Knowledge Visualizations to Inform Decision Making for Improving Food Accessibility and Reducing Obesity Rates in the United States

 , and
, and
Abstract
:
1. Introduction
1.1. Overview
1.2. Knowledge Visualization for Knowledge Creation Activities in Public Health
1.3. Food Access Research Atlas Dataset for Public Health Knowledge Creation
1.4. Need for Knowledge Visualizations to Communicate Knowledge on Food Access Measures in the Food Access Research Atlas Dataset
1.5. Need for Knowledge Visualizations to Communicate Knowledge on Adult Obesity Rates in Census Tracts with Identical Food Access Measures
2. Materials and Methods
2.1. Overview
- (1)
- Data Source for Constructing Food Access Patterns for Census Tracts in the United States.
- (2)
- Construction of Food Access Patterns using Variables with Binary Values (0 or 1).
- (3)
- Design and Implementation of Interactive Visualizations as Solutions for Grouping Census Tracts by Food Access Patterns.
- (4)
- Comparison of Obesity Rates in Census Tracts.
2.2. Data Sources for Constructing Food Access Patterns for Census Tracts in the United States
2.3. Construction of Food Access Patterns Using Variables with Binary Values (0 or 1)
2.4. Design and Implementation of Interactive Visualizations as Solutions for Grouping Census Tracts by Food Access Patterns
2.5. Comparison of Obesity Rates in Census Tracts
3. Results
3.1. Overview
3.2. Groups of Census Tracts by Food Access Patterns
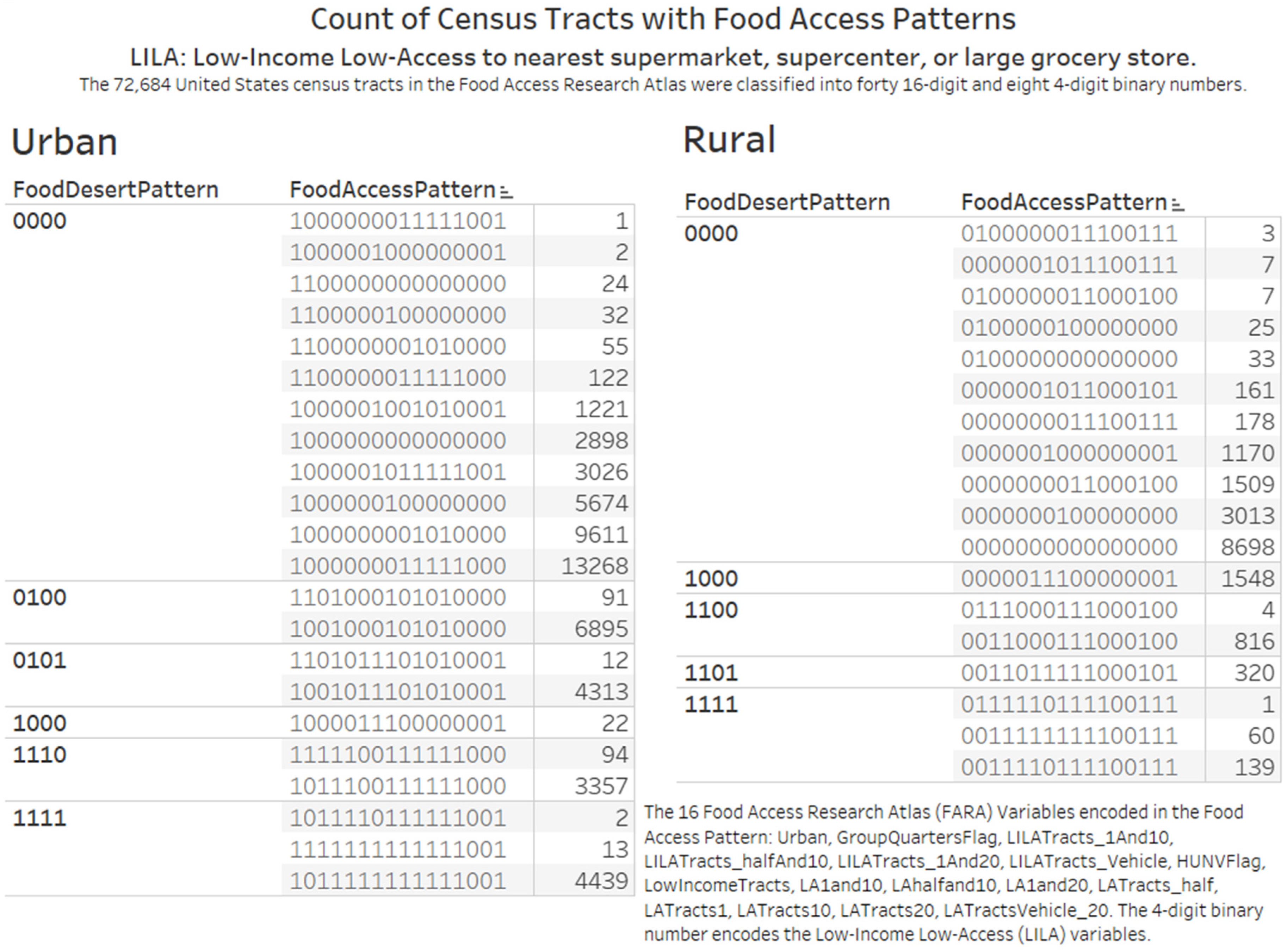
3.2.1. Knowledge Visualization for Knowledge Transfer on Counts of Census Tracts in Rural and Urban Locations
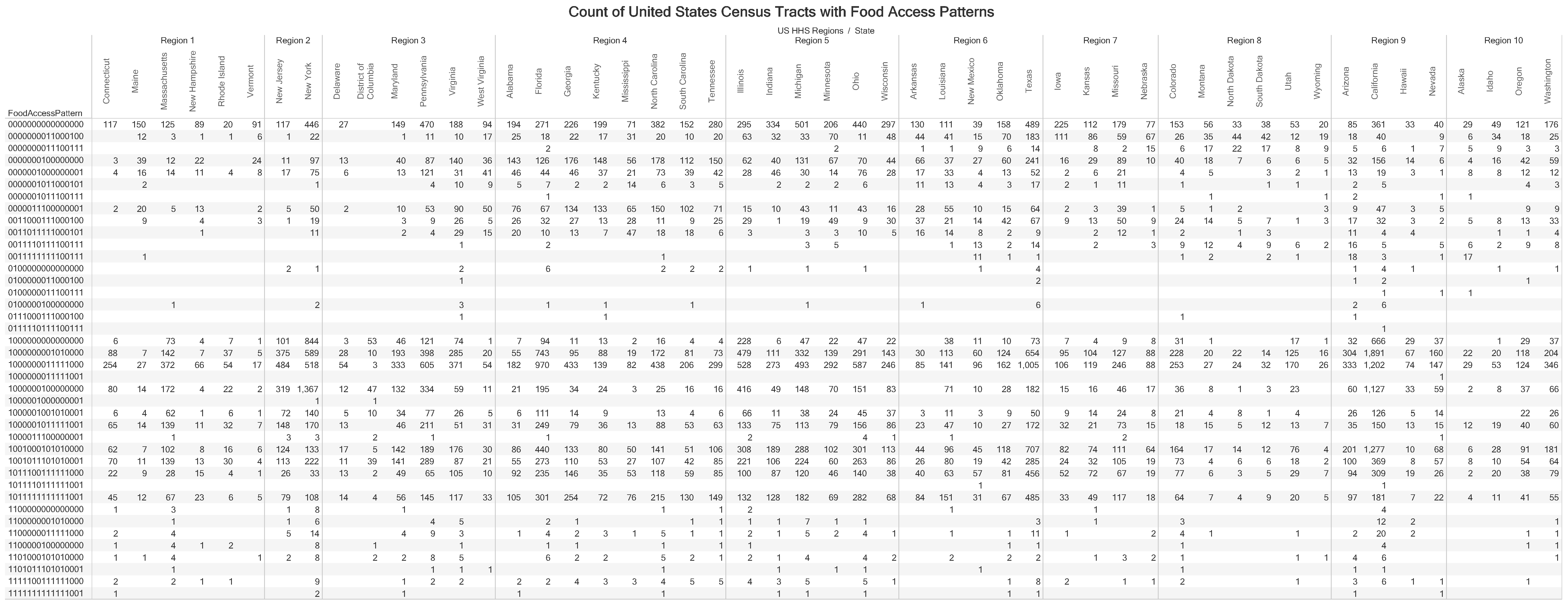
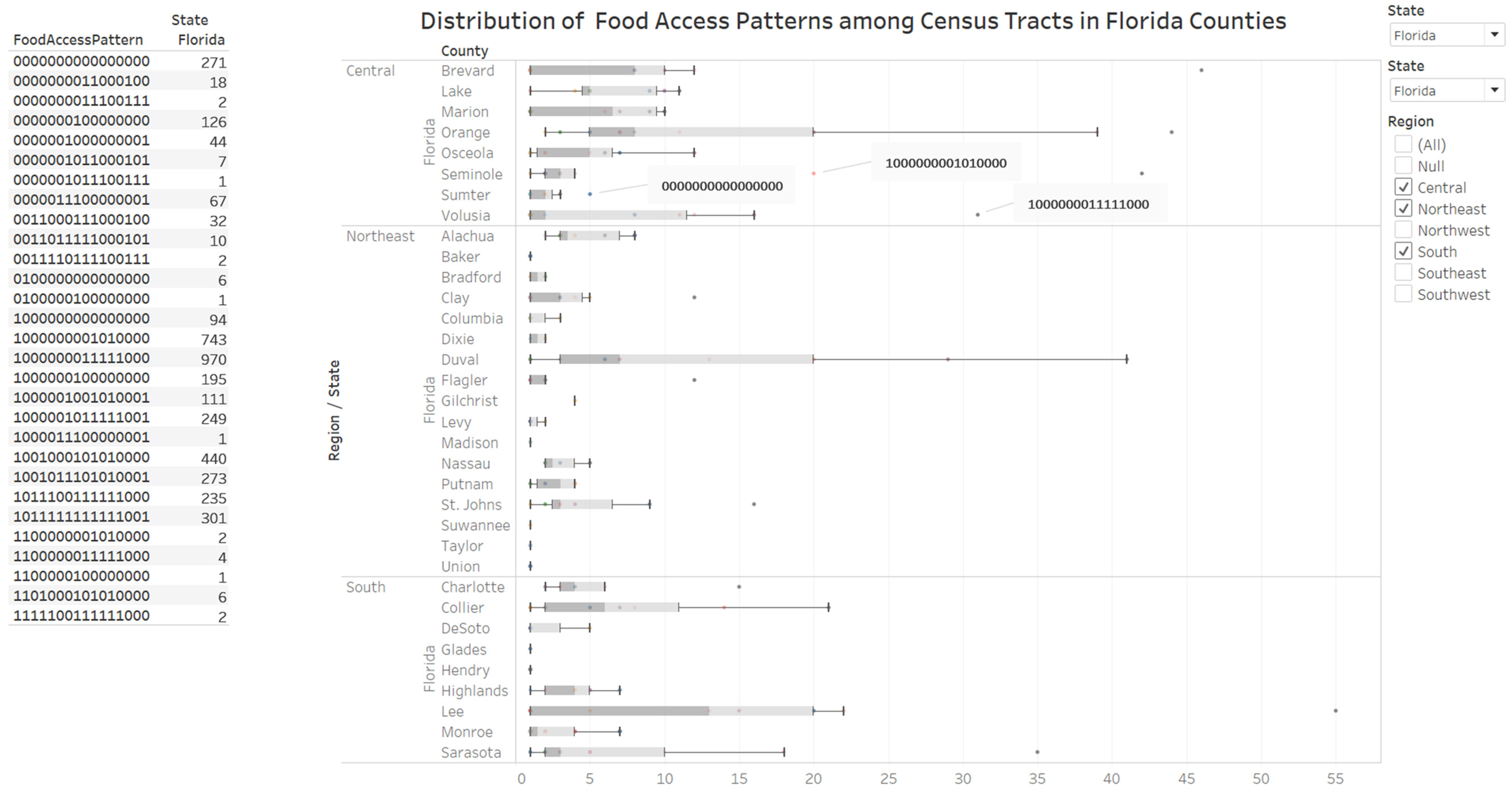
3.2.2. Knowledge Visualization for Elaboration of the Distribution of Food Access Measures by States
3.2.3. Knowledge Visualization for Coordination of Environmental Protection Regions and Food Accessibility
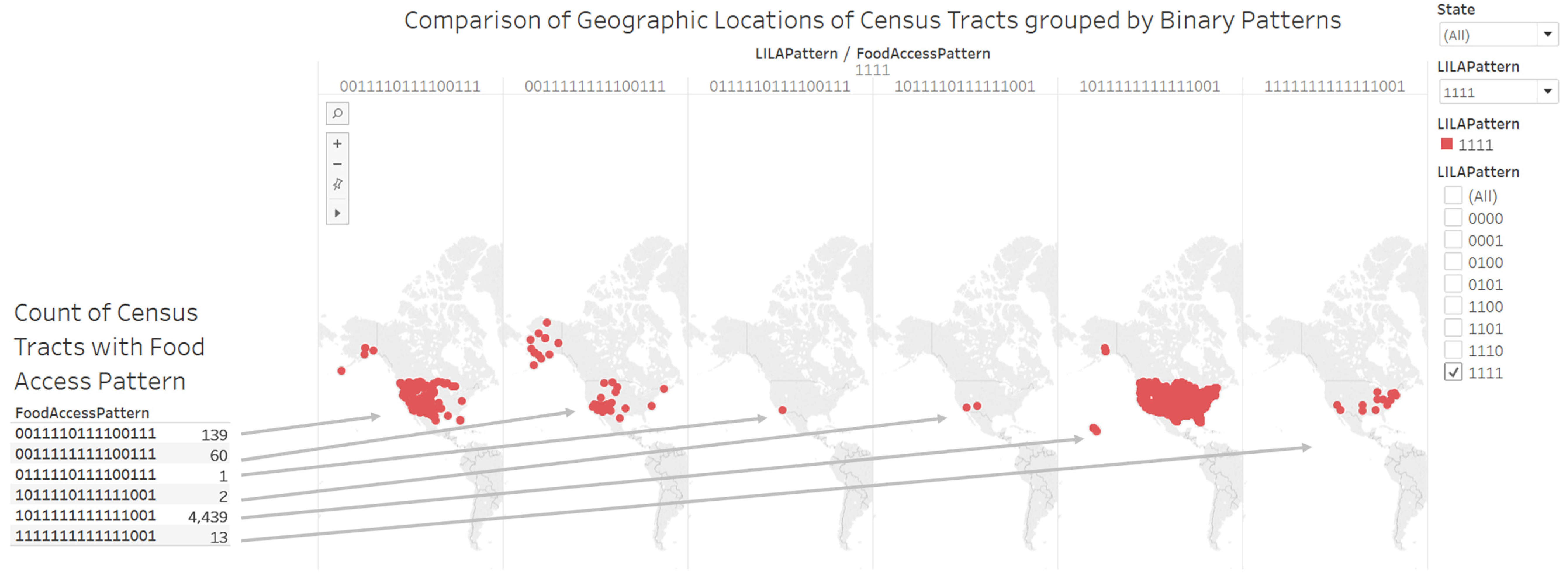
3.2.4. Knowledge Visualization for Attention and Motivation on Locations of Low-Income Low-Access Census Tracts
3.2.5. Knowledge Visualization for New Insights on General Tract Characteristics of Census Tracts with Identical Food Access Pattern
3.2.6. Knowledge Visualization for Attention to Food Accessibility in Rural Census Tracts
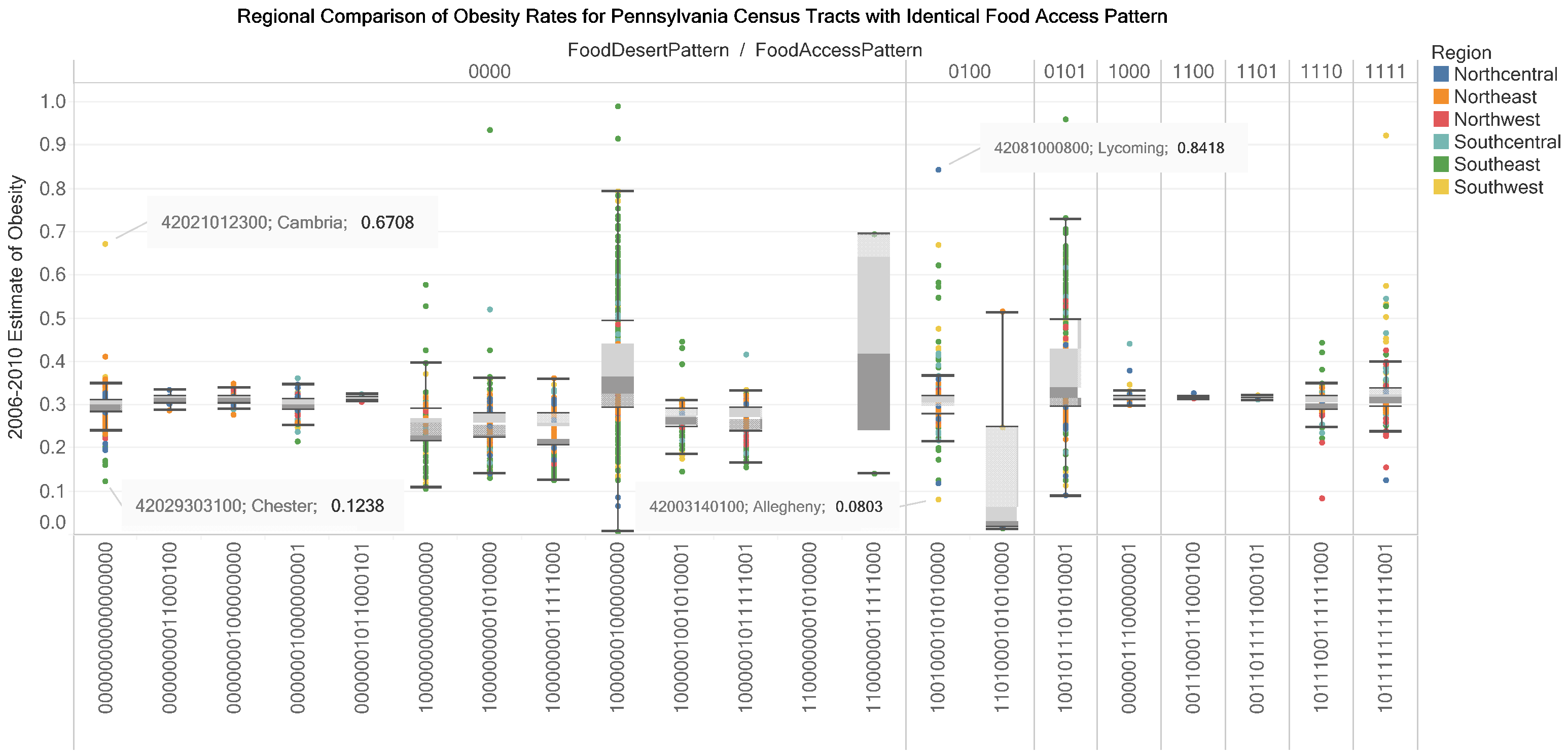
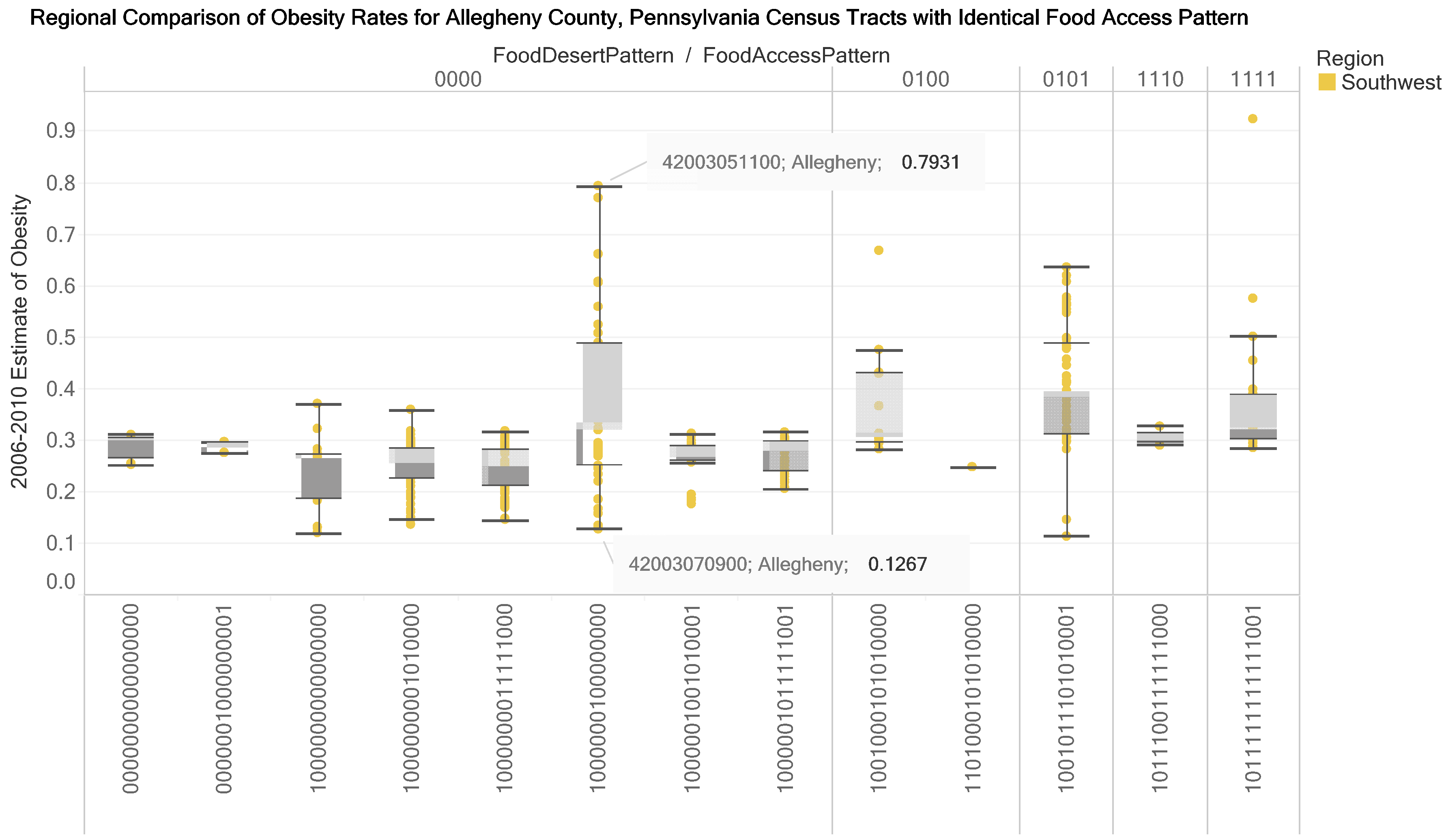
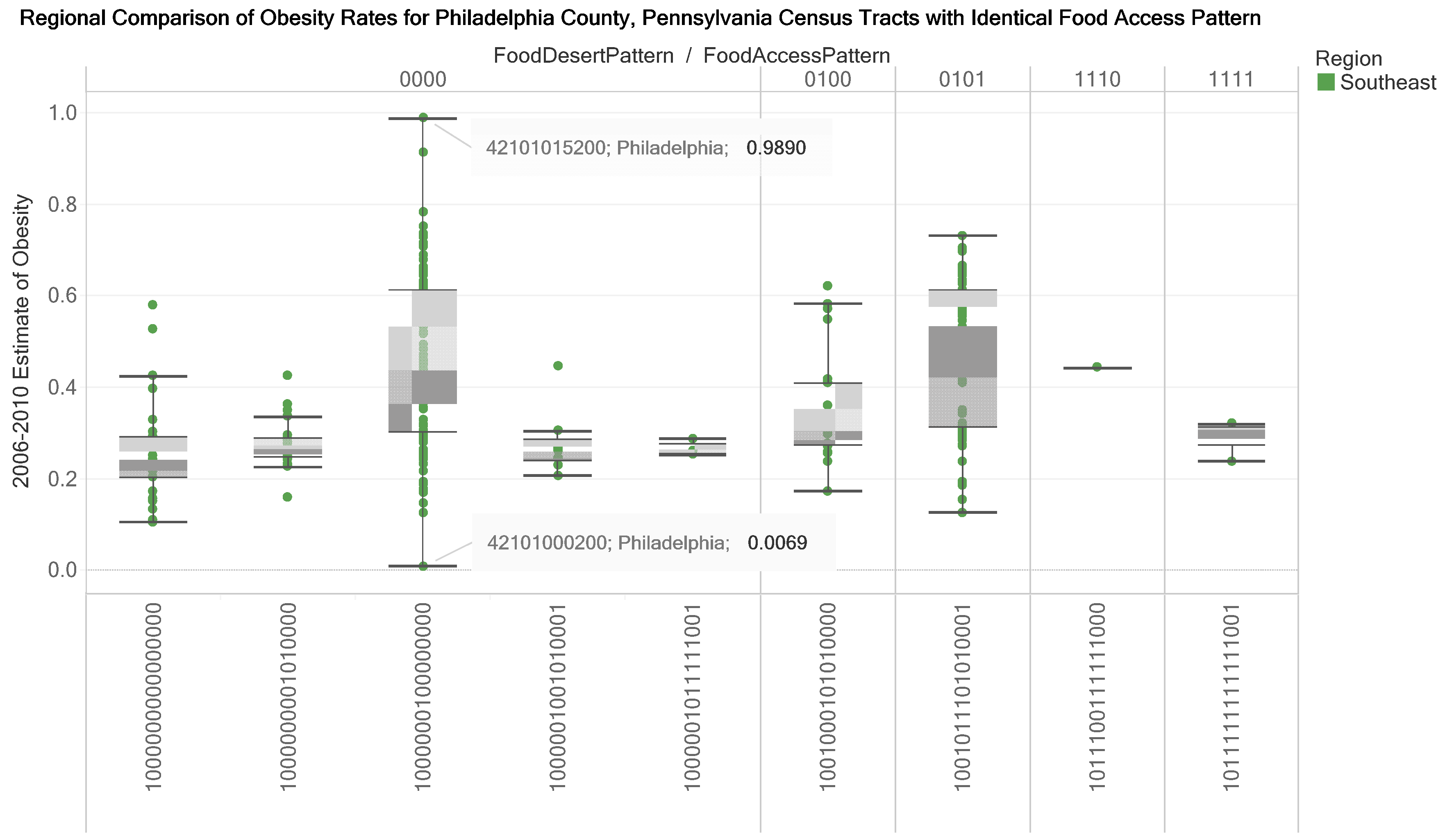
3.3. Knowledge Visualizations to Inform Decision Making for Improving Food Accessibility and Reducing Adult Obesity Rates
4. Discussion
4.1. Overview
4.2. Knowledge Visualization as Integrated Explanation and Prediction System in Public Health
4.3. Validation of the Accuracy of Value-Added Datasets
4.4. Opportunities for Natural Language Processing of Large-Scale Text on Food Access
4.5. Opportunities to Collect Primary Data on Rural Census Tracts on Factors Influencing Obesity Rates
4.6. Opportunities for Census Tract Level Research on Nutritional Inequality and Nutrition Therapy in Diabetic Care
4.7. Limitations of Research and Strategies to Address Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Caspi, C.E.; Sorensen, G.; Subramanian, S.; Kawachi, I. The local food environment and diet: a systematic review. Health Place 2012, 18, 1172–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, C.; Aggarwal, A.; Walls, H.; Herforth, A.; Drewnowski, A.; Coates, J.; Kalamatianou, S.; Kadiyala, S. Concepts and critical perspectives for food environment research: A global framework with implications for action in low-and middle-income countries. Global Food Secur. 2018, 18, 93–101. [Google Scholar] [CrossRef]
- Andress, L.; Fitch, C. Juggling the five dimensions of food access: Perceptions of rural low income residents. Appetite 2016, 105, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Usher, K.M. Valuing all knowledges through an expanded definition of access. J. Agric. Food Syst. Community Dev. 2016, 5, 109–114. [Google Scholar] [CrossRef] [Green Version]
- Economic Research Service (ERS) U.S. Department of Agriculture (USDA). Food Access Research Atlas. Available online: http://www.ers.usda.gov/data-products/food-access-research-atlas.aspx (accessed on 3 March 2017).
- Ver Ploeg, M.; Dutko, P.; Breneman, V. Measuring food access and food deserts for policy purposes. Appl. Econ. Perspect. Policy 2015, 37, 205–225. [Google Scholar] [CrossRef] [Green Version]
- Rhone, A.; Ver Ploeg, M.; Dicken, C.; Williams, R.; Breneman, V. Low-Income and Low-Supermarket-Access Census Tracts, 2010–2015; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2017.
- Rhone, A.; Ver Ploeg, M.; Williams, R.; Breneman, V. Understanding Low-Income and Low-Access Census Tracts Across the Nation: Subnational and Subpopulation Estimates of Access to Healthy Food; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2019.
- Landry, R.; Amara, N.; Pablos-Mendes, A.; Shademani, R.; Gold, I. The knowledge-value chain: a conceptual framework for knowledge translation in health. Bull. World Health Organ. 2006, 84, 597–602. [Google Scholar] [CrossRef]
- Renaud, K.; Van Biljon, J. A framework to maximise the communicative power of knowledge visualisations. In Proceedings of the South African Institute of Computer Scientists and Information Technologists (SAICSIT), Skukuza, South Africa, 17–19 September 2019. [Google Scholar]
- Kastens, K. Pervasive and Persistent Understandings about Data; Oceans of Data Institute: Waltham, MA, USA, 2014; pp. 1–4. [Google Scholar]
- Ola, O.; Sedig, K. Discourse with Visual Health Data: Design of Human-Data Interaction. Multimodal Technol. Interact. 2018, 2, 10. [Google Scholar] [CrossRef] [Green Version]
- Dammann, O. Data, Information, Evidence, and Knowledge: A Proposal for Health Informatics and Data Science. Online J. Public Health Inform. 2018, 10, 244. [Google Scholar] [CrossRef]
- Burkhard, R.A. Learning from architects: the difference between knowledge visualization and information visualization. In Proceedings of the Eighth International Conference on Information Visualisation, London, UK, 14–16 July 2004; pp. 519–524. [Google Scholar]
- Mitton, C.; Smith, N.; Peacock, S.; Evoy, B.; Abelson, J. Public participation in health care priority setting: A scoping review. Health Policy 2009, 91, 219–228. [Google Scholar] [CrossRef]
- Burkhard, R.A. Towards a framework and a model for knowledge visualization: Synergies between information and knowledge visualization. In Knowledge and Information Visualization; Springer: Berlin/Heidelberg, Germany, 2005; pp. 238–255. [Google Scholar]
- Börner, K.; Bueckle, A.; Ginda, M. Data visualization literacy: Definitions, conceptual frameworks, exercises, and assessments. Proc. Natl. Acad. Sci. USA 2019, 116, 1857–1864. [Google Scholar] [CrossRef] [Green Version]
- Major, E.; Delmelle, E.; Delmelle, E. SNAPScapes: Using geodemographic segmentation to classify the food access landscape. Urban Sci. 2018, 2, 71. [Google Scholar] [CrossRef] [Green Version]
- Gailey, S.; Bruckner, T. Obesity among black women in food deserts: An “omnibus” test of differential risk. SSM-Popul. Health 2019, 7, 100363. [Google Scholar] [CrossRef] [PubMed]
- Gourevitch, M.N.; Athens, J.K.; Levine, S.E.; Kleiman, N.; Thorpe, L.E. City-Level Measures of Health, Health Determinants, and Equity to Foster Population Health Improvement: The City Health Dashboard. Am. J. Public Health 2019, 109, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Kelli, H.M.; Kim, J.H.; Samman Tahhan, A.; Liu, C.; Ko, Y.A.; Hammadah, M.; Sullivan, S.; Sandesara, P.; Alkhoder, A.A.; Choudhary, F.K. Living in food deserts and adverse cardiovascular outcomes in patients with cardiovascular disease. J. Am. Heart Assoc. 2019, 8, e010694. [Google Scholar] [CrossRef] [Green Version]
- Madzia, J.; McKinney, D.; Kelly, E.; DeFranco, E. Gestational weight gain and preterm birth risk for underweight women living in Ohio food deserts. Am. J. Obstet. Gynecol. 2019, 220, 468. [Google Scholar] [CrossRef]
- Berkowitz, S.A.; Karter, A.J.; Corbie-Smith, G.; Seligman, H.K.; Ackroyd, S.A.; Barnard, L.S.; Atlas, S.J.; Wexler, D.J. Food insecurity, food “deserts,” and glycemic control in patients with diabetes: a longitudinal analysis. Diabetes Care 2018, 41, 1188–1195. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Baena, D.S.; Perez-Pulido, A.J.; Aguilar− Ruiz, J.S. A biclustering algorithm for extracting bit-patterns from binary datasets. Bioinformatics 2011, 27, 2738–2745. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.; Jaenicke, E.C.; Volpe, R.J. Food environments and obesity: household diet expenditure versus food deserts. Am. J. Public Health 2016, 106, 881–888. [Google Scholar] [CrossRef]
- Gordon-Larsen, P. Food availability/convenience and obesity. Advances in Nutrition: An Int. Rev. J. 2014, 5, 809–817. [Google Scholar] [CrossRef]
- Hilmers, A.; Hilmers, D.C.; Dave, J. Neighborhood disparities in access to healthy foods and their effects on environmental justice. Am. J. Public Health 2012, 102, 1644–1654. [Google Scholar] [CrossRef]
- Ariel-Donges, A.H.; Gordon, E.L.; Dixon, B.N.; Eastman, A.J.; Bauman, V.; Ross, K.M.; Perri, M.G. Rural/urban disparities in access to the National Diabetes Prevention Program. Transl. Behav. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Hinojosa, A.M.O.; Davies, M.M.; Jarjour, S.; Burnett, R.T.; Mann, J.K.; Hughes, E.; Balmes, J.R.; Turner, M.C.; Jerrett, M. Developing small-area predictions for smoking and obesity prevalence in the United States for use in Environmental Public Health Tracking. Environ. Res. 2014, 134, 435–452. [Google Scholar] [CrossRef] [PubMed]
- Le, A.; Judd, S.E.; Allison, D.B.; Oza-Frank, R.; Affuso, O.; Safford, M.M.; Howard, V.J.; Howard, G. The geographic distribution of obesity in the US and the potential regional differences in misreporting of obesity. Obesity 2014, 22, 300–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sims, J.N.; Isokpehi, R.D.; Cooper, G.A.; Bass, M.P.; Brown, S.D.; John, A.L.S.; Gulig, P.A.; Cohly, H.H.P. Visual Analytics of Surveillance Data on Foodborne Vibriosis, United States, 1973–2010. Environ. Health Insights 2011, 5, 71–85. [Google Scholar] [CrossRef] [Green Version]
- Johnson, M.O.; Cozart, T.; Isokpehi, R.D. Harnessing Knowledge for Improving Access to Fruits and Vegetables at Farmers Markets: Interactive Data Visualization to Inform Food Security Programs and Policy. Health Promot. Pract. Online First October 15. 2019. [Google Scholar] [CrossRef]
- Johnson, M.O.; Cohly, H.H.; Isokpehi, R.D.; Awofolu, O.R. The case for visual analytics of arsenic concentrations in foods. Int. J. Environ. Res. Public Health 2010, 7, 1970–1983. [Google Scholar] [CrossRef] [Green Version]
- Isokpehi, R.; Simmons, S.; Johnson, M.; Payton, M. Genomic evidence for bacterial determinants influencing obesity development. Int. J. Environ. Res. Public Health 2017, 14, 345. [Google Scholar] [CrossRef]
- Ahalt, S.; Bedard, D.; Carsey, T.; Crabtree, J.; Green, K.; Jeffries, C.; Knowles, D.; Kum, H.; Lander, H.; Nassar, N. Establishing a National Consortium for Data Science; National Consortium for Data Science: Chapel Hill, NC, USA, 2012. [Google Scholar]
- Sedig, K.; Parsons, P. Interaction design for complex cognitive activities with visual representations: A pattern-based approach. AIS Trans. Hum.-Comput. Interact. 2013, 5, 84–133. [Google Scholar] [CrossRef] [Green Version]
- Parsons, P.; Sedig, K. Common visualizations: Their cognitive utility. In Handbook of Human Centric Visualization; Springer: Berlin/Heidelberg, Germany, 2014; pp. 671–691. [Google Scholar]
- van Biljon, J. Human-Computer Interaction for Development: A knowledge mobilisation framework. Hum.-Comput. Interact. 2018, 12, 13–2018. [Google Scholar]
- Van Biljon, J.; Renaud, K. Harnessing both Information and Knowledge Visualisation to Represent a Community of Practice: Depicting the South African ICT4D Researcher Community. In Proceedings of the African Conference on Information Systems & Technology (ACIST), Cape Town, South Africa, 10–11 July 2017. [Google Scholar]
- Van Biljon, J. Charting the path towards effective knowledge visualisations. In Proceedings of the South African Institute of Computer Scientists and Information Technologists, Thaba Nchu, South Africa, 26–28 September 2017. [Google Scholar]
- Fadiran, O.A.; Van Biljon, J.; Schoeman, M.A. How can visualisation principles be used to support knowledge transfer in teaching and learning? In Proceedings of the 2018 Conference on Information Communications Technology and Society (ICTAS), Durban, South Africa, 8–9 March 2018. [Google Scholar]
- Sacha, D.; Stoffel, A.; Stoffel, F.; Kwon, B.C.; Ellis, G.; Keim, D.A. Knowledge generation model for visual analytics. IEEE Trans. Vis. Comput. Graph. 2014, 20, 1604–1613. [Google Scholar] [CrossRef]
- Carter, M.G. A picture is worth a thousand words: A cross-curricular approach to learning about visuals in STEM. Int. J. Eng. Educ. 2013, 29, 822–828. [Google Scholar]
- Lurie, N.H.; Mason, C.H. Visual representation: Implications for decision making. J. Mark. 2007, 71, 160–177. [Google Scholar] [CrossRef]
- Geraldi, J.; Arlt, M. Confident and “wrong”? Towards a mindful use of visuals in project portfolio decisions. In Proceedings of the International Research Network on Organizing by Projects (IRNOP) Conference, London, UK, 21–24 June 2015. [Google Scholar]
- Börner, K. Atlas of Knowledge: Anyone Can Map; MIT Press: Cambridge, MA, USA, 2015. [Google Scholar]
- Gil, J.D.B.; Reidsma, P.; Giller, K.; Todman, L.; Whitmore, A.; van Ittersum, M. Sustainable development goal 2: Improved targets and indicators for agriculture and food security. Ambio 2019, 48, 685–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, R.; Pan, L.; Blanck, H.M. Racial and Ethnic Disparities in Adult Obesity in the United States: CDC’s Tracking to Inform State and Local Action. Prev. Chronic Dis. 2019, 16, E16. [Google Scholar] [CrossRef] [Green Version]
- Pan, L.; Blanck, H.M.; Park, S.; Galuska, D.A.; Freedman, D.S.; Potter, A.; Petersen, R. State-Specific Prevalence of Obesity Among Children Aged 2–4 Years Enrolled in the Special Supplemental Nutrition Program for Women, Infants, and Children—United States, 2010–2016. Morb. Mortal. Wkly. Rep. 2019, 68, 1057. [Google Scholar] [CrossRef] [Green Version]
- Wen, M.; Fan, J.X.; Kowaleski-Jones, L.; Wan, N. Rural–urban disparities in obesity prevalence among working age adults in the United States: exploring the mechanisms. Am. J. Health Promot. 2018, 32, 400–408. [Google Scholar] [CrossRef]
- Anderson, F.; Burau, K. Back to Basics: Is Civic Agriculture the Solution to Food Deserts in Texas? Open J. Soc. Sci. 2015, 3, 82. [Google Scholar] [CrossRef] [Green Version]
- Wadlington, T.D. Access to Healthy Foods: A Descriptive Analysis of Farmers’ Markets, Food Deserts & USDA Food Assistance Programs in Tennessee Census Tracts; East Tennessee State University: Johnson City, TN, USA, 2017. [Google Scholar]
- Pai, V.M.; Rodgers, M.; Conroy, R.; Luo, J.; Zhou, R.; Seto, B. Workshop on using natural language processing applications for enhancing clinical decision making: an executive summary. J. Am. Med Inform. Assoc. 2013, 21, e2–e5. [Google Scholar] [CrossRef] [Green Version]
- Chowkwanyun, M. Big Data, Large-Scale Text Analysis, and Public Health Research. Am. J. Public Health 2019, 109, S126–S127. [Google Scholar] [CrossRef]
- Johnson, M.; Cozart, T.; Campos, B.; Isokpehi, R. Interactive Data Visualizations of Policy Indicators on Access and Production of Fruits and Vegetables. In Proceedings of the APHA’s 2019 Annual Meeting and Expo, Philadelphia, PA, USA, 2–6 November 2019. [Google Scholar]
- Johnson, C.; Isokpehi, R.; Johnson, M.; Cozart, T. Interactive Analytics of Public Health Aspects of Sickle Cell Disease. In Proceedings of the APHA’s 2019 Annual Meeting and Expo, Philadelphia, PA, USA, 2–6 November 2019. [Google Scholar]
- Yu, H.; Shen, Z.; Miao, C.; Leung, C.; Chen, Y.; Fauvel, S.; Lin, J.; Cui, L.; Pan, Z.; Yang, Q. A dataset of human decision-making in teamwork management. Sci. Data 2017, 4, 160127. [Google Scholar] [CrossRef] [Green Version]
- Befort, C.A.; Nazir, N.; Perri, M.G. Prevalence of obesity among adults from rural and urban areas of the United States: findings from NHANES (2005–2008). J. Rural Health 2012, 28, 392–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porter, G.C.; Laumb, K.; Michaud, T.; Brito, F.; Petreca, D.; Schwieger, G.; Bartee, T.; Yeary, K.H.; Estabrooks, P.A. Understanding the impact of rural weight loss interventions: A systematic review and meta-analysis. Obes. Rev. 2019, 20, 713–724. [Google Scholar] [CrossRef] [PubMed]
- Bixby, H.; Bentham, J.; Zhou, B.; Di Cesare, M.; Paciorek, C.J.; Collaboration, N.R.F. Rising rural body-mass index is the main driver of the global obesity epidemic. Nature 2019, 569, 260–264. [Google Scholar]
- Shikany, J.M.; Carson, T.L.; Hardy, C.M.; Li, Y.; Sterling, S.; Hardy, S.; Walker, C.M.; Baskin, M.L. Assessment of the nutrition environment in rural counties in the Deep South. J. Nutr. Sci. 2018, 7, e72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, L.K.; Enzler, C.; Perry, C.K.; Rodriguez, E.; Mariscal, N.; Linde, S.; Duggan, C. Food availability and food access in rural agricultural communities: use of mixed methods. BMC Public Health 2018, 18, 634. [Google Scholar] [CrossRef] [Green Version]
- DuBreck, C.M.; Sadler, R.C.; Arku, G.; Gilliland, J.A. Examining community and consumer food environments for children: An urban-suburban-rural comparison in Southwestern Ontario. Soc. Sci. Med. 2018, 209, 33–42. [Google Scholar] [CrossRef]
- Shanks, C.B.; Haack, S.; Tarabochia, D.; Bates, K.; Christenson, L. Factors influencing food choices among older adults in the rural western USA. J. Community Health 2017, 42, 511–521. [Google Scholar] [CrossRef]
- Sharpe, P.A.; Liese, A.D.; Bell, B.A.; Wilcox, S.; Hutto, B.E.; Stucker, J. Household food security and use of community food sources and food assistance programs among food shoppers in neighborhoods of low income and low food access. J. Hunger Environ. Nutr. 2018, 13, 482–496. [Google Scholar] [CrossRef]
- Allcott, H.; Diamond, R.; Dubé, J.-P.; Handbury, J.; Rahkovsky, I.; Schnell, M. Food deserts and the causes of nutritional inequality. Q. J. Econ. 2019, 134, 1793–1844. [Google Scholar] [CrossRef]
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S. Nutrition therapy for adults with diabetes or prediabetes: A consensus report. Diabetes Care 2019, 42, 731–754. [Google Scholar] [CrossRef] [Green Version]
- Kolak, M.; Abraham, G.; Talen, M.R. Mapping Census Tract Clusters of Type 2 Diabetes in a Primary Care Population. Prev. Chronic Dis. 2019, 16, E59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.C.; Ta’Loria Young, C.A.K.; Shim, C.J.; Osorio, M.; Vinson, A.J.; Ravenell, J.E.; Wall, S.P. Age Disparities Among Patients With Type 2 Diabetes and Associated Rates of Hospital Use and Diabetic Complications. Prev. Chronic Dis. 2019, 16, E101. [Google Scholar] [CrossRef] [PubMed]
- Kasl, S.V. Current research in the epidemiology and public health of aging--the need for more diverse strategies. Am. J. Public Health 1997, 87, 333–334. [Google Scholar] [CrossRef] [PubMed]
- Kastens, K. The Relationship Between Direct and Data-Mediated Knowledge of the World; Oceans of Data: Waltam, MA, USA, 2014. [Google Scholar]
- Liben, L.S. Developing an understanding of external spatial representations. In Development of Mental Representation: Theories and Applications; Sigel, I.E., Ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1999; pp. 297–321. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Field 1 | LongName | Position in Binary Number |
|---|---|---|
| Urban | Urban tract | 1 |
| GroupQuartersFlag | Group quarters, tract with high share | 2 |
| LILATracts_1And10 | Low income and low access tract measured at 1 mile for urban areas and 10 miles for rural areas | 3 |
| LILATracts_halfAnd10 | Low income and low access tract measured at 1/2 mile for urban areas and 10 miles for rural areas | 4 |
| LILATracts_1And20 | Low income and low access tract measured at 1 mile for urban areas and 20 miles for rural areas | 5 |
| LILATracts_Vehicle | Low income and low access tract using vehicle access or low income and low access tract measured at 20 miles | 6 |
| HUNVFlag | Vehicle access, tract with low vehicle access | 7 |
| LowIncomeTracts | Low income tract | 8 |
| LA1and10 | Low access tract at 1 mile for urban areas and 10 miles for rural areas | 9 |
| LAhalfand10 | Low access tract at 1/2 mile for urban areas and 10 miles for rural areas | 10 |
| LA1and20 | Low access tract at 1 mile for urban areas and 20 miles for rural areas | 11 |
| LATracts_half | Low access tract at 1/2 mile | 12 |
| LATracts1 | Low access tract at 1 mile | 13 |
| LATracts10 | Low access tract at 10 miles | 14 |
| LATracts20 | Low access tract at 20 miles | 15 |
| LATractsVehicle_20 | Low access tract using vehicle access and at 20 miles in rural areas | 16 |
| US HHS Regions 1 | State | Census Tract Count | All Zeros Count | Percent |
|---|---|---|---|---|
| Region 1 | Connecticut | 832 | 117 | 14.1 |
| Maine | 355 | 150 | 42.3 | |
| Massachusetts | 1476 | 125 | 8.5 | |
| New Hampshire | 295 | 89 | 30.2 | |
| Rhode Island | 242 | 20 | 8.26 | |
| Vermont | 184 | 91 | 49.5 | |
| Region 2 | New Jersey | 2007 | 117 | 5.8 |
| New York | 4907 | 446 | 9.1 | |
| Region 3 | Delaware | 218 | 27 | 12.4 |
| Maryland | 1399 | 149 | 10.7 | |
| Pennsylvania | 3218 | 470 | 14.6 | |
| Virginia | 1900 | 188 | 9.9 | |
| West Virginia | 484 | 94 | 19.4 | |
| Region 4 | Alabama | 1179 | 194 | 16.5 |
| Florida | 4214 | 271 | 6.4 | |
| Georgia | 1965 | 226 | 11.5 | |
| Kentucky | 1115 | 199 | 17.9 | |
| Mississippi | 662 | 71 | 10.7 | |
| North Carolina | 2192 | 382 | 17.4 | |
| South Carolina | 1103 | 152 | 13.8 | |
| Tennessee | 1497 | 280 | 18.7 | |
| Region 5 | Illinois | 3121 | 295 | 9.5 |
| Indiana | 1508 | 334 | 22.2 | |
| Michigan | 2774 | 501 | 18.1 | |
| Minnesota | 1336 | 206 | 15.4 | |
| Ohio | 2949 | 440 | 14.9 | |
| Wisconsin | 1395 | 297 | 21.3 |
| US HHS Regions 1 | State | Census Tract Count | All Zeros Count | Percent |
|---|---|---|---|---|
| Region 6 | Arkansas | 686 | 130 | 19.0 |
| Louisiana | 1143 | 111 | 9.7 | |
| New Mexico | 499 | 39 | 7.8 | |
| Oklahoma | 1046 | 158 | 15.1 | |
| Texas | 5258 | 489 | 9.3 | |
| Region 7 | Iowa | 825 | 225 | 27.3 |
| Kansas | 770 | 112 | 14.6 | |
| Missouri | 1393 | 179 | 12.9 | |
| Nebraska | 532 | 77 | 14.5 | |
| Region 8 | Colorado | 1249 | 153 | 12.5 |
| Montana | 271 | 56 | 20.7 | |
| North Dakota | 205 | 33 | 16.1 | |
| South Dakota | 222 | 38 | 17.1 | |
| Utah | 588 | 53 | 9.0 | |
| Wyoming | 132 | 20 | 15.2 | |
| Region 9 | Arizona | 1526 | 85 | 5.6 |
| California | 8044 | 361 | 4.5 | |
| Hawaii | 332 | 33 | 9.9 | |
| Nevada | 687 | 40 | 5.8 | |
| Region 10 | Alaska | 167 | 29 | 17.4 |
| Idaho | 298 | 49 | 16.4 | |
| Oregon | 830 | 121 | 14.6 | |
| Washington | 1455 | 176 | 12.1 |
| Census Tract 1 | State | County |
|---|---|---|
| 01125011200 | Alabama | Tuscaloosa |
| 04013114100 | Arizona | Maricopa |
| 09003503800 | Connecticut | Hartford |
| 18105000201 | Indiana | Monroe |
| 24033807200 | Maryland | Prince George’s |
| 26121000402 | Michigan | Muskegon |
| 32003000700 | Nevada | Clark |
| 36093021001 | New York | Schenectady |
| 36109000400 | New York | Tompkins |
| 37135011602 | North Carolina | Orange |
| 39009973901 | Ohio | Athens |
| 40119010400 | Oklahoma | Payne |
| 48113010000 | Texas | Dallas |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isokpehi, R.D.; Johnson, M.O.; Campos, B.; Sanders, A.; Cozart, T.; Harvey, I.S. Knowledge Visualizations to Inform Decision Making for Improving Food Accessibility and Reducing Obesity Rates in the United States. Int. J. Environ. Res. Public Health 2020, 17, 1263. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041263
Isokpehi RD, Johnson MO, Campos B, Sanders A, Cozart T, Harvey IS. Knowledge Visualizations to Inform Decision Making for Improving Food Accessibility and Reducing Obesity Rates in the United States. International Journal of Environmental Research and Public Health. 2020; 17(4):1263. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041263
Chicago/Turabian StyleIsokpehi, Raphael D., Matilda O. Johnson, Bryanna Campos, Arianna Sanders, Thometta Cozart, and Idethia S. Harvey. 2020. "Knowledge Visualizations to Inform Decision Making for Improving Food Accessibility and Reducing Obesity Rates in the United States" International Journal of Environmental Research and Public Health 17, no. 4: 1263. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041263