Effect of Aerobic Physical Activity on Health-Related Quality of Life in Middle Aged Women with Osteoarthritis: Korea National Health and Nutrition Examination Survey (2016–2017)


Abstract
:1. Introduction
2. Methods
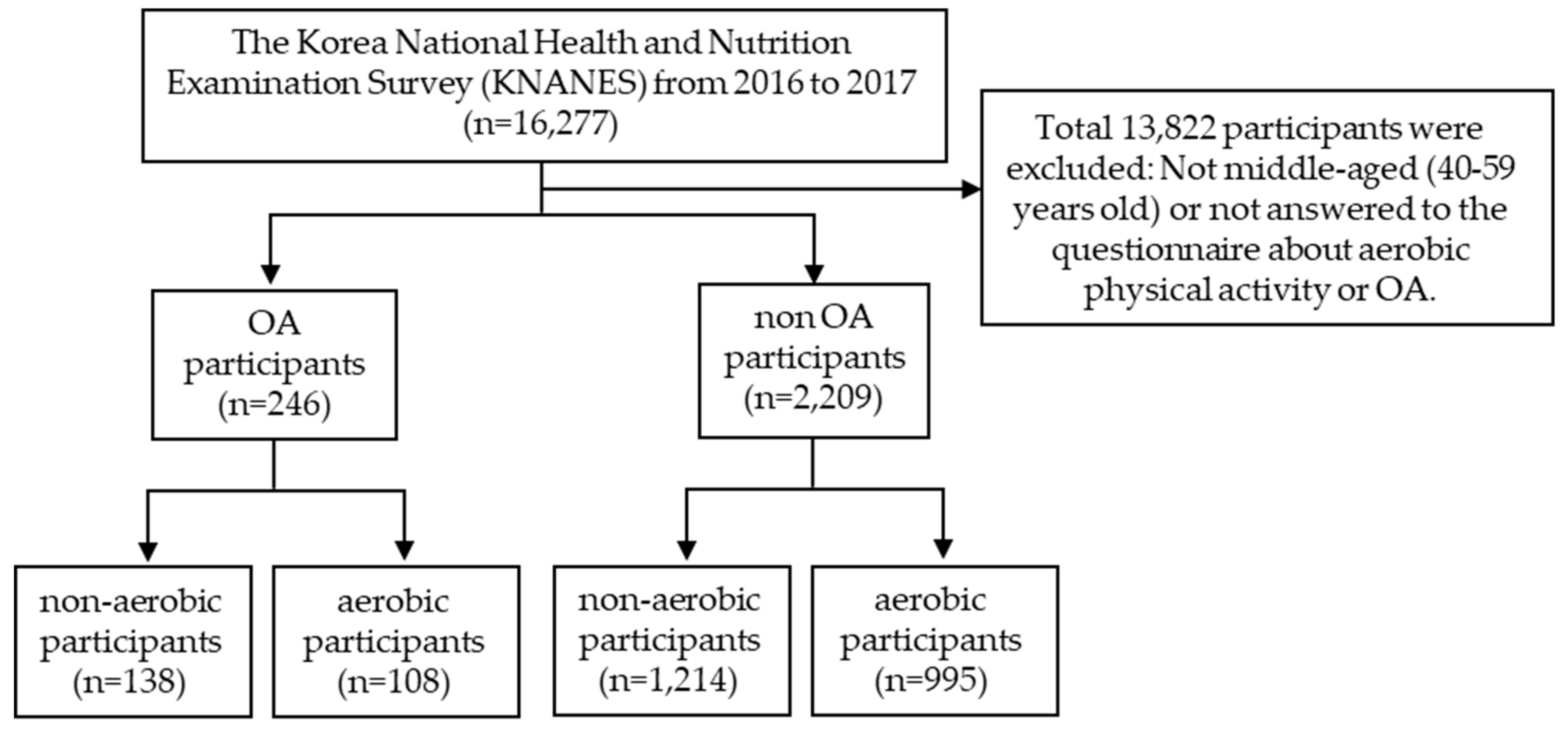
2.1. Study Population and Data Collection
2.2. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Arden, N.; Nevitt, M.C. Osteoarthritis: Epidemiology. Best Pract. Res. Clin. Rheumatol. 2006, 20, 3–25. [Google Scholar] [CrossRef] [PubMed]
- Shane, A.A.; Loeser, R.F. Why is osteoarthritis an age-related disease? Best Pract. Res. Clin. Rheumatol. 2010, 24, 15–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bedson, J.; Jordan, K.; Croft, P. The prevalence and history of knee osteoarthritis in general practice: A case-control study. Fam. Pract. 2005, 22, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Murphy, L.; Helmick, C.G. The impact of osteoarthritis in the United States: A population-health perspective. Am. J. Nurs. 2012, 112 (Suppl. 1), S13–S19. [Google Scholar] [CrossRef]
- Health Insurance Review and Assessment Service, National Health Insurance Service. National Health Insurance Statistical Yearbook; Health Insurance Review and Assessment Service, National Health Insurance Service: Wonju, Korea, 2014. [Google Scholar]
- Salacinski, A.J.; Krohn, K.; Lewis, S.F.; Holland, M.L.; Ireland, K.; Marchetti, G. The effects of group cycling on gait and pain-related disability in individuals with mild-to-moderate knee osteoarthritis: A randomized controlled trial. J. Orthop. Sports Phys. Ther. 2012, 42, 985–995. [Google Scholar] [CrossRef] [PubMed]
- Lund, H.; Weile, U.; Christensen, R.; Rostock, B.; Downey, A.; Bartels, E.M.; Danneskiold-Samsøe, B.; Bliddal, H. A randomized controlled trial of aquatic and land-based exercise in patients with knee osteoarthritis. J. Rehabil. Med. 2008, 40, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, T.; Wada, M.; Kawahara, H.; Sato, M.; Baba, H.; Shimada, S. Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann. Rheum. Dis. 2002, 61, 617–622. [Google Scholar] [CrossRef]
- Mündermann, A.; Dyrby, C.O.; Hurwitz, D.E.; Sharma, L.; Andriacchi, T.P. Potential strategies to reduce medial compartment loading in patients with knee osteoarthritis of varying severity: Reduced walking speed. Arthritis Rheum. 2004, 50, 1172–1178. [Google Scholar] [CrossRef]
- Fayers, P.; Machin, D. Quality of Life: The Assessment, Analysis and Interpretation of Patient-Reported Outcomes, 2nd ed.; John Wiley & Sons Ltd.: Chichester, UK, 2007. [Google Scholar]
- Fishwick, D.; Lewis, L.; Darby, A.; Young, C.; Wiggans, R.; Waterhouse, J.; Wight, J.; Blanc, P.D. Determinants of health-related quality of life among residents with and without COPD in a historically industrialised area. Int. Arch. Occup. Environ. Health 2015, 88, 799–805. [Google Scholar] [CrossRef] [Green Version]
- Tan, Z.; Liang, Y.; Liu, S.; Cao, W.; Tu, H.; Guo, L.; Xu, Y. Health-related quality of life as measured with EQ-5D among populations with and without specific chronic conditions: A population-based survey in Shaanxi Province, China. PLoS ONE 2013, 8, e65958. [Google Scholar] [CrossRef] [Green Version]
- Jang, E.S.; Kim, Y.S.; Kim, K.A.; Lee, Y.J.; Chung, W.J.; Kim, I.H.; Lee, B.S.; Jeong, S.H. Factors Associated with Health-Related Quality of Life in Korean Patients with Chronic Hepatitis C Infection Using the SF-36 and EQ-5D. Gut Liver 2018, 12, 440–448. [Google Scholar] [CrossRef]
- Liu, L.; Li, S.; Wang, M.; Chen, G. Comparison of EQ-5D-5L health state utilities using four country-specific tariffs on a breast cancer patient sample in mainland China. Patient Prefer. Adherence 2017, 23, 1049–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korea Centers for Disease Control and Prevention. 2007 National Health Statistics; Korea Centers for Disease Control and Prevention: Cheongju, Korea, 2007. [Google Scholar]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Pisters, M.F.; Veenhof, C.; van Meeteren, N.L.; Ostelo, R.W.; de Bakker, D.H.; Schellevis, F.G.; Dekker, J. Long-term effectiveness of exercise therapy in patients with osteoarthritis of the hip or knee: A systematic review. Arthritis Rheum. 2007, 57, 1245–1253. [Google Scholar] [CrossRef] [PubMed]
- Van Saase, J.L.; van Romunde, L.K.; Cats, A.; Vandenbroucke, J.P.; Valkenburg, H.A. Epidemiology of osteoarthritis: Zoetermeer survey. Comparison of radiological osteoarthritis in a Dutch population with that in 10 other populations. Ann. Rheum. Dis. 1989, 48, 271–280. [Google Scholar] [CrossRef] [Green Version]
- Mikkelsen, W.M.; Dodge, H.J.; Duff, I.F.; Kato, H. Estimates of the prevalence of rheumatic diseases in the population of Tecumseh, Michigan, 1959–1960. J. Chronic Dis. 1967, 20, 351–369. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, L.S.; Kelsey, J.L. Epidemiology of musculoskeletal impairments and associated disability. Am. J. Public Health 1984, 74, 574–579. [Google Scholar] [CrossRef]
- Felson, D.T.; Naimark, A.; Anderson, J.; Kazis, L.; Castelli, W.; Meenan, R.F. The prevalence of knee osteoarthritis in the elderly. The Framingham Osteoarthritis Study. Arthritis Rheum. 1987, 30, 914–918. [Google Scholar] [CrossRef]
- Cella, D.F.; Tulsky, D.S. Measuring quality of life today: Methodological aspects. Oncology (Williston Park) 1990, 4, 29–38. [Google Scholar]
- Lee, S.; Kim, S.J. Prevalence of knee osteoarthritis, risk factors, and quality of life: The Fifth Korean National Health and Nutrition Examination Survey. Int. J. Rheum. Dis. 2017, 20, 809–817. [Google Scholar] [CrossRef]
- Parker, L.; Moran, G.M.; Roberts, L.M.; Calvert, M.; McCahon, D. The burden of common chronic disease on health-related quality of life in an elderly community-dwelling population in the UK. Fam. Pract. 2014, 31, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.H.; Lee, K.; Jung, S.Y.; Bae, W.K.; Ju, H.J.; Cho, I.Y.; Song, J.K.; Park, H.Y.; Han, J.S.; Lee, G.H.; et al. Osteoarthritis Affects Health-Related Quality of Life in Korean Adults with Chronic Diseases: The Korea National Health and Nutritional Examination Surveys 2009–2013. Korean J. Fam. Med. 2017, 38, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Fransen, M.; McConnell, S. Exercise for osteoarthritis of the knee. Cochrane Database Syst. Rev. 2008, 8, CD004376. [Google Scholar]
- Szychlinska, M.A.; Imbesi, R.; Castrogiovanni, P.; Guglielmino, C.; Ravalli, S.; Di Rosa, M.; Musumeci, G. Assessment of Vitamin D Supplementation on Articular Cartilage Morphology in a Young Healthy Sedentary Rat Model. Nutrients 2019, 11, 1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fransen, M.; McConnell, S.; Bell, M. Therapeutic exercise for people with osteoarthritis of the hip or knee. A systematic review. J. Rheumatol. 2002, 29, 1737–1745. [Google Scholar]
- Van Baar, M.E.; Assendelft, W.J.; Dekker, J.; Oostendorp, R.A.; Bijlsma, J.W. Effectiveness of exercise therapy in patients with osteoarthritis of the hip or knee: A systematic review of randomized clinical trials. Arthritis Rheum. 1999, 42, 1361–1369. [Google Scholar] [CrossRef]
- Smidt, N.; de Vet, H.C.; Bouter, L.M.; Dekker, J.; Arendzen, J.H.; de Bie, R.A.; Bierma-Zeinstra, S.M.; Helders, P.J.; Keus, S.H.; Kwakkel, G.; et al. Effectiveness of exercise therapy: A best-evidence summary of systematic reviews. Aust. J. Physiother. 2005, 51, 71–85. [Google Scholar] [CrossRef] [Green Version]
- Fransen, M.; McConnell, S.; Harmer, A.R.; Van der Esch, M.; Simic, M.; Bennell, K.L. Exercise for osteoarthritis of the knee: A Cochrane systematic review. Br. J. Sports Med. 2015, 49, 1554–1557. [Google Scholar] [CrossRef]
- Roddy, E.; Zhang, W.; Doherty, M. Aerobic walking or strengthening exercise for osteoarthritis of the knee? A systematic review. Ann. Rheum. Dis. 2005, 64, 544–548. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, C.; Lefèvre-Colau, M.M.; Poiraudeau, S.; Rannou, F. Rehabilitation (exercise and strength training) and osteoarthritis: A critical narrative review. Ann. Phys. Rehabil. Med. 2016, 59, 190–195. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, S.C.; Muir, K.R.; Doherty, M. Effectiveness of home exercise on pain and disability from osteoarthritis of the knee: A randomised controlled trial. Ann. Rheum. Dis. 1999, 58, 15–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juhl, C.; Christensen, R.; Roos, E.M.; Zhang, W.; Lund, H. Impact of exercise type and dose on pain and disability in knee osteoarthritis: A systematic review and meta-regression analysis of randomized controlled trials. Arthritis Rheumatol. 2014, 66, 622–636. [Google Scholar] [CrossRef] [PubMed]
- Roddy, E.; Zhang, W.; Doherty, M.; Arden, N.K.; Barlow, J.; Birrell, F.; Carr, A.; Chakravarty, K.; Dickson, J.; Hay, E.; et al. Evidence-based recommendations for the role of exercise in the management of osteoarthritis of the hip or knee—The MOVE consensus. Rheumatology 2005, 44, 67–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Item | non-OA a (n = 2209) | OA a (n = 246) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-Aerobic (n = 1214) | Aerobic (n = 995) | p-Value | Non-Aerobic (n = 138) | Aerobic (n = 108) | p-Value | ||||||
| n | % | n | % | n | % | n | % | ||||
| Age (years) | >40 | 631 | 52.0 | 520 | 52.3 | 0.034 * | 26 | 18.8 | 18 | 16.7 | 0.121 |
| <59 | 583 | 48.0 | 475 | 47.7 | 112 | 81.2 | 90 | 83.3 | |||
| Income level | level 1 | 307 | 25.3 | 214 | 21.5 | <0.001 ** | 46 | 33.3 | 35 | 32.4 | 0.046 * |
| level 2 | 322 | 26.6 | 237 | 23.8 | 35 | 25.4 | 25 | 23.1 | |||
| level 3 | 287 | 23.7 | 260 | 26.1 | 30 | 21.7 | 30 | 27.8 | |||
| level 4 | 296 | 24.4 | 284 | 28.5 | 27 | 19.6 | 18 | 16.7 | |||
| Education level | elementary | 110 | 9.1 | 58 | 5.8 | <0.001 ** | 42 | 30.4 | 18 | 16.7 | 0.006 ** |
| middle | 130 | 10.7 | 89 | 9.0 | 26 | 18.8 | 22 | 20.4 | |||
| high | 526 | 43.4 | 425 | 42.8 | 46 | 33.3 | 48 | 44.4 | |||
| university | 445 | 36.7 | 422 | 42.5 | 24 | 17.4 | 20 | 18.5 | |||
| Marital status | single | 37 | 3.1 | 35 | 3.5 | 0.004 ** | 1 | 0.7 | 1 | 0.9 | 0.097 |
| marriaged | 1022 | 84.3 | 864 | 86.9 | 109 | 79.0 | 89 | 82.4 | |||
| divorced | 154 | 12.7 | 95 | 9.6 | 28 | 20.3 | 18 | 16.7 | |||
| Economic activity | no | 417 | 34.4 | 414 | 41.6 | <0.001 ** | 52 | 37.7 | 39 | 36.1 | 0.103 |
| yes | 796 | 65.6 | 581 | 58.4 | 86 | 62.3 | 69 | 63.9 | |||
| Type of insurance | local | 408 | 33.7 | 253 | 25.5 | <0.001 ** | 48 | 34.8 | 34 | 31.5 | 0.087 |
| company | 764 | 63.2 | 719 | 72.5 | 78 | 56.5 | 70 | 64.8 | |||
| gov. cover | 37 | 3.1 | 20 | 2.0 | 12 | 8.7 | 4 | 3.7 | |||
| Private insurance | no | 97 | 8.0 | 66 | 6.6 | 0.031 * | 20 | 14.5 | 10 | 9.3 | 0.074 |
| yes | 1115 | 92.0 | 928 | 93.4 | 118 | 85.5 | 98 | 90.7 | |||
| Self-health status | good | 301 | 24.8 | 323 | 32.5 | <0.001 ** | 26 | 18.8 | 16 | 14.8 | 0.074 |
| fair | 704 | 58.0 | 531 | 53.4 | 68 | 49.3 | 60 | 55.6 | |||
| bad | 209 | 17.2 | 141 | 14.2 | 44 | 31.9 | 32 | 29.6 | |||
| Drinking | non-drinker | 139 | 11.5 | 91 | 9.2 | 0.003 ** | 20 | 14.5 | 19 | 17.6 | 0.041 * |
| 1 year non-drinker | 215 | 17.8 | 149 | 15.0 | 33 | 23.9 | 20 | 18.5 | |||
| <4/m b | 705 | 58.3 | 634 | 63.8 | 64 | 46.4 | 62 | 57.4 | |||
| >4/m b | 151 | 12.5 | 120 | 12.1 | 21 | 15.2 | 7 | 6.5 | |||
| Smoking | non-smoker | 1081 | 89.4 | 918 | 92.4 | 0.001 ** | 120 | 87.0 | 101 | 93.5 | 0.035 * |
| past | 57 | 4.7 | 43 | 4.3 | 9 | 6.5 | 3 | 2.8 | |||
| present | 71 | 5.9 | 32 | 3.2 | 9 | 6.5 | 4 | 3.7 | |||
| Sleep hours (per day) | <7 | 507 | 41.8 | 446 | 44.8 | 0.003 ** | 59 | 42.8 | 55 | 50.9 | 0.032 * |
| 7 | 386 | 31.8 | 325 | 32.7 | 44 | 31.9 | 30 | 27.8 | |||
| ≥8 | 320 | 26.4 | 224 | 22.5 | 35 | 25.4 | 23 | 21.3 | |||
| Muscle exercise (days/week) | no | 1057 | 87.1 | 736 | 74.0 | <0.001 ** | 116 | 84.1 | 82 | 75.9 | 0.031 * |
| <5 | 117 | 9.6 | 192 | 19.3 | 13 | 9.4 | 16 | 14.8 | |||
| >5 | 39 | 3.2 | 67 | 6.7 | 9 | 6.5 | 10 | 9.3 | |||
| Menopause | menopause | 531 | 44.0 | 431 | 43.4 | 0.033 * | 106 | 76.8 | 84 | 77.8 | 0.120 |
| no-menopause | 677 | 56.0 | 563 | 56.6 | 32 | 23.2 | 24 | 22.2 | |||
| Obesity | low | 42 | 3.5 | 33 | 3.3 | 0.030 * | 3 | 2.2 | 0.084 | ||
| normal | 818 | 67.4 | 684 | 68.7 | 78 | 56.5 | 70 | 64.8 | |||
| obesity | 354 | 29.2 | 278 | 27.9 | 57 | 41.3 | 38 | 35.2 | |||
| Item | Group 1 Non-OA a (n = 2209) | Group 2 OA a (n = 246) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group 1-1 Non-Aerobic (n = 1214) | p-Value | Group1-2 Aerobic (n = 995) | p-Value | Group2-1 Non-Aerobic (n = 138) | p-Value | Group2-2 Aerobic (n = 108) | p-Value | ||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||||||
| Age (years) | >40 | 0.97 | 0.06 | 0.006 ** | 0.98 | 0.06 | 0.011 * | 0.89 | 0.20 | 0.869 | 0.92 | 0.11 | 0.749 |
| <59 | 0.96 | 0.07 | 0.97 | 0.07 | 0.90 | 0.15 | 0.91 | 0.11 | |||||
| Income level | level 1 | 0.95 | 0.09 | <0.001 ** | 0.96 | 0.10 | <0.001 ** | 0.82 | 0.23 | <0.001 ** | 0.89 | 0.12 | 0.166 |
| level 2 | 0.97 | 0.06 | 0.97 | 0.06 | 0.95 | 0.09 | 0.91 | 0.11 | |||||
| level 3 | 0.97 | 0.06 | 0.98 | 0.05 | 0.91 | 0.10 | 0.94 | 0.08 | |||||
| level 4 | 0.98 | 0.05 | 0.98 | 0.06 | 0.95 | 0.06 | 0.94 | 0.08 | |||||
| Education level | elementary | 0.95 | 0.09 | <0.001 ** | 0.92 | 0.12 | <0.001 ** | 0.85 | 0.23 | 0.076 | 0.88 | 0.14 | 0.139 |
| middle | 0.95 | 0.08 | 0.95 | 0.11 | 0.91 | 0.13 | 0.90 | 0.10 | |||||
| high | 0.97 | 0.06 | 0.98 | 0.05 | 0.93 | 0.10 | 0.94 | 0.09 | |||||
| university | 0.98 | 0.05 | 0.98 | 0.05 | 0.93 | 0.13 | 0.91 | 0.11 | |||||
| Marital status | single | 0.97 | 0.06 | 0.001 ** | 0.96 | 0.09 | 0.002 ** | 1.00 | . | <0.001 ** | 1.00 | . | 0.442 |
| marriaged | 0.97 | 0.06 | 0.97 | 0.06 | 0.93 | 0.09 | 0.92 | 0.10 | |||||
| divorced | 0.95 | 0.09 | 0.95 | 0.11 | 0.79 | 0.29 | 0.89 | 0.13 | |||||
| Economic activity | no | 0.96 | 0.08 | 0.001 ** | 0.96 | 0.08 | 0.003 ** | 0.83 | 0.22 | <0.001 ** | 0.90 | 0.12 | 0.306 |
| yes | 0.97 | 0.06 | 0.98 | 0.06 | 0.94 | 0.08 | 0.92 | 0.09 | |||||
| Type of insurance | local | 0.97 | 0.07 | <0.001 ** | 0.97 | 0.07 | <0.001 ** | 0.93 | 0.09 | <0.001 ** | 0.88 | 0.12 | 0.014 * |
| company | 0.97 | 0.06 | 0.98 | 0.06 | 0.92 | 0.15 | 0.94 | 0.09 | |||||
| gov. cover | 0.90 | 0.12 | 0.86 | 0.20 | 0.64 | 0.23 | 0.85 | 0.07 | |||||
| Private insurance | no | 0.96 | 0.10 | 0.086 | 0.95 | 0.11 | 0.003 ** | 0.87 | 0.15 | 0.385 | 0.91 | 0.10 | 0.841 |
| yes | 0.97 | 0.06 | 0.97 | 0.06 | 0.90 | 0.16 | 0.92 | 0.11 | |||||
| Self-health status | good | 0.99 | 0.03 | <0.001 ** | 0.99 | 0.03 | <0.001 ** | 0.96 | 0.07 | <0.001 ** | 0.96 | 0.06 | <0.001 ** |
| fair | 0.97 | 0.05 | 0.98 | 0.06 | 0.95 | 0.07 | 0.94 | 0.07 | |||||
| bad | 0.92 | 0.11 | 0.91 | 0.12 | 0.78 | 0.23 | 0.85 | 0.14 | |||||
| Drinking | non-drinker | 0.97 | 0.06 | 0.319 | 0.97 | 0.06 | 0.022 * | 0.89 | 0.22 | 0.603 | 0.91 | 0.12 | 0.953 |
| 1 year non-drinker | 0.96 | 0.08 | 0.96 | 0.08 | 0.89 | 0.09 | 0.92 | 0.12 | |||||
| <4/m b | 0.97 | 0.06 | 0.97 | 0.07 | 0.90 | 0.19 | 0.92 | 0.09 | |||||
| >4/m b | 0.96 | 0.07 | 0.98 | 0.04 | 0.94 | 0.07 | 0.91 | 0.15 | |||||
| Smoking | non-smoker | 0.97 | 0.06 | 0.154 | 0.97 | 0.07 | 0.406 | 0.90 | 0.16 | 0.409 | 0.92 | 0.10 | 0.236 |
| past | 0.96 | 0.07 | 0.97 | 0.06 | 0.90 | 0.11 | 0.82 | 0.23 | |||||
| present | 0.96 | 0.08 | 0.96 | 0.09 | 0.83 | 0.19 | 0.88 | 0.19 | |||||
| Sleep hours (per day) | <7 | 0.97 | 0.07 | 0.242 | 0.97 | 0.07 | 0.340 | 0.88 | 0.21 | 0.591 | 0.90 | 0.12 | 0.144 |
| 7 | 0.97 | 0.06 | 0.98 | 0.07 | 0.91 | 0.11 | 0.94 | 0.09 | |||||
| ≥8 | 0.97 | 0.06 | 0.97 | 0.07 | 0.92 | 0.12 | 0.93 | 0.08 | |||||
| Muscle exercise (days/week) | no | 0.97 | 0.07 | 0.411 | 0.97 | 0.07 | 0.300 | 0.90 | 0.13 | 0.047 * | 0.91 | 0.11 | 0.902 |
| <5 | 0.97 | 0.06 | 0.98 | 0.06 | 0.94 | 0.10 | 0.93 | 0.10 | |||||
| >5 | 0.98 | 0.04 | 0.98 | 0.04 | 0.78 | 0.39 | 0.92 | 0.10 | |||||
| Menopause | menopause | 0.96 | 0.07 | 0.001 ** | 0.96 | 0.08 | 0.001 ** | 0.90 | 0.16 | 0.750 | 0.91 | 0.11 | 0.082 |
| no-menopause | 0.97 | 0.06 | 0.98 | 0.06 | 0.91 | 0.18 | 0.95 | 0.07 | |||||
| Obesity | low | 0.96 | 0.06 | <0.001 ** | 0.97 | 0.08 | 0.041 * | 0.93 | 0.07 | 0.946 | 0.92 | 0.10 | 0.551 |
| normal | 0.97 | 0.06 | 0.98 | 0.06 | 0.90 | 0.17 | 0.91 | 0.11 | |||||
| obesity | 0.96 | 0.08 | 0.96 | 0.08 | 0.90 | 0.16 | 0.92 | 0.11 | |||||
| Item | non-OA a (n = 2209) | OA a (n = 246) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-Aerobic (n = 1214) | Aerobic (n = 995) | Non-Aerobic (n = 138) | Aerobic (n = 108) | ||||||||||
| Age (years) | >40 | 0.003 | 0.005 | 0.543 | −0.001 | 0.006 | 0.797 | −0.032 | 0.036 | 0.376 | −0.043 | 0.032 | 0.182 |
| <59 | - | - | - | - | |||||||||
| Income level | level 1 | −0.002 | 0.005 | 0.743 | −0.003 | 0.006 | 0.667 | −0.067 | 0.033 | 0.041 * | −0.039 | 0.032 | 0.216 |
| level 2 | 0.002 | 0.005 | 0.641 | −0.001 | 0.005 | 0.854 | −0.020 | 0.031 | 0.528 | −0.054 | 0.030 | 0.067 | |
| level 3 | 0.002 | 0.005 | 0.661 | 0.002 | 0.005 | 0.760 | −0.045 | 0.034 | 0.185 | −0.010 | 0.029 | 0.723 | |
| level 4 | - | - | - | - | |||||||||
| Education level | elementary | −0.016 | 0.007 | 0.020 * | −0.025 | 0.010 | 0.008 ** | −0.019 | 0.034 | 0.585 | 0.007 | 0.036 | 0.847 |
| middle | −0.008 | 0.006 | 0.223 | −0.016 | 0.008 | 0.045 * | 0.024 | 0.035 | 0.493 | 0.008 | 0.031 | 0.792 | |
| high | 0.001 | 0.004 | 0.731 | 0.002 | 0.004 | 0.602 | 0.033 | 0.032 | 0.297 | 0.016 | 0.026 | 0.543 | |
| university | - | - | - | - | |||||||||
| Marital status | single | 0.010 | 0.011 | 0.389 | −0.001 | 0.012 | 0.938 | 0.039 | 0.150 | 0.792 | −0.003 | 0.097 | 0.975 |
| marriaged | 0.007 | 0.006 | 0.183 | 0.005 | 0.007 | 0.467 | 0.025 | 0.030 | 0.401 | 0.013 | 0.026 | 0.618 | |
| divorced | - | - | - | - | |||||||||
| Economic activity | no | −0.008 | 0.004 | 0.030 * | −0.009 | 0.004 | 0.021 * | −0.041 | 0.024 | 0.084 | −0.026 | 0.020 | 0.212 |
| yes | - | 0 a | 0 a | 0 a | |||||||||
| Type of insurance | local | 0.049 | 0.011 | <0.001 ** | 0.086 | 0.015 | <0.001 ** | 0.123 | 0.047 | 0.008 ** | −0.016 | 0.048 | 0.737 |
| company | 0.054 | 0.011 | <0.001 ** | 0.090 | 0.015 | <0.001 ** | 0.101 | 0.046 | 0.027 * | 0.053 | 0.047 | 0.263 | |
| gov. cover | - | - | - | - | |||||||||
| Private insurance | no | 0.001 | 0.007 | 0.895 | −0.004 | 0.008 | 0.643 | 0.030 | 0.030 | 0.312 | −0.009 | 0.034 | 0.793 |
| yes | - | - | - | - | |||||||||
| Self-health status | good | 0.069 | 0.006 | <0.001 ** | 0.062 | 0.007 | <0.001 ** | 0.120 | 0.032 | <0.001 ** | 0.122 | 0.031 | <0.001 ** |
| fair | 0.055 | 0.005 | <0.001 ** | 0.052 | 0.006 | <0.001 ** | 0.135 | 0.024 | <0.001 ** | 0.093 | 0.021 | <0.001 ** | |
| bad | - | - | - | - | |||||||||
| Drinking | non-drinker | 0.013 | 0.007 | 0.062 | −0.008 | 0.009 | 0.350 | 0.002 | 0.040 | 0.958 | 0.014 | 0.043 | 0.747 |
| 1 year non-drinker | 0.009 | 0.006 | 0.157 | −0.015 | 0.008 | 0.049 | −0.001 | 0.035 | 0.969 | 0.025 | 0.040 | 0.537 | |
| <4/m b | 0.007 | 0.005 | 0.198 | −0.011 | 0.006 | 0.078 | 0.006 | 0.031 | 0.841 | 0.012 | 0.039 | 0.766 | |
| >4/m b | - | - | - | - | |||||||||
| Smoking | non-smoker | −0.006 | 0.008 | 0.400 | 0.003 | 0.011 | 0.765 | −0.018 | 0.041 | 0.670 | −0.021 | 0.051 | 0.678 |
| past | −0.008 | 0.011 | 0.453 | 0.001 | 0.014 | 0.933 | 0.015 | 0.055 | 0.781 | −0.056 | 0.073 | 0.444 | |
| present | - | - | - | - | |||||||||
| Sleep hours (per day) | <7 | −0.010 | 0.004 | 0.020 * | 0.001 | 0.005 | 0.818 | −0.013 | 0.026 | 0.624 | −0.048 | 0.022 | 0.030 * |
| 7 | −0.004 | 0.005 | 0.436 | 0.004 | 0.005 | 0.417 | −0.014 | 0.027 | 0.604 | −0.030 | 0.027 | 0.270 | |
| ≥8 | - | - | - | - | |||||||||
| Muscle exercise (days/week) | no | −0.008 | 0.010 | 0.387 | −0.010 | 0.008 | 0.193 | 0.141 | 0.042 | 0.001 ** | 0.034 | 0.030 | 0.256 |
| <5 | −0.009 | 0.011 | 0.413 | −0.011 | 0.009 | 0.211 | 0.173 | 0.053 | 0.001 ** | 0.029 | 0.035 | 0.408 | |
| >5 | - | - | - | - | |||||||||
| Menopause | menopause | −0.003 | 0.005 | 0.482 | −0.006 | 0.006 | 0.298 | 0.006 | 0.031 | 0.858 | −0.079 | 0.028 | 0.005 ** |
| no-menopause | - | - | - | - | |||||||||
| Obesity | low | −0.005 | 0.010 | 0.623 | 0.001 | 0.011 | 0.945 | 0.015 | 0.088 | 0.867 | |||
| normal | 0.006 | 0.004 | 0.127 | 0.003 | 0.004 | 0.557 | −0.003 | 0.022 | 0.884 | −0.021 | 0.018 | 0.259 | |
| obesity | - | - | - | - | |||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryu, M.; Lee, S.; Kim, H.; Baek, W.-C.; Kimm, H. Effect of Aerobic Physical Activity on Health-Related Quality of Life in Middle Aged Women with Osteoarthritis: Korea National Health and Nutrition Examination Survey (2016–2017). Int. J. Environ. Res. Public Health 2020, 17, 527. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020527
Ryu M, Lee S, Kim H, Baek W-C, Kimm H. Effect of Aerobic Physical Activity on Health-Related Quality of Life in Middle Aged Women with Osteoarthritis: Korea National Health and Nutrition Examination Survey (2016–2017). International Journal of Environmental Research and Public Health. 2020; 17(2):527. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020527
Chicago/Turabian StyleRyu, Mikyung, Sol Lee, Ho Kim, Weon-Chil Baek, and Heejin Kimm. 2020. "Effect of Aerobic Physical Activity on Health-Related Quality of Life in Middle Aged Women with Osteoarthritis: Korea National Health and Nutrition Examination Survey (2016–2017)" International Journal of Environmental Research and Public Health 17, no. 2: 527. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020527