Being at the Bottom Rung of the Ladder in an Unequal Society: A Qualitative Analysis of Stories of People without a Home


Abstract
:1. Introduction
2. Study Methods
2.1. Setting, Recruitment, and Sampling Strategies
2.2. Data Collection
2.3. Ethical Approval
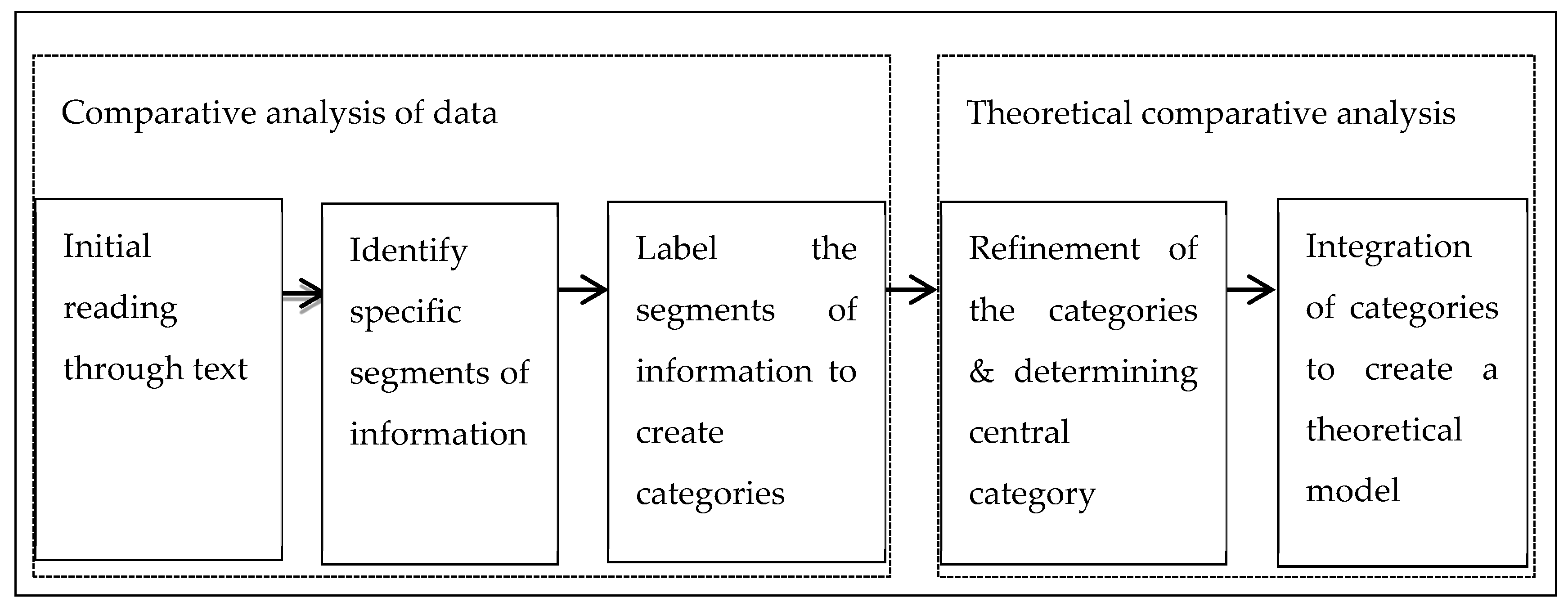
3. Data Analysis
4. Results:
4.1. Being Homeless is Being at the Bottom Rung of the Ladder
I am sick of being looked down upon by the members of the public; I am sick of being discriminated and being hurt because I am homeless on the street. …you get assaulted left, right and centre by the members of the public and at the same time police are giving us all the ASBOs[anti-social behaviour order] kicking us out of town, shift you off to another town, what is the point of that? You will still be homeless.[Kelly]
It is horrible being in the street you … you get battered every so often. … people come up to me on the street kick punch me, which is what they do all the time because I am a homeless person in the street.
I am a big girl … sometimes they think I am a man, but I do not think that matters anyway, they have known I am a girl, but they still battered me.[Kelly]
I used to be battered by people in their night out in the town centre where I grew up, people used to batter me, I don’t think they understood I was that I was the only child, yea I used to be battered by drunk people Friday and Saturday night.[Thomas]
…after I got kicked out … I was living and sleeping on the streets, …going to work then going on the streets again… I tried to find any shelter I could go under where it isn’t wet, where it is out of the way somewhere where no one would disturb me… I was quite scared I suppose ’cause I didn’t know where to go or what was gonna happen with my job ’cause I was living on the streets.[Clarke]
I’ve been trying to bid on properties… they wanted non-smokers or people over 21, stuff like that… [be]cause I’m 17, on a zero-hour contract they were like what if you don’t have the money to pay rent or…[Clarke]
You just seem to lose all self-respect and reassurance that you have when you’ve got a roof over your head that you can go back to, um frightening very frightening I … It is really horrible not being able to do anything in the privacy of your own home like you know. Frightening very frightening, constant fear of being robbed, bullied and turning to drink, or drugs.[Danny]
When I got that injury and had to go to the hospital, um somebody had burnt me tent down with all my belongings in it, whilst I was at the hospital. So, I lost everything.[Gary]
We came to Chester because Chester has facilities like this that accommodate homeless people. But because of no local connection, there’s not a lot of people can do. So we put up a tent near the canal until this Saturday when people decided to trash it.[Marie and Thomas]
My stuff gets robbed off me all the time, my medication gets robbed. Last week all my medication and all that got robbed. Cause the diazes and zoppies and that people get off on them, gets them wrecked.
If I’ve got 14 Ensures in a bag, walking around with them all the time and a big bag full of medication I’m asking to get robbed, in the town I’m asking to get robbed. You can’t even leave your *dibs* on the floor sometimes and someone robs them off ya. You know Ensures in the shop they are £4.50 a bottle so people are gonna steal them off me cause they could get £1 each for them on the streets. But I can’t have people doing that all the time.[Henry]
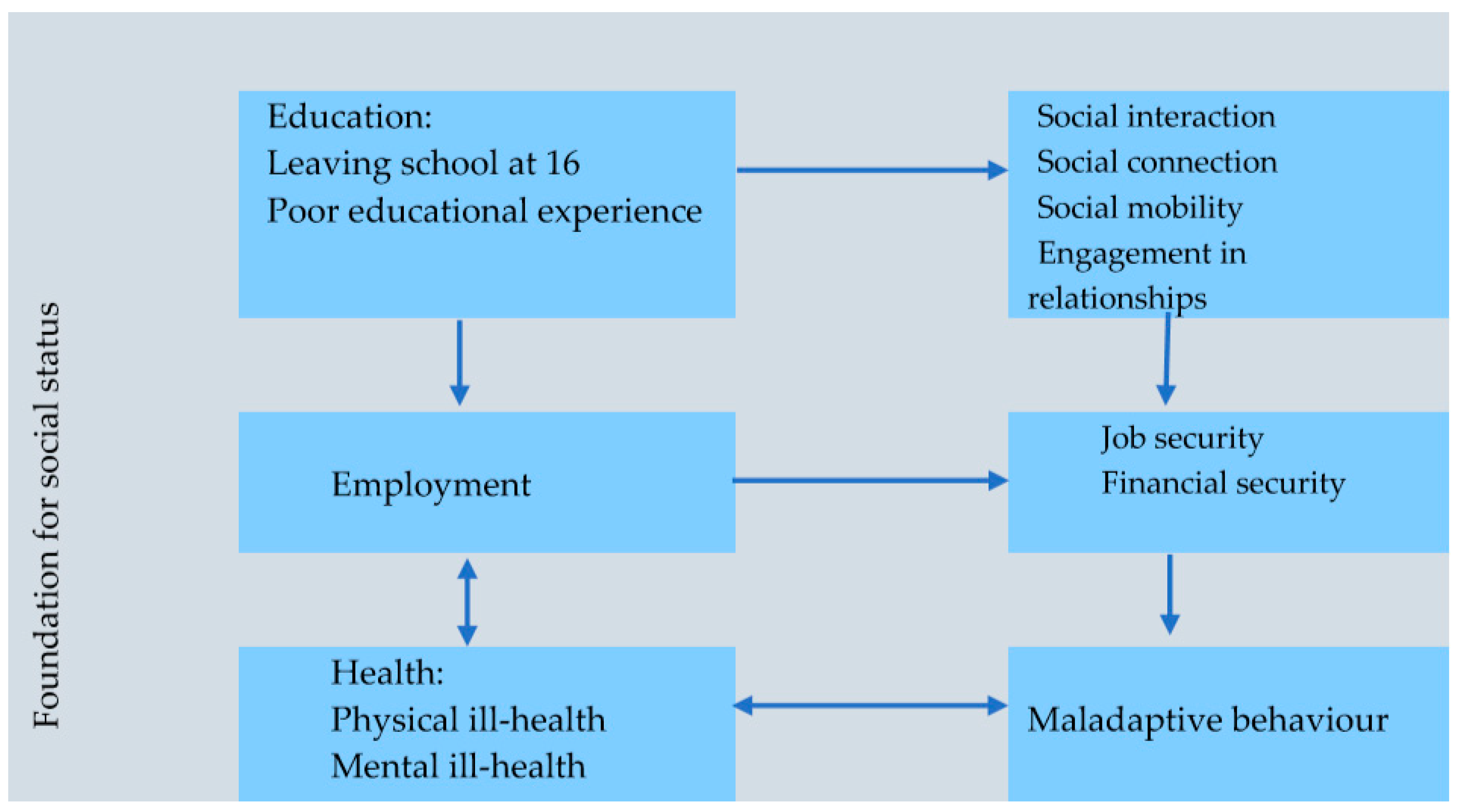
4.2. Social Status of Homeless People
4.2.1. Education
… at the end of the day, if you don’t have education early enough in life, I don’t mean maths, English and that, I mean being able to actually engage with people. If you don’t have that education early on enough in life, I’m talking about the age of 5, 6, 7, 8, if you don’t have that then we get a despondent youth and once it goes down, they’re on a very slippery slope. And it’s very tough to get yourself back up, you know. You are on a ladder without rungs if you know what I mean.[Barry]
I did not go to school because I kept on bunking. When I was fifteen I left school because I was caught robbing, the police took me home and my mum told me you’re not going back to school again, you are now off for good. Because if you go back to school you keep on thieving, she said I keep away from the lads. I said fair enough. When I was seventeen I got run over by a car.[Pat]
- Leaving school at the age of 16
- Poor educational experiences.
I left school when I was fifteen because I was the youngest in my year. I left school then I went off the rails. I got kidnapped for three and a half months. When I came back I was just more interested in crime. When I left school I was supposed to go to College, but I went with travellers. I was just more interested in getting arrested every weekend until my mum say right I have enough of you. I was only seventeen. I went through the hostels when I was seventeen.[Lee]
I left school when I was sixteen straight away I got married had children, I have three children and marriage was fine. Um, I was married for 17 years. Um, and as the marriage broke up I turned to…[Danny]
… I was working on building sites before I left school at 16 you know when I was doing my exams I actually got the job and I was hod carrying for the bricklayers…[Alvin]
On a few occasions I came out on the corridors, I would be getting battered on to my hands and knees and teachers walk past me. There was quite often blood on the floor from my nose, would be punched on my face and be thrown on the floor. …. It was a hard school, pernicious. I would go as far as saying I never felt welcome in that school, I felt like a fish out of the water.
Eventually, I started striking back when I started striking back suddenly I was a bad one. My mother decided to put me in … school for maladjusted boys, everyone who been there including me has spent time in prison.[Marco]
The kids used to overhear my aunty talking to the teachers about my child abuse [she was sexually abused by her biological father], I used to go to the toilet and the boys will say are you coming out to play? The girls will be telling me we don’t want anything to do with because of your daddy something, something, something.[Kelly]
I couldn’t go to school really because I was an abandoned child…[Thomas]
You were bullied in that way, weren’t you?[Marie]
Obviously, I wasn’t diagnosed with ADHD till I was like 13, so like in school they used to say that’s just a naughty child. … So it was like always getting suspended, excluded and all that sort of stuff. And in the end [I] went to college and the same happened there.[Emily]
4.2.2. Employment
I’ve had it all; really, I’ve had a wife, I’ve got two gorgeous girls now who are 11 and 13, who’ve I got this afternoon actually. Then there was a break up of my marriage. Basically, it started off I was a bricklayer …, I was a builder and had a mortgage had the BMWs had everything… when the recession hit when Liverpool 2008 … won culture capital, it was an abundance of bricklayers so the prices went down in the bricklaying so basically with me having two young children I was the only breadwinner in the family… I had to kinda look for factory work and so I managed to get a job, … it shifted work like four 12 hour days and four 12 hour nights and 6 days off, really hard shifts
… I was off Monday, Tuesday, Wednesday, Thursday you know for instance, but I’d treat that like me weekend you know because I’ve worked all weekend. Then… so I’d have a drink then and stuff like that you know. and it’s … 7 o’clock on a Monday morning not really the time to be drinking but I used to treat it like my weekend.[Alvin]
so we argued me and my ex-missus a little bit and in the end, we split up…, I was diagnosed with depression and anxiety… so I used to drink …to get rid of the anxiety and to numb the pain of the breakup of my marriage really you know it was not good you know.[Alvin]
I had an injury to my ankle which stopped me from working. I was at home all day, every day. …I was drinking because I was bored. I started drinking a lot [be]cause I couldn’t move about in the house. It was a bad injury I had to my ankle. Um, and one day me and my partner were having this argument and I turned around and saw my little boy just stood there stiff as a board just staring, looking at us. And from that day on I just said to my a partner that I’ll move out, cause I didn’t want my little boy to be seeing this all the time.[Gary]
I used to have a bit of a drink but it wasn’t a problem because I used to get up in the morning and go out to work and enjoy a couple of beers every evening after a day’s work. Um, but then when I wasn’t working I was drinking, and it just snowballed out, you know snowball effect having four cans every evening and then it went from there. I was drinking more [be]cause I was depressed. I was very active before and then I became like non-active, not being able to do anything and in a lot of pain as well.[Gary]
Yes, yes I was roofing for about 10 years. It was a very good job. I enjoyed what I was doing you know. … [I drank] but not very heavy, just like a sociable drink after work. I’d call into like the local pub and have a few pints and it was controlled. My drinking habit was under control then.
I was drinking quite heavily then [when I lost my job and marriage broke down]. I suppose it was a form of release ….[Danny]
4.2.3. Health
4.2.4. Physical Illnesses
I got assaulted, kicked down a flight of stairs, I landed on my back on the bottom of the stairs but my heel hit the stairs as it was still going up if you know what I mean. Smashed me heel, fractured my heel… So, by the time I got to the hospital and they x-rayed it, there wasn’t even able to operate [be]cause it was in that many pieces, they weren’t even able to pin it if you know what I mean.[Gary]
It was an alcohol withdrawal seizure I had at the top of the stairs of all places. So I had a fall and I’ve crushed four of my vertebrae so I’m unable to work at the moment. I am awaiting surgery. Hopefully, that would give me a little bit of mobility back.
I’m unable to work at the moment due to my collapse spine. A collapsed spine they put me as a condition. I’ve crushed four vertebrae through a fall.[Danny]
… a foot infection when I was in the streets but that’s gone …my foot was like red, totally red on the bottom and it had all blisters on the bottom. So he [the doctor] gave me the tablets and the cream prescription. I think four tablets a day and the cream twice a day. It seemed to work I suppose. … I was in that much pain and I had to keep sitting down every like 10–15 yards ’cause I was in that much pain. I keep getting sent home from work ’cause I was in that much pain.[Clarke]
… I was quite scared I suppose ’cause I didn’t know where to go or what was gonna happen with my job ’cause I was living on the streets.[Clarke]
I’m striving towards you know …I wanna make a success of my life, I wanna rebuild and get that BMW back and get you to know.[Alvin]
4.2.5. Mental Wellbeing
… so we argued me and my ex-missus a little bit and in the end, we split up so…, the drinking got worse, I was diagnosed with depression and anxiety, now I used to drink used to drink to get rid of the anxiety and also to numb the pain of the breakup of my marriage really you know it wasn’t good you know, one thing led to another and I just couldn’t stop it got hold of me the alcohol.[Alvin]
They say… well I suffer really bad now from mental health problem and anxiety and they say like at the age of 11, to lose a parent at the age of 11 you like in between. I was drinking more cause I was depressed.[Gary]
I was drinking quite a lot as well trying to take my to mind off it and trying to make me go to sleep. ’Cause I was up all night cause I couldn’t get to sleep. But if I drank had a few drinks I could go sleep.[Clarke]
I was admitted about I don’t know 10 times—suicidal thoughts, pancreatitis which was through the drinking, just hating myself. …, did not really wanna be on this planet. The reason I used to drink the vodka is that it sooner is asleep than awake. I used to hate waking up cause I just hated what was going on. Hated what I was doing to my family but it was a catch 22 cause I drank more to block it out, you know.[Alvin]
There have been days that I feel like I just don’t want to be here anymore, I don’t want to face the world; and it’s very frightening, very frightening.[Danny]
I’m going to end up waking up and thinking of killing meself like today. It’s wrong. I shouldn’t have to feel like that. I’m 29, and all I want to do really is just die.[Henry]
I suppose, your mood’s very low when you’re homeless and you’re not able to think straight and you would possibly turn to anything you know. Drink or drugs. At the moment, like I said I’m being strong, I’m not turning back to alcohol as I’d like to think I’d never go back down that path again.
It’s my mental health that suffered a lot I was very, very depressed. Um, which I did. I have tried to take my own life a couple of times through medication and self-harm cause I couldn’t put up any longer on the streets you know.
I think if I was in now I’d probably have tried to take my life again. Not being able to handle or cope with not having the help and support.[Danny]
When you homeless you can’t think, you can’t do anything, the best thing people do is to get pissed get drunk and drugs just to get by, when they get drunk they don’t bother where they go. I don’t drink alcohol but I have used cannabis in the past.[Lee]
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Homeless Link. 2017 Rough Sleeping Statistics; Homeless Link: London, UK, 2017. [Google Scholar]
- Department of Housing Communities and Local Government (DCLG). Rough Sleeping Statistics Autumn 2017, England (Revised); Department of Housing, Communities and Local Government (DCLG): London, UK, 2018.
- Government Legislation. Homelessness reduction act 2017. In c.13; Crown: London, UK, 2017. [Google Scholar]
- Anderson, I. Synthesizing homelessness research: Trends, lessons and prospects. J. Community Appl. Soc. Psychol. 2003, 13, 197–205. [Google Scholar] [CrossRef]
- Anderson, I.; Christian, J. Causes of homelessness in the UK: A dynamic analysis. J. Community Appl. Soc. Psychol. 2003, 13, 105–118. [Google Scholar] [CrossRef]
- Mabhala, M.A.; Yohannes, A.; Griffith, M. Social conditions of becoming homelessness: Qualitative analysis of life stories of homeless peoples. Int. J. Equity Health 2017, 16, 150. [Google Scholar] [CrossRef]
- Bingham, B.; Moniruzzaman, A.; Patterson, M.; Distasio, J.; Sareen, J.; O’Neil, J.; Somers, J.M. Indigenous and non-indigenous people experiencing homelessness and mental illness in two canadian cities: A retrospective analysis and implications for culturally informed action. BMJ Open 2019, 9, e024748. [Google Scholar] [CrossRef]
- Duff, P.; Shoveller, J.; Chettiar, J.; Feng, C.; Nicoletti, R.; Shannon, K. Sex work and motherhood: Social and structural barriers to health and social services for pregnant and parenting street and off-street sex workers. Health Care Women Int. 2015, 36, 1039–1055. [Google Scholar] [CrossRef]
- Fazel, S.; Geddes, J.R.; Kushel, M. The health of homeless people in high-income countries: Descriptive epidemiology, health consequences, and clinical and policy recommendations. Lancet 2014, 384, 1529–1540. [Google Scholar] [CrossRef]
- Jones, M.M. Creating a science of homelessness during the reagan era. In The Milbank Quarterly; Wiley Periodicals Inc.: San Francisco, CA, USA, 2015; Volume 93, pp. 139–178. [Google Scholar]
- Shinn, M.; Gibbons-Benton, J.; Brown, S.R. Poverty, homelessness, and family break-up. Child Welf. 2015, 94, 105–122. [Google Scholar]
- Van Leeuwen, B. To the edge of the urban landscape: Homelessness and the politics of care. Polit Theory 2018, 46, 586–610. [Google Scholar] [CrossRef]
- Gaetz, S.; O’grady, B.; Kidd, S.; Schwan, K. Without a Home: The National Youth Homelessness Survey. Available online: https://homelesshub.ca/sites/default/files/WithoutAHome-final.pdf (accessed on 11 Novermber 2019).
- Gaetz, S. Safe streets for whom? Street youth, social exclusion and criminal victimization. Can. J. Criminol. Crim. Justice 2004, 46, 423–456. [Google Scholar] [CrossRef]
- Kidd, S.A.; Gaetz, S.; O’Grady, B. The 2015 national canadian homeless youth survey: Mental health and addiction findings. Can. J. Psychiatry 2017, 62, 493–500. [Google Scholar] [CrossRef]
- Fry, C.; Langley, K.; Shelton, K. A sysyematic review of cognitive functioning among young people who have experienced homelessness, foster care, ot poverty. Child. Neuropsychol. 2017, 23, 907–934. [Google Scholar] [CrossRef] [PubMed]
- Deforge, B.R.; Belcher, J.; O’rourke, M.; Lindsey, M.A. Personal resources and homelessness in early life: Predictors of depression in consumers of homeless multiservice centres. J. Loss Trauma 2008, 13, 222–242. [Google Scholar] [CrossRef]
- Bauermeister, J.A.; Eaton, L.; Meanley, S.; Pingel, E.S.; Partnership, U. Transactional sex with regular and casual partners among young men who have sex with men in the detroit metro area. Am. J. Men’s Health 2017, 11, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Skosireva, A.; O’Campo, P.; Zerger, S.; Chambers, C.; Gapka, S.; Stergiopoulos, V. Different faces of discrimination: Perceived discrimination among homeless adults with mental illness in healthcare settings. BMC Health Serv. Res. 2014, 14, 376. [Google Scholar] [CrossRef]
- McNeil, R.; Kerr, T.; Anderson, S.; Maher, L.; Keewatin, C.; Milloy, M.J.; Wood, E.; Small, W. Negotiating structural vulnerability following regulatory changes to a provincial methadone program in Vancouver, Canada: A qualitative study. Soc. Sci Med. 2015, 133, 168–176. [Google Scholar] [CrossRef]
- Shinn, M. Homelessness, poverty and social exclusion in the united states and europe. Eur. J. Homelessness 2010, 4, 19–43. [Google Scholar]
- Patterson, M.L.; Moniruzzaman, A.; Somers, J.M. History of foster care among homeless adults with mental illness in vancouver, british columbia: A precursor to trajectories of risk. BMC Psychiatry 2015, 15, 32. [Google Scholar] [CrossRef]
- Reeve, K. Welfare conditionality, benefit sanctions and homelessness in the UK: Ending the ‘something for nothing culture’ or punishing the poor? J. Poverty Soc. Justice 2017, 25, 65–78. [Google Scholar] [CrossRef]
- Somers, J.; Patterson, M.; Moniruzzaman, A.; Currie, L.; Rezansoff, S.; Palepu, A. Vancouver at home: Pragmatic randomized trials investigating housing first for homeless and mentally ill adults. Trials 2013, 14, 365. [Google Scholar] [CrossRef]
- Watson, J.; Crawley, J.; Kane, D. Social exclusion, health and hidden homelessness. Public Health 2016, 139, 96–102. [Google Scholar] [CrossRef]
- Roos, L.E.; Distasio, J.; Bolton, S.-L.; Katz, L.Y.; Afifi, T.O.; Isaak, C.; Goering, P.; Bruce, L.; Sareen, J. A history in-care predicts unique characteristics in a homeless population with mental illness. Child Abus. Negl. 2014, 38, 1618–1627. [Google Scholar] [CrossRef] [PubMed]
- Roos, L.E.; Mota, N.; Afifi, T.O.; Katz, L.Y.; Distasio, J.; Sareen, J. Relationship between adverse childhood experiences and homelessness and the impact of axis i and ii disorders. Am. J. Public Health 2013, 103, S275–S281. [Google Scholar] [CrossRef] [PubMed]
- Barker, B.; Kerr, T.; Dong, H.; Wood, E.; DeBeck, K. High school incompletion and childhood maltreatment among street-involved young people in vancouver, canada. Health Soc. Care Community 2017, 25, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis; Sage Publications: London, UK, 2006. [Google Scholar]
- Mabhala, M.A. Health inequalities as a foundation for embodying knowledge within public health teaching: A qualitative study. Int. J. Equity Health 2013, 12, 46. [Google Scholar] [CrossRef] [PubMed]
- Mabhala, M. Public health nurse educators’ conceptualisation of public health as a strategy to reduce health inequalities: A qualitative study. Int. J. Equity Health 2015, 14, 1–11. [Google Scholar] [CrossRef]
- Mabhala, M. The Social and Health Inequalities Agenda; McGraw Hill Open University Press: Maidenhead, UK, 2014. [Google Scholar]
- Mabhala, M.A.; Ellahi, B.; Massey, A.; Kingston, P. Understanding the determinants of homelessness through examining the life stories of homeless people and those who work with them: A qualitative research protocol. Divers. Equal. Health Care 2016, 13, 284–289. [Google Scholar] [CrossRef]
- Mabhala, M.A.; Massey, A.; Reid, J. Mind your language: Discursive practices produce unequal power and control over infectious disease: A critical discourse analysis. Int. J. Prev. Med. 2019, 13, 284–289. [Google Scholar]
- Mabhala, M. Social justice and global perspectives on health improvement. In Health in Improvement and Wellbeing Strategies and Actions; Wilson, F., Mabhala, M.A., Massey, A., Eds.; McGrow Hill: Maidenhead, UK, 2015. [Google Scholar]
- Strauss, A.; Corbin, J. Basics of Qualitative Research: Tecniques and Procedures for Developing Grounded Theory; Sage Publications: London, UK, 1998. [Google Scholar]
- Díaz Andrade, A. Interpretive research aiming at theory building: Adopting and adapting the case study design. Qual. Rep. 2009, 2, 42–60. [Google Scholar]
- Dey, I. Grounding Grounded Theory: Guidelines for Qualitative Inquiry; Academic Press: San Diego, CA, USA, 1999. [Google Scholar]
- Economic and Social Research Council. Esrc Framework for Research Ethics (fre). Available online: http://www.esrc.ac.uk/about-esrc/information/research-ethics.aspx (accessed on 19 July 2019).
- HM Government. Mental Capacity Act 2005. Available online: http://www.legislation.gov.uk/ukpga/2005/9/pdfs/ukpga_20050009_en.pdf (accessed on 5 June 2017).
- Corbin, J.; Strauss, A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory; Sage Publications: Los Angeles, CA, USA, 2008. [Google Scholar]
- Krieger, N.; Birn, A.E. A Vision of Social Justice as the Foundation of Public Health: Commemorating 150 Years of the Spirit of 1848. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC1508556/pdf/amjph00023-0009.pdf (accessed on 26 February 2009).
- Marmot, M. Achieving health equity: From root causes to fair outcomes. Lancet 2007, 6736, 1153–1163. [Google Scholar] [CrossRef]
- Powers, M.; Faden, R. Social Justice: The Foundations of Public Health and Health Policy; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Rawls, J. A Theory of Justice; Harvard University Press: Cambridge, MA, USA, 1971. [Google Scholar]
- Ruger, P.J. Health and social justice. Lancet Public Health 2004, 364, 1075–1080. [Google Scholar] [CrossRef]
- Department for Communities and Local Goverment. The English Indices of Deprivation 2015; Department for Communities and Local Goverment: London, UK, 2015.
- Keane, C.A.; Magee, C.A.; Kelly, P.J. Is there a complex trauma experience typology for australians experiencing extreme social disadvantage and low housing stability? Child Abus. Negl. 2016, 61, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Bassuk, E.L.; Buckner, J.C.; Weinreb, L.F.; Browne, A.; Bassuk, S.S.; Dawson, R.; Perloff, J.N. Homelessness in female-headed families: Childhood and adult risk and protective factors. Am. J. Public Health 1997, 87, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Tierney, W.G.; Gupton, J.T.; Hallett, R.E. Transitions to Adulthood for Homeless Adolescents: Education and Public Policy. Available online: https://files.eric.ed.gov/fulltext/ED503645.pdf (accessed on 24 April 2018).
- Tsai, J.; Edens, E.; Rosenheck, R. A typology of childhood problems among chronically homeless adults and its association with housing and clinical outcomes. J. Health Care Poor Underserved 2011, 22, 853–870. [Google Scholar] [CrossRef] [PubMed]
- Haskett, M.E.; Armstrong, M.J.; Tinsdale, J. Developmental status and social-emotional functioning of young children experiencing homelessness. Early Child. Educ. J. 2016, 44, 119–125. [Google Scholar] [CrossRef]
- Department of Education. Unlocking Talent, Fulfilling Potential a Plan for Improving Social Mobility Through Education. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/667690/Social_Mobility_Action_Plan_-_for_printing.pdf (accessed on 19 July 2019).
- Caton, C.L.M.; Dominguez, B.; Schanzer, B.; Hasin, D.S.; Shrout, P.E.; Felix, A.; McQuistion, H.; Opler, L.A.; Hsu, E. Risk factors for long-term homelessness: Findings from a longitudinal study of first-time homeless single adults. Am. J. Public Health 2005, 95, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Barile, J.P.; Pruitt, A.S.; Parker, J.L. A latent class analysis of self-identified reasons for experiencing homelessness: Opportunities for prevention. J. Community Appl. Soc. Psychol. 2018, 28, 94–107. [Google Scholar] [CrossRef]
- D’Amore, J.; Hung, O.; Chiang, W.; Goldfrank, L. The epidemiology of the homeless population and its impact on an urban emergency department. Acad. Emerg. Med. 2001, 8, 1051–1055. [Google Scholar] [CrossRef] [Green Version]
- Laporte, A.; Vandentorren, S.; Détrez, M.-A.; Douay, C.; Le Strat, Y.; Le Méner, E.; Chauvin, P.; The Samenta Research, G. Prevalence of mental disorders and addictions among homeless people in the greater paris area, france. Int. J. Environ. Res. Public Health 2018, 15, 241. [Google Scholar] [CrossRef] [Green Version]
- Santa Maria, D.; Padhye, N.; Yang, Y.; Gallardo, K.; Businelle, M. Predicting sexual behaviors among homeless young adults: Ecological momentary assessment study. JMIR Public Health Surveill 2018, 4, e39. [Google Scholar] [CrossRef]
- Smith, C.M.; Trienekens, S.C.M.; Anderson, C.; Lalor, M.K.; Brown, T.; Story, A.; Fry, H.; Hayward, A.C.; Maguire, H. Twenty years and counting: Epidemiology of an outbreak of isoniazid-resistant tuberculosis in england and wales, 1995 to 2014. Eurosurveillance 2017, 22, 30467. [Google Scholar] [CrossRef]
- Worrell, M.C.; Kramer, M.; Yamin, A.; Ray, S.M.; Goswami, N.D. Use of activity space in a tuberculosis outbreak: Bringing homeless persons into spatial analyses. Open Forum Infect. Dis. 2017, 4, 280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seedhouse, D. Health: The Foundations for Achievement; John Wiley Ltd.: London, UK, 1986. [Google Scholar]



{kind=link}
{kind=link}
| Pseudonym | Age | Education History | Childhood Living Arrangements | Employment History | Drugs, Alcohol or Tobacco? | Age of Contact with the Criminal Justice System |
|---|---|---|---|---|---|---|
| Ruddle | 35 | Left school at 16 | Both parents | Never worked | Yes | 18 |
| Ian | 74 | Both parents | Both parents | Paint and decoration | Yes | No criminal record |
| Patrick | 64 | Left school at 16 | Both parents | Never worked | Yes | 12 |
| Lee | 35 | Left school at 15 | Children’s care | Chef | Yes | 15 |
| David | 31 | Left school at 16 | Foster care | Untrained chef | Yes | No criminal record |
| Marco | 46 | Left school at 16 | Residential school for boys with challenging behaviour | Building construction | Yes | 15 |
| Alvin | 39 | Left school at 16 | Both parents | Builder | Yes | No criminal record |
| Barry | 43 | Law Degree | Both parents | Military | No | No criminal record |
| Clarke | 18 | Left school at 16 | Mum and stepdad | McDonald | Yes | No criminal record |
| Danny | 44 | Left school at 16 | Both parents | Roofer | Yes | No criminal record |
| Emily | 23 | Left school at 16 | Single mum | Morrison supermarket | Yes | 16 |
| Finn | 24 | Left school at 16 | Single parent | Takeaway restaurant | Yes | No criminal record |
| Geoff | 32 | Left school at 16 | Both parents | Warehouse | Yes | No criminal record |
| Gary (John) | 35 | Left school at 16 | Mum and stepdad | Joiner | Yes | No criminal record |
| Guy | 26 | Left school at 16 | Both parents | Factory worker | Yes | No criminal record |
| Henry | 29 | Left school at 15 | Stepdad and mum | Electrician | Yes | 16 |
| Ian Cath | 42 | Left school at 16 | Both parents | Factory worker | Yes | 16 |
| Tom | 36 | Left school at 13 | Children’s home | Never worked | Yes | No criminal record |
| Marie | 35 | Left school at 13 | Children’s care home | Never worked | Yes | No criminal record |
| Leo | 42 | Left school at 16 | Single mum | Plumber, computer tech and supermarket | Yes | No criminal record |
| Norma | 31 | Left school at 16 | Foster care | Cleaner | Yes | No criminal record |
| Crewe | 58 | Left school at 15 | Foster care | Motor mechanic | Yes | 16 |
| Paddy | 35 | Left school at 16 | Mum and stepdad | Never worked | Yes | 14 |
| Matt | 33 | Left school at 16 | Foster care | Builder | Yes | 18 |
| Milly | 31 | Left school at 16 | Foster care | Never worked | Yes | 16 |
| Kieran | 38 | Left school at 16 | Children’s home | Motor mechanic | Yes | 18 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mabhala, M.A.; Yohannes, A. Being at the Bottom Rung of the Ladder in an Unequal Society: A Qualitative Analysis of Stories of People without a Home. Int. J. Environ. Res. Public Health 2019, 16, 4620. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234620
Mabhala MA, Yohannes A. Being at the Bottom Rung of the Ladder in an Unequal Society: A Qualitative Analysis of Stories of People without a Home. International Journal of Environmental Research and Public Health. 2019; 16(23):4620. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234620
Chicago/Turabian StyleMabhala, Mzwandile A., and Asmait Yohannes. 2019. "Being at the Bottom Rung of the Ladder in an Unequal Society: A Qualitative Analysis of Stories of People without a Home" International Journal of Environmental Research and Public Health 16, no. 23: 4620. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234620