Arozullah, A.M. Health Literacy and Social Support Among Elderly Medicare Enrollees in a Managed Care Plan. J. Appl. Gerontol. 2006, 25, 324–337. [Google Scholar] [CrossRef]
- Hagell, A. Promoting young people’s health literacy and understanding their help-seeking behaviour. In AYPH Exploring Evidence Series; Association for Young People’s Health: London, UK, 2015. [Google Scholar]
- Ruggiano, N.; Whiteman, K.; Shtompel, N. “If I Don’t Like the Way I Feel With a Certain Drug, I’ll Tell Them.”:Older Adults’ Experiences with Self-Determination and Health Self-Advocacy. J. Appl. Gerontol. 2016, 35, 401–420. [Google Scholar] [CrossRef]
- Wahl, H.-W.; Iwarsson, S.; Oswald, F. Aging Well and the Environment: Toward an Integrative Model and Research Agenda for the Future. Gerontologist 2012, 52, 306–316. [Google Scholar] [CrossRef]
- Lawton, M.P.; Nahemow, L. Ecology and the aging process. In The Psychology of Adult Development and Aging; American Psychological Association: Washington, DC, USA, 1973; pp. 619–674. [Google Scholar]
- Amoah, P.A. Social Capital, Health Literacy and Access to Healthcare: A Study among Rural and Urban Populations in Ghana; Department of Sociology and Social Policy, Lingnan University: Hong Kong, China, 2017. [Google Scholar]
- Arnett, J.J.; Žukauskienė, R.; Sugimura, K. The new life stage of emerging adulthood at ages 18–29 years: Implications for mental health. Lancet Psychiatry 2014, 1, 569–576. [Google Scholar] [CrossRef]
- GSS. 2010 Population and Housing Census: Summary Report of Final Results; Ghana Statistical Service (GSS): Accra, Ghana, 2012. [Google Scholar]
- Albert, S.M.; Freedman, V.A. Public Health and Aging: Maximizing Function and Well-Being, 2nd ed.; Springer Publishing Company: New York, NY, USA, 2009. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics; Harper Collins: New York, NY, USA, 1996. [Google Scholar]
- Bryman, A. Social Research Methods, 4th ed.; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Wångdahl, J.M.; Mårtensson, L.I. Measuring health literacy—The Swedish Functional Health Literacy scale. Scand. J. Caring Sci. 2015, 29, 165–172. [Google Scholar] [CrossRef]
- Wangdahl, J.; Lytsy, P.; Martensson, L.; Westerling, R. Health literacy among refugees in Sweden—A cross-sectional study. BMC Public Health 2014, 14, 1030. [Google Scholar] [CrossRef] [PubMed]
- Harpham, T.; Grant, E.; Thomas, E. Measuring social capital within health surveys: Keys issues. Health Policy Plan. 2002, 17, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.F. Moderation in Management Research: What, Why, When, and How. J. Bus. Psychol. 2014, 29, 1–19. [Google Scholar] [CrossRef]
- GSS. Ghana Living Standards Survey Round 6 (GLSS 6): Poverty Profile in Ghana (2005–2013); Ghana Statistical Service (GSS): Accra, Ghana, 2014. [Google Scholar]
- Parikh, N.S.; Parker, R.M.; Nurss, J.R.; Baker, D.W.; Williams, M.V. Shame and health literacy: The unspoken connection. Patient Educ. Couns. 1996, 27, 33–39. [Google Scholar] [CrossRef]
- Musich, S.; Wang, S.S.; Kraemer, S.; Hawkins, K.; Wicker, E. Purpose in Life and Positive Health Outcomes Among Older Adults. Popul. Health Manag. 2018, 21, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Fry-Bowers, E.K.; Maliski, S.; Lewis, M.A.; Macabasco-O’Connell, A.; DiMatteo, R. The Association of Health Literacy, Social Support, Self-Efficacy and Interpersonal Interactions with Health Care Providers in Low-Income Latina Mothers. J. Pediatr. Nurs. Nurs. Care Child. Fam. 2014, 29, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.; Wood, F.; Davies, M.; Edwards, A. ‘Distributed health literacy’: Longitudinal qualitative analysis of the roles of health literacy mediators and social networks of people living with a long-term health condition. Health Expect. 2013, 18, 1180–1193. [Google Scholar] [CrossRef] [PubMed]
- Vittinghoff, E.; McCulloch, C.E. Relaxing the Rule of Ten Events per Variable in Logistic and Cox Regression. Am. J. Epidemiol. 2006, 165, 710–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Analysis; Allyn and Bacon: Boston, MA, USA, 2001. [Google Scholar]
- Gelman, A.; Carlin, J. Beyond Power Calculations: Assessing Type S (Sign) and Type M (Magnitude) Errors. Perspect. Psychol. Sci. 2014, 9, 641–651. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Young and Emerging Adults 18–29 years, N = 318 | Older Adults 50+ years, N = 203 | Overall (N = 521) | ||
|---|---|---|---|---|
| % | % | p-value a | N (%) | |
| Sex | 0.266 | |||
| Male | 44.3 | 49.3 | 46.3 | |
| Female | 55.7 | 50.7 | 53.7 | |
| Context/People | 0.993 | |||
| Rural | 38.9 | 39.0 | 45.3 | |
| Urban | 61.1 | 61.0 | 54.7 | |
| Educational Attainment | 0.001 | |||
| Never been to school | 0.6 | 50.2 | 20.0 | |
| Basic education (Junior high school) | 48.8 | 31.0 | 41.3 | |
| Senior High School (SHS) | 44.0 | 12.3 | 32.1 | |
| Tertiary Level | 7.5 | 5.4 | 6.7 | |
| Marital Status | 0.001 | |||
| Married | 20.1 | 51.2 | 48.8 | |
| Unmarried | 79.9 | 48.8 | 51.2 | |
| Employment Status | 0.884 | |||
| Employed | 51.9 | 51.2 | 51.6 | |
| Unemployed | 48.1 | 48.8 | 48.4 | |
| Monthly Income/Stipend b | 0.001 c | |||
| <200 GH¢ | 52.2 | 64.9 | 58.5 | |
| 200–500 GH¢ | 26.7 | 14.9 | 20.9 | |
| 500–1000 GH¢ | 16.1 | 13.2 | 14.7 | |
| 1000+ GH¢ | 5 | 6.9 | 5.9 | |
| Informational support | 0.416 | |||
| No | 25.5 | 28.6 | 26.7 | |
| Yes | 74.5 | 71.4 | 73.3 | |
| Instrumental support | 0.573 | |||
| No | 24.5 | 26.7 | 25.3 | |
| Yes | 75.5 | 73.3 | 74.7 | |
| Emotional support | 0.033 | |||
| No | 22.3 | 30.7 | 25.6 | |
| Yes | 77.7 | 69.3 | 74.4 | |
| Health literacy | 0.001 | |||
| Sufficient HL | 43.1 | 28.1 | 37.2 | |
| Problematic HL | 35.5 | 21.7 | 30.1 | |
| Inadequate HL | 21.4 | 50.2 | 32.6 | |
| Mean (SD)/ Minimum-maximum d | 19.2 (3.8)/5–25 | 15.6 (5.1)/5–25 | 17.8 (4.9)/ 5–25 | |
| Health status | 0.001 c | |||
| Poor | 10.1 | 15.3 | 12.1 | |
| Fair | 15.1 | 22.2 | 17.9 | |
| Good | 26.7 | 31.5 | 28.6 | |
| Very good | 32.7 | 25.1 | 29.8 | |
| Excellent | 15.4 | 5.9 | 11.7 |
| Young and Emerging Adults (18–29 years) | Older-Persons (50 years +) | Overall | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Estimate (B) | Std. Error | 95% Confidence Interval | Estimate (B) | Std. Error | 95% Confidence Interval (B) | Estimate | Std. Error | 95% Confidence Interval (B) | ||||
| Lower Bound | Upper Bound | Lower Bound | Upper Bound | Lower Bound | Upper Bound | |||||||
| Age | −0.530 | 0.521 | −1.551 | 0.490 | −0.097 | 0.141 | −0.373 | 0.180 | −0.270 * | 0.116 | −0.498 | −0.043 |
| Income/stipend | 0.144 | 0.212 | −0.271 | 0.559 | 0.258 * | 0.125 | 0.013 | 0.504 | 0.223 * | 0.098 | 0.031 | 0.414 |
| Marital status | ||||||||||||
| Not married (ref) | ||||||||||||
| Married | 0.664 ** | 0.282 | 0.111 | 1.217 | 0.177 | 1.003 | −2.143 | 1.788 | 0.504 * | 0.235 | 0.044 | 0.964 |
| Information support | ||||||||||||
| No (ref) | ||||||||||||
| Yes | 0.247 * | 0.102 | 0.008 | 0.485 | 0.184 * | 0.061 | 0.019 | 0.421 | 0.278 ** | 0.097 | 0.087 | 0.467 |
| Instrumental support | ||||||||||||
| No (ref) | ||||||||||||
| Yes | −0.169 | 0.123 | −0.410 | 0.071 | 0.114 | 0.196 | −0.260 | 0.488 | −0.063 | 0.097 | −0.254 | 0.127 |
| Emotional support | ||||||||||||
| No (ref) | ||||||||||||
| Yes | 0.286 ** | 0.106 | 0.058 | 0.513 | 0.150 | 0.194 | −0.231 | 0.531 | 0.166 * | 0.043 | 0.026 | 0.349 |
| Health literacy | 0.294 ** | 0.099 | 0.081 | 0.478 | 0.261 * | 0.163 | 0.059 | 0.580 | 0.190 * | 0.050 | 0.035 | 0.376 |
| Health literacy * Instrumental support | −0.005 | 0.127 | −0.255 | 0.244 | 0.077 | 0.171 | −0.257 | 0.412 | −0.040 | 0.096 | −0.228 | 0.148 |
| Health literacy*Informational support | 0.193 | 0.132 | −0.451 | 0.065 | 0.238 * | 0.053 | 0.072 | 0.531 | 0.284 ** | 0.089 | 0.109 | 0.459 |
| Health literacy*Emotional support | 0.309 ** | 0.121 | 0.071 | 0.547 | 0.151 | 0.143 | −0.129 | 0.431 | 0.117 | 0.091 | −0.062 | 0.296 |
| Cox and Snell | 0.086 | 0.117 | 0.175 | |||||||||
| Nagelkerke | 0.091 | 0.123 | 0.178 | |||||||||
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amoah, P.A. The Relationship between Functional Health Literacy, Self-Rated Health, and Social Support between Younger and Older Adults in Ghana. Int. J. Environ. Res. Public Health 2019, 16, 3188. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173188
Amoah PA. The Relationship between Functional Health Literacy, Self-Rated Health, and Social Support between Younger and Older Adults in Ghana. International Journal of Environmental Research and Public Health. 2019; 16(17):3188. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173188
Chicago/Turabian StyleAmoah, Padmore Adusei. 2019. "The Relationship between Functional Health Literacy, Self-Rated Health, and Social Support between Younger and Older Adults in Ghana" International Journal of Environmental Research and Public Health 16, no. 17: 3188. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173188