Online Survey for the Assessment of Generic Health Literacy among Adolescents in Germany (GeKoJu): Study Protocol

 , ,
, ,
Abstract
:1. Introduction
1.1. Background
1.2. Objectives
2. Research Design, Methodology, and Methods
2.1. Study Design
2.2. Study Population
2.3. Sampling Strategies
2.4. Data Protection and Ethics Approval
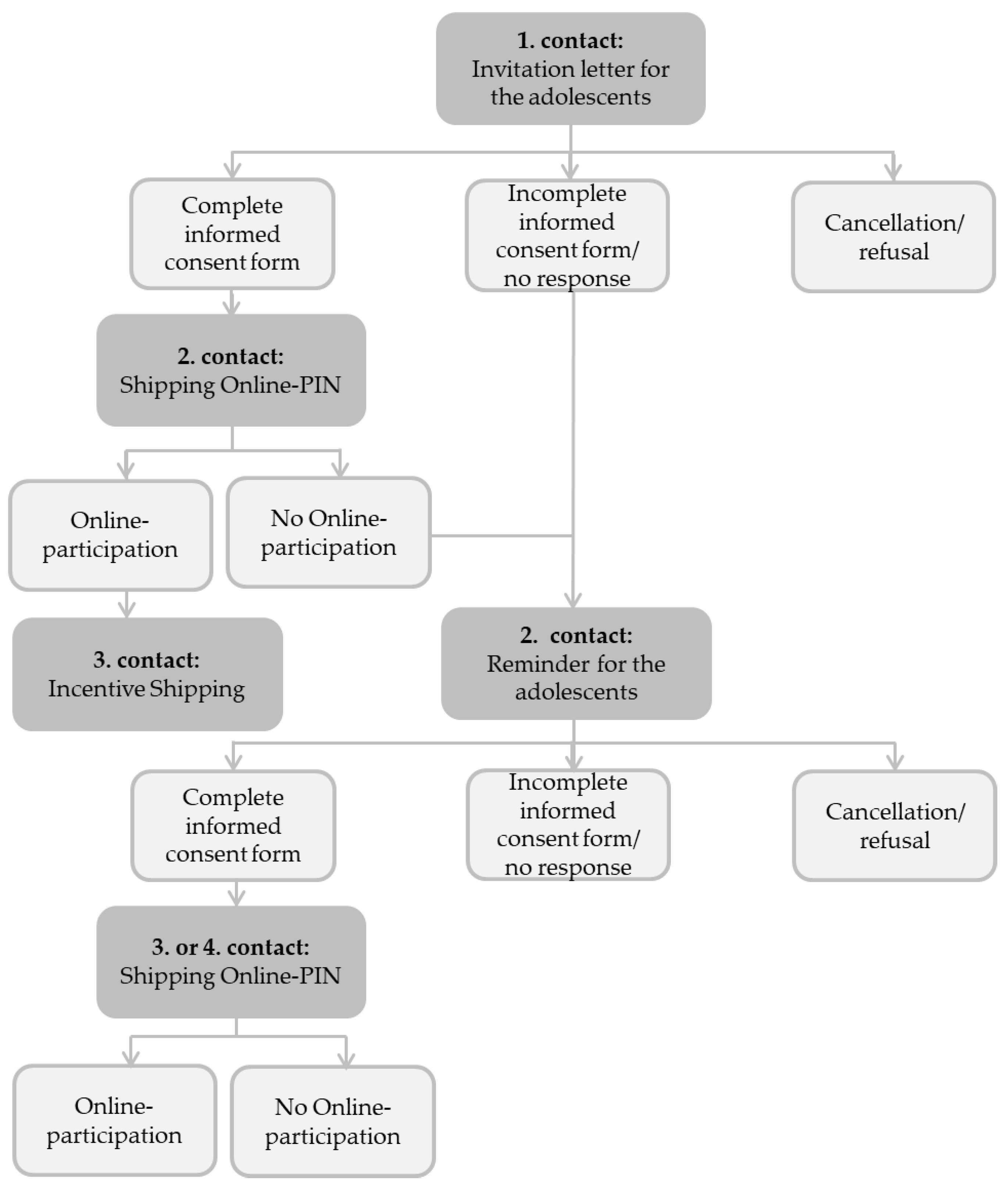
2.5. Data Collection & Data Handling
2.6. Measurements
2.7. Data Managament, Data Preparation and Data Analysis
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Van den Broucke, S. Health literacy: A critical concept for public health. Arch Public Health 2014, 72, 10. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Consortium Health Literacy Project European. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Jordan, S.; Hoebel, J. Health literacy of adults in Germany: Findings from the German Health Update (GEDA) study. Gesundheitskompetenz von Erwachsenen in Deutschland: Ergebnisse der Studie “Gesundheit in Deutschland aktuell” (GEDA). Bundesgesundheitsbl. Gesundh. Gesundh. 2015, 58, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Magnani, J.W.; Mujahid, M.S.; Aronow, H.D.; Cene, C.W.; Dickson, V.V.; Havranek, E.; Morgenstern, L.B.; Paasche-Orlow, M.K.; Pollak, A.; Willey, J.Z. Health Literacy and Cardiovascular Disease: Fundamental Relevance to Primary and Secondary Prevention: A Scientific Statement From the American Heart Association. Circulation 2018, 138, e48–e74. [Google Scholar] [CrossRef] [PubMed]
- Moser, D.K.; Robinson, S.; Biddle, M.J.; Pelter, M.M.; Nesbitt, T.S.; Southard, J.; Cooper, L.; Dracup, K. Health Literacy Predicts Morbidity and Mortality in Rural Patients With Heart Failure. J. Card Fail 2015, 21, 612–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bostock, S.; Steptoe, A. Association between low functional health literacy and mortality in older adults: Longitudinal cohort study. BMJ 2012, 344, e1602. [Google Scholar] [CrossRef] [Green Version]
- Berkman, N.; Sheridan, S.; Donahue, K.; Halpern, D.; Viera, A.; Crotty, K.; Holland, A.; Brasure, M.; Lohr, K.; Harden, E.; et al. Health Literacy Interventions and Outcomes: An Updated Systematic Review. Evidence Report/Technology Assesment No. 199. (Prepared by RTI International–University of North Carolina Evidence-Based Practice Center under Contract No. 290-2007-10056-I. AHRQ Publication Number 11-E006); Agency for Healthcare Research and Quality: Rockville, MD, USA, 2011. [Google Scholar]
- Garcia-Codina, O.; Juvinya-Canal, D.; Amil-Bujan, P.; Bertran-Noguer, C.; Gonzalez-Mestre, M.A.; Masachs-Fatjo, E.; Santaeugenia, S.J.; Magrinya-Rull, P.; Salto-Cerezuela, E. Determinants of health literacy in the general population: Results of the Catalan health survey. BMC Public Health 2019, 19, 1122. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for Europe (WHO Europe). Health Literacy. The Solid Facts. Available online: https://apps.who.int/iris/bitstream/handle/10665/128703/e96854.pdf (accessed on 17 November 2019).
- Mantwill, S.; Monestel-Umana, S.; Schulz, P.J. The Relationship between Health Literacy and Health Disparities: A Systematic Review. PLoS ONE 2015, 10, e0145455. [Google Scholar] [CrossRef] [Green Version]
- Chahardah-Cherik, S.M.; Gheibizadeh, M.P.; Jahani, S.P.; Cheraghian, B.P. The Relationship between Health Literacy and Health Promoting Behaviors in Patients with Type 2 Diabetes. Int. J. Community Based Nurs Midwifery 2018, 6, 65–75. [Google Scholar]
- Rom, K.M. Health Promotion for Children and Adolescents; Springer: Berlin/Heidelberg, Germany, 2016; ISBN 978-1-4899-7709-0. [Google Scholar]
- Borzekowski, D.L. Considering children and health literacy: A theoretical approach. Pediatrics 2009, 124 (Suppl. 3), S282–S288. [Google Scholar] [CrossRef]
- Bröder, J.; Okan, O.; Bauer, U.; Schlupp, S.; Pinheiro, P. Advancing perspectives on health literacy in childhood and youth. Health Promot. Int. 2019, 1–11. [Google Scholar] [CrossRef]
- Bundesministerium für Familie, Senioren, Frauen und Jugend. In Joint Responsibility: Policy for, with and by Youth. The Federal Government’s Youth Strategy. In Gemeinsamer Verantwortung: Politik für, mit und von Jugend. Die Jugendstrategie der Bundesregierung. Available online: https://www.bmfsfj.de/blob/141940/bfd79e3fc3acf5197251512ccec1d901/in-gemeinsamer-verantwortung-politik-fuer-mit-und-von-jugend-data.pdf (accessed on 10 December 2019).
- Bröder, J.; Okan, O.; Bauer, U.; Bruland, D.; Schlupp, S.; Bollweg, T.M.; Saboga-Nunes, L.; Bond, E.; Sorensen, K.; Bitzer, E.M.; et al. Health literacy in childhood and youth: A systematic review of definitions and models. BMC Public Health 2017, 17, 1–25. [Google Scholar] [CrossRef]
- Garcia, O.F.; Serra, E.; Zacares, J.J.; Calafat, A.; Garcia, F. Alcohol use and abuse and motivations for drinking and non-drinking among Spanish adolescents: Do we know enough when we know parenting style? Psychol. Health 2019, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, D.; Hurrelmann, K.; Bauer, U.; Kolpatzik, K.; Gille, S.; Vogt, D. National Action Plan Health Literacy: Need, Objective and Content. Der Nationale Aktionsplan Gesundheitskompetenz-Notwendigkeit, Ziel und Inhalt. Gesundheitswesen 2019, 81, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Manganello, J.A. Health literacy and adolescents: A framework and agenda for future research. Health Educ. Res. 2008, 23, 840–847. [Google Scholar] [CrossRef]
- Zamora, P.; Pinheiro, P.; Okan, O.; Bitzer, E.-M.; Jordan, S.; Bittlingmayer, U.H.; Kessl, F.; Lenz, A.; Wasem, J.; Jochimsen, M.A.; et al. “Health Literacy” in childhood and adolescence. Structure and objectives of a new German research consortium (HLCA Consortium). “Health Literacy” im Kindes- und Jugendalter. Struktur und Gegenstand eines neuen interdisziplinären Forschungsverbunds (HLCA-Forschungsverbund). Präv. Gesundh. 2015, 10, 167–172. [Google Scholar] [CrossRef]
- Okan, O.; Lopes, E.; Bollweg, T.M.; Bröder, J.; Messer, M.; Bruland, D.; Bond, E.; Carvalho, G.S.; Sørensen, K.; Saboga-Nunes, L.; et al. Generic health literacy measurement instruments for children and adolescents: A systematic review of the literature. BMC Public Health 2018, 18, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Arvanitis, M.; Davis, M.M.; Wolf, M.S. Topical Review: Proposing a Developmentally Informed Research Agenda for the Study of Health Literacy in Children. J. Pediatr. Psychol. 2019, 1–5. [Google Scholar] [CrossRef]
- Wallmann, B.; Gierschner, S.; Froböse, I. Health literacy: What do our students know about health? Gesundheitskompetenz: Was wissen unsere Schüler über Gesundheit? Präv. Gesundh. 2011, 7, 5–10. [Google Scholar] [CrossRef]
- Steckelberg, A.; Hülfenhaus, C.; Kasper, J.; Mühlhauser, I. Ebm@school—A curriculum of critical health literacy for secondary school students: Results of a pilot study. Int. J. Public Health 2009, 54, 158–165. [Google Scholar] [CrossRef]
- Steckelberg, A.; Hülfenhaus, C.; Kasper, J.; Rost, J.; Mühlhauser, I. How to measure critical health competences: Development and validation of the Critical Health Competence Test (CHC Test). Adv. Health Sci. Educ. 2009, 14, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, C.O.; Fahland, R.A.; Franze, M.; Splieth, C.; Thyrian, J.R.; Plachta-Danielzik, S.; Hoffmann, W.; Kohlmann, T. Health-related behavior, knowledge, attitudes, communication and social status in school children in Eastern Germany. Health Educ. Res. 2010, 25, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Berens, E.M.; Vogt, D.; Messer, M.; Hurrelmann, K.; Schaeffer, D. Health literacy among different age groups in Germany: Results of a cross-sectional survey. BMC Public Health 2016, 16, 1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quenzel, G.; Schaffer, D.; Messer, M.; Vogt, D. Health literacy among less well-educated young people: Influencing factors and consequences. Gesundheitskompetenz bildungsferner Jugendlicher: Einflussfaktoren und Folgen. Bundesgesundheitsbl. Gesundh. Gesundh. 2015, 58, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Richter, D.; Mehnert, A.; Forstmeyer, D.; Ernst, J.; Geue, K. Health Literacy in Adolescent and Young Adult Cancer Patients and Its Association with Health Outcomes. J. Adolesc. Young Adult Oncol. 2019, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Ohtake, P.; Childs, J. Why Publish Study Protocols? Phys. Ther. 2014, 94, 1208–1209. [Google Scholar] [CrossRef] [Green Version]
- Summerskill, W.; Collingridge, D.; Frankish, H. Protocols, probity, and publication. Lancet 2009, 373, 992. [Google Scholar] [CrossRef]
- Heim, R.; Konowalczyk, S.; Grgic, M.; Seyda, M.; Burrmann, U.; Rauschenbach, T. Can you do it with the mouse?-A methodological study on online surveys in youth research. Geht’s auch mit der Maus?–Eine Methodenstudie zu Online-Befragungen in der Jugendforschung. Z. Erzieh. 2016, 19, 783–805. [Google Scholar] [CrossRef]
- BIK Aschpurwis und Behrens GmbH. BIK Regions 2010. Available online: https://www.bik-gmbh.de/download/BIK-Regionen753_Methodenbeschreibung_lang.pdf (accessed on 27 November 2019).
- Saß, A.-C.; Grüne, B.; Brettschneider, A.-K.; Rommel, A.; Razum, O.; Ellert, U. Participation of people with migration background in health surveys of the Robert Koch Institute. Beteiligung von Menschen mit Migrationshintergrund an Gesundheitssurveys des Robert Koch-Instituts. Bundesgesundheitsbl. Gesundh. Gesundh. 2015, 58, 533–542. [Google Scholar] [CrossRef] [Green Version]
- Hölling, H.; Schlack, R.; Kamtsiuris, P.; Butschalowsky, H.; Schlaud, M.; Kurth, B.M. The KiGGS study. Nationwide representative longitudinal and cross-sectional study on the health of children and adolescents within the framework of health monitoring at the Robert Koch Institute. Die KiGGS-Studie. Bundesweit reprasentative Langs- und Querschnittstudie zur Gesundheit von Kindern und Jugendlichen im Rahmen des Gesundheitsmonitorings am Robert Koch-Institut. Bundesgesundheitsbl. Gesundh. Gesundh. 2012, 55, 836–842. [Google Scholar] [CrossRef]
- Kurth, B.M.; Kamtsiuris, P.; Hölling, H.; Mauz, E. Strategies of the Robert Koch Institute for monitoring the health of children and young people living in Germany. Strategien des Robert Koch-Instituts zum Monitoring der Gesundheit von in Deutschland lebenden Kindern und Jugendlichen. Kinder Jugendmed. 2016, 16, 176–183. [Google Scholar] [CrossRef]
- Mauz, E.; Gößwald, A.; Kamtsiuris, P.; Hoffmann, R.; Lange, M.; Schenck, U.V.; Allen, J.; Butschalowsky, H.; Frank, L.; Hölling, H.; et al. New data for action. Data collection for KiGGS Wave 2 has been completed. JoHM 2017, 2, 2–27. [Google Scholar] [CrossRef]
- Statistisches Bundesamt (DESTATIS). Population and employment. Population with Migration Background. Results of the Microcensus 2018. Bevölkerung und Erwerbstätigkeit. Bevölkerung mit Migrationshintergrund. Ergebnisse des Mikrozensus 2018. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Migration-Integration/Publikationen/Downloads-Migration/migrationshintergrund-2010220187004.pdf?__blob=publicationFile (accessed on 2 December 2019).
- Domanska, O.; Bollweg, T.M.; Loer, A.-K.; Holmberg, C.; Schenk, L.; Jordan, S. Development and psychometric properties of a questionnaire assessing self-reported generic ehalth literacy in adolescence. Int. J. Environ. Res. Public Health. submitted.
- European Commission. Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the Protection of Natural Persons with Regard to the Processing of Personal Data and on the free Movement of Such Data, and Repealing Directive 95/46/EC (General Data Protection Regulation) (Text with EEA relevance). Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32016R0679 (accessed on 24 November 2019).
- Robert Koch-Institut. German Health Update (GEDA19-EHIS). [Gesundheit in Deutschland Aktuell (GEDA19-EHIS)]. Available online: https://www.geda-studie.de/gesundheitsstudie/geda-2019-ehis.html (accessed on 9 December 2019).
- Hartley, J.E.; Levin, K.; Currie, C. A new version of the HBSC Family Affluence Scale-FAS III: Scottish Qualitative Findings from the International FAS Development Study. Child Indic. Res. 2016, 9, 233–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adler, N.E.; Epel, E.S.; Castellazzo, G.; Ickovics, J.R. Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy white women. Health Psychol. 2000, 19, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Lampert, T.; Höbel, J.; Kuntz, B.; Müters, S.; Kroll, L.E. Socioeconomic status and subjective social status measurement in KiGGS Wave 2. JoHM 2018, 3, 108–125. [Google Scholar] [CrossRef]
- Bildungsinstitut Bildungsforschung (BIFIE). Materials. PISA 2015. Student Questionnaire. [Materialien. PISA 2015. Schülerfragebogen]. Available online: https://www.bifie.at/wp-content/uploads/2017/04/Schuelerfragebogen.pdf (accessed on 7 December 2019).
- Schumann, M.; Kajikhina, K.; Polizzi, A.; Sarma, N.; Hoebel, J.; Bug, M.; Bartig, S.; Lampert, T.; Santos-Hövener, C. Concepts for migration-sensitive health monitoring. JoHM 2019, 4, 49–65. [Google Scholar] [CrossRef]
- Firnges, C.; Domanska, O.; Jordan, S. Developing an instrument for measuring the health literacy of adolescents: Lessons learned. In International Handbook of Health Literacy. Research, Practice and Policy across the Lifespan; Okan, O., Bauer, U., Levin-Zamir, D., Pinheiro, P., Sørensen, K., Eds.; Policy Press University of Bristol: Britain, UK, 2019; pp. 99–114. ISBN 978-1447344513. [Google Scholar]
- Ghanbari, S.; Ramezankhani, A.; Montazeri, A.; Mehrabi, Y. Health Literacy Measure for Adolescents (HELMA): Development and Psychometric Properties. PLoS ONE 2016, 11, e0149202. [Google Scholar] [CrossRef] [Green Version]
- Wartella, E.; Rideout, V.; Montague, H.; Beaudoin-Ryan, L.; Lauricella, A. Teens, Health and Technology: A National Survey. Media Commun. 2016, 4, 13–23. [Google Scholar] [CrossRef]
- Bradley, K.A.; McDonell, M.B.; Bush, K.; Kivlahan, D.R.; Diehr, P.; Fihn, S.D. The AUDIT alcohol consumption questions: Reliability, validity, and responsiveness to change in older male primary care patients. Alcohol. Clin. Exp. Res. 1998, 22, 1842–1849. [Google Scholar] [CrossRef]
- Bush, K.; Kivlahan, D.R.; McDonell, M.B.; Fihn, S.D.; Bradley, K.A. The AUDIT alcohol consumption questions (AUDIT-C): An effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch. Intern. Med. 1998, 158, 1789–1795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mensink, G.; Schienkiewitz, A.; Lange, C. Vegetable consumption among adults in Germany. JoHM 2017, 50–56. [Google Scholar] [CrossRef]
- Mensink, G.; Schienkiewitz, A.; Lange, C. Fruit consumption among adults in Germany. JoHM 2017, 43–49. [Google Scholar] [CrossRef]
- Schwarzer, R.; Jerusalem, M.H. Scales for Recording Teacher and Student Characteristics. Documentation of the Psychometric Procedures within the Framework of the Scientific Monitoring of the Pilot Project Self-Effective Schools; [Skalen zur Erfassung von Lehrer-und Schülermerkmalen: Dokumentation der psychometrischen Verfahrenim Rahmen der Wissenschaftlichen Begleitung des Modellversuchs Selbstwirksame Schulen]; Freie Universität Berlin: Berlin, Germany, 1999; ISBN 3-00-003708-X. [Google Scholar]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Pers. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Zimet, G.D.; Powell, S.S.; Farley, G.K.; Werkman, S.; Berkoff, K.A. Psychometric characteristics of the Multidimensional Scale of Perceived Social Support. J. Pers. Assess. 1990, 55, 610–617. [Google Scholar] [CrossRef]
- HLS-EU Consortium. Comparative Report on Health Literacy in Eight EU Members States. The European Health Literacy Survey HLS-EU (Second Reviesed and Extended Version, Date 22 July 2014). Available online: https://cdn1.sph.harvard.edu/wp-content/uploads/sites/135/2015/09/neu_rev_hls-eu_report_2015_05_13_lit.pdf (accessed on 3 December 2019).
- American Association for Public Opinion Research (AAPOR). Standard Definitions. Final Dispositions of Case Codes and Outcome Rates for Surveys. Available online: https://www.aapor.org/AAPOR_Main/media/publications/Standard-Definitions20169theditionfinal.pdf (accessed on 3 December 2019).
- McCormack, L.; Haun, J.; Sorensen, K.; Valerio, M. Recommendations for advancing health literacy measurement. J. Health Commun. 2013, 18 (Suppl. 1), 9–14. [Google Scholar] [CrossRef] [Green Version]
- Schaeffer, D.; Hurrelmann, K.; Bauer, U.; Kolpatzik, K.H. National Action Plan Health Literacy [Nationaler Aktionsplan Gesundheitskompetenz. Die Gesundheitskompetenz in Deutschland stärken]; KomPart: Berlin, Germany, 2018. [Google Scholar]
- Salkind, N.J. Encyclopedia of Research Design; Sage: Newcastle, UK, 2010. [Google Scholar] [CrossRef]
- Walter, U.; Liersch, S.; Gerlich, M.G.; Raithel, J.; Barnekow, V. The life phase of adolescence and young adults-social and age-specific challenges to promote health. [Die Lebensphase Adoleszenz und junge Erwachsene–gesellschaftliche und altersspezifische Herausforderungen zur Förderung der Gesundheit]. In Gesund jung?!: Herausforderung für die Prävention und Gesundheitsförderung bei Jugendlichen und Jungen Erwachsenen; Springer: Berlin/Heidelberg, Germany, 2011; pp. 3–30. ISBN 978-3-642-16710-2. [Google Scholar]
- Secretariat of the Standing Conference of the Ministers of Education and Cultural Affairs of the Länder in the Federal Republic of Germany. The Education System in the Federal Republic of Germany 2015/2016. A Description of the Responsibilities, Structures and Developments in Education Policy for the Exchange of Information in Europe. Available online: https://www.kmk.org/fileadmin/Dateien/pdf/Eurydice/Bildungswesen-engl-pdfs/dossier_en_ebook.pdf (accessed on 29 November 2019).
- Schenk, L.; Ellert, U.; Neuhauser, H. Children and young people with a migration background in Germany. [Kinder und Jugendliche mit Migrationshintergrund in Deutschland.]. Bundesgesundheitsbl. Gesundh. Gesundh. 2007, 50, 590–599. [Google Scholar] [CrossRef]
- Frank, L.; Yesil-Jürgens, R.; Born, S.; Hoffmann, R.; Santos-Hövener, C.; Lampert, T. Improving the inclusion and participation of children and adolescents with a migration background in KiGGS Wave 2. JoHM 2018, 3, 126–142. [Google Scholar] [CrossRef]
- Lohr, S.L. Sampling: Design and Analysis, 2nd ed.; Brooks/Cole: Boston, MA, USA, 2010; ISBN 0495105279. [Google Scholar]
- Koch, A.; Blohm, M. Nonresponse Bias. Available online: https://www.gesis.org/fileadmin/upload/SDMwiki/Nonresponse_Bias_Koch_Blohm_08102015_1.1.pdf (accessed on 4 December 2019).



{kind=link}
{kind=link}
| Topic/Parameter | Measures | Indication of Source | Number of Items | Used for Analyzing Follwing Objectives * |
|---|---|---|---|---|
| Socio-demographics | Year and month of birth | Study KiGGS 2 [37] | 1 | 1, 2, 3 |
| Sex (stated in the birth certificate) | Study “German Health Update” (GEDA19-EHIS) [41] | 1 | ||
| Gender (subjective belonging) | Study GEDA19-EHIS [41] | 1 | ||
| Education | School attendence | Study KiGGS 2 [37] | 1 | 1, 2, 3 |
| Type of school | Study KiGGS 2, slightly adapted [37] | 1 | ||
| Achieved school certificate on the secondary level | Study KiGGS 2 [37] | 1 | ||
| Socio-economic status of family | Social Family Affluance Scale | Study “Health Behavior in School-aged Children” (HBSC) [42] | 6 | 1, 2, 3 |
| Subjective social status (German version of MacArthur Scale) | Study KiGGS 2 [43,44] | 1 | ||
| cultural capital through the number of books in the household | Survey PISA 2015 [45] | 1 | ||
| Immigration background | Respondent’s country of origin | Study KiGGS 2 [37] | 1 | 1, 2, 3 |
| Mother’s country of origin | Study KiGGS 2 [37] | 1 | ||
| Father’s country of origin | Study KiGGS 2 [37] | 1 | ||
| Length of stay in Germany | Study KiGGS 2 [37] | 1 | ||
| Self-reported language skills | Native language | Project “Improving Health Monitoring in Migrant Populations” (IMIRA) [46] | 1 | 1 |
| Self-rated German skills | Project IMIRA [46] | 1 | ||
| Self-rated native language skills | Project IMIRA [46] | 1 | ||
| Generic health literacy | Measurement of Health Literacy Among Adolescents- Questionnaire (MOHLAA-Q) | Study MOHLAA [39,47] | 29 | 1, 2, 3 |
| Reading comprehension and numeracy | Health Literacy Measure for Adolescents (HELMA) | Measurement HELMA, adapted [48] | 3 | 1, 2, 3 |
| Health literacy seeking behavior | Sources and quantity of received health literacy information | Survey “Teens, Health and Technology: a national survey”, adapted [49] | 14 | 1, 2, 3 |
| Health-related behavior | Alcohol: harmful and binge drinking (Alcohol Use Disorders Identification Test, AUDIT-C) | Study KiGGS 2 [37,50,51] | 4 | 3 |
| Smoking tabbaco use | Study KiGGS 2 [37] | 2 | ||
| Physical activity (sport) | Study KiGGS 2 [37] | 1 | ||
| Keeping safety rules | Study KiGGS 2 [37] | 4 | ||
| Nutrition (fruits and vegetables consumption) | Study GEDA 2014/2015 [52,53], slightly adapted | 4 | ||
| Social and personal resources | Self-efficacy scale (Scale of General Self-efficacy) | Study KiGGS 2 [54] | 10 | 2, 3 |
| Social support (the Multidimensional Scale of Perceived Social Support) | Study HBSC [55,56] | 8 | ||
| Health status | Subjective health status | Study KiGGS 2 [37] | 1 | 3 |
| Anthropometry | Self-reported height | Study KiGGS 2 [37] | 1 | 3 |
| Self-reported weight | Study KiGGS 2 [37] | 1 | ||
| Utilisation of health services | Utilisation of doctor visits in the last 12 months | Survey “The European Health Literacy Survey” (HLS-EU), adapted [57] | 1 | 3 |
| Utilisation of hospitals in the last 12 months | Study KiGGS [35,36] | 1 | ||
| Utilisation of ambulances in the last 12 months | Study KiGGS [35,36] | 1 | ||
| Total number | 106 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loer, A.-K.M.; Domanska, O.M.; Kuhnert, R.; Houben, R.; Albrecht, S.; Jordan, S. Online Survey for the Assessment of Generic Health Literacy among Adolescents in Germany (GeKoJu): Study Protocol. Int. J. Environ. Res. Public Health 2020, 17, 1518. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051518
Loer A-KM, Domanska OM, Kuhnert R, Houben R, Albrecht S, Jordan S. Online Survey for the Assessment of Generic Health Literacy among Adolescents in Germany (GeKoJu): Study Protocol. International Journal of Environmental Research and Public Health. 2020; 17(5):1518. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051518
Chicago/Turabian StyleLoer, Anne-Kathrin M., Olga Maria Domanska, Ronny Kuhnert, Robin Houben, Stefan Albrecht, and Susanne Jordan. 2020. "Online Survey for the Assessment of Generic Health Literacy among Adolescents in Germany (GeKoJu): Study Protocol" International Journal of Environmental Research and Public Health 17, no. 5: 1518. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051518