The Development and Exploratory Psychometric Properties of the Traumatic and Routine Stressors Scale on Emergency Nurses (TRSS-EN)

Abstract
:1. Introduction
Background
2. Materials and Methods
2.1. Ethical Approval
2.2. Design
2.3. Participants and Procedure
2.4. Instruments
2.4.1. The Spanish Version of the Symptom Assessment-45 Questionnaire (SA-45)
2.4.2. The Posttraumatic Diagnostic Scale for DMS-5 (PDS-5)
2.4.3. Traumatic and Routine Stressors Scale on Emergency Nurses (TRSS-EN)
2.5. Analysis
Psychometric Analysis of TRSS-EN
3. Results
3.1. Descriptive Analysis and Internal Consistency
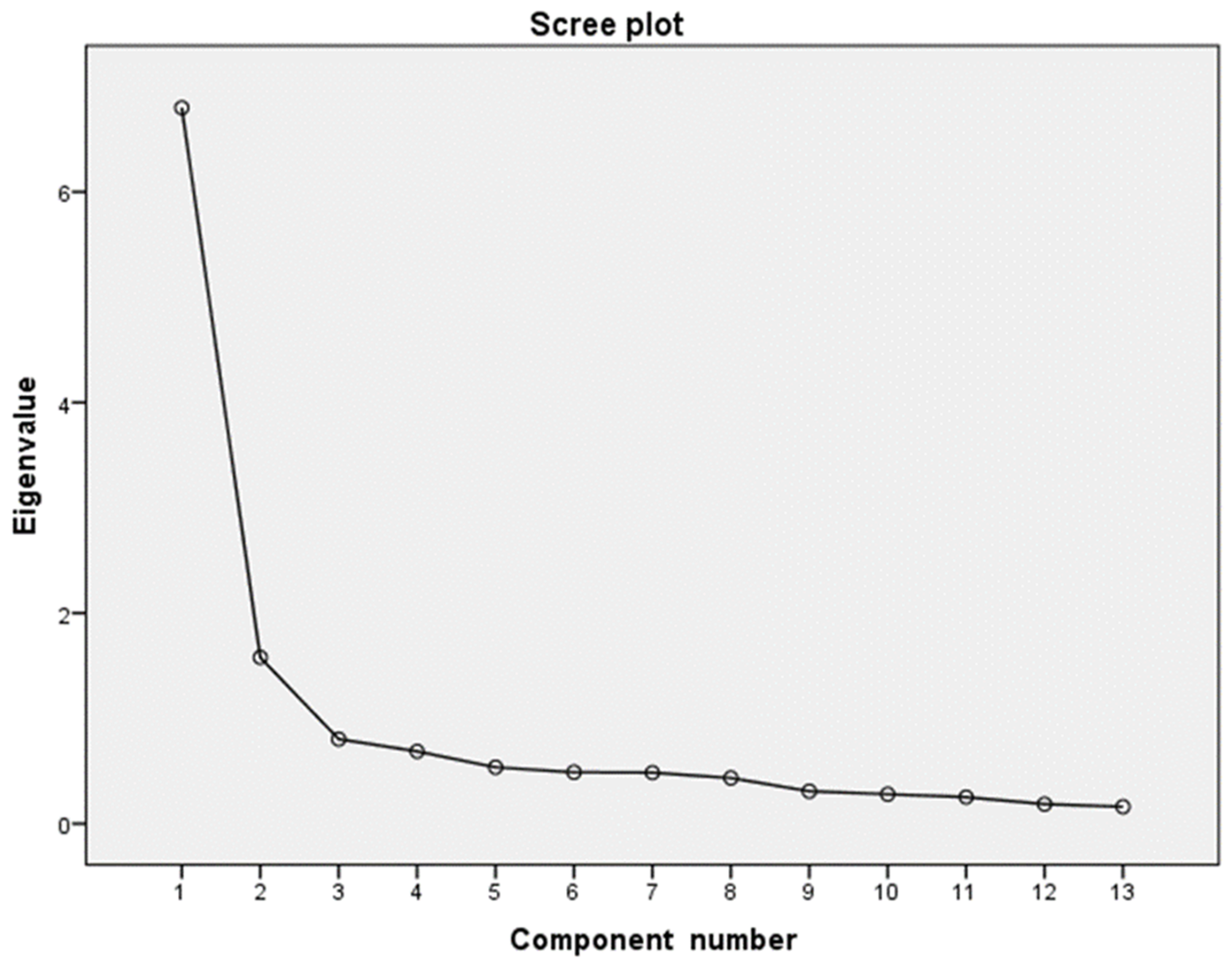
3.2. Exploratory Factor Analysis
3.3. Validity Assessments
3.4. Test–retest
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Adriaenssens, J.; de Gucht, V.; Maes, S. The impact of traumatic events on emergency room nurses: Findings from a questionnaire survey. Int. J. Nurs. Stud. 2012, 49, 1411–1422. [Google Scholar] [CrossRef]
- Laposa, J.M.; Alden, L.E.; Fullerton, L.M. Work stress and posttraumatic stress disorder in ED nurses/personnel (CE). J. Emerg. Nurs. 2003, 29, 23–28. [Google Scholar] [CrossRef]
- Somville, F.J.; De Gucht, V.; Maes, S. The impact of occupational hazards and traumatic events among Belgian emergency physicians. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 59. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Arlington, TX, USA, 2013. [Google Scholar]
- World Health Organization. ICD-11 for Mortality and Morbidity Statistics (ICD-11 MMS) 2019 Version. Available online: https://icd.who.int/browse11/l-m/en (accessed on 17 March 2020).
- Liberman, A.M.; Best, S.; Metzler, T.J.; Fagan, J.A.; Weiss, D.S.; Marmar, C.R. Routine occupational stress and psychological distress in police. Polic. Int. J. Police Strateg. Manag. 2002, 25, 421–441. [Google Scholar] [CrossRef]
- Violanti, J.M.; Ma, C.C.; Mnatsakanova, A.; Fekedulegn, D.; Hartley, T.A.; Gu, J.K.; Andrew, M.E. Associations between Police Work Stressors and Posttraumatic Stress Disorder Symptoms: Examining the Moderating Effects of Coping. J. Police Crim. Psychol. 2018, 33, 271–282. [Google Scholar] [CrossRef]
- Friedman, M.J.; Resick, P.A.; Keane, T.M. PTSD: Twenty-five years of progress and challenges. In Handbook of PTSD: Science and Practice; Friedman, M.J., Keane, T.M., Resick, P.A., Eds.; Guilford Press: New York, NY, USA, 2007; pp. 3–18. [Google Scholar]
- Bullman, T.A.; Kang, H.K.; Thomas, T.L. Posttraumatic stress disorder among Vietnam veterans on the agent orange registry a case-control analysis. Ann. Epidemiol. 1991, 1, 505–512. [Google Scholar] [CrossRef]
- Basoglu, M.; Paker, M. Severity of trauma as predictor of long-term psychological status in survivors of torture. J. Anxiety Disord. 1995, 9, 339–350. [Google Scholar] [CrossRef]
- Declercq, F.; Meganck, R.; Deheegher, J.; Van Hoorde, H. Frequency of and subjective response to critical incidents in the prediction of PTSD in emergency personnel. J. Trauma. Stress 2011, 24, 133–136. [Google Scholar] [CrossRef]
- Eisenbarth, H.; Godinez, D.; du Pont, A.; Corley, R.P.; Stallings, M.C.; Rhee, S.H. The influence of stressful life events, psychopathy, and their interaction on internalizing and externalizing psychopathology. Psychiatry Res. 2019, 272, 438–446. [Google Scholar] [CrossRef]
- Hammen, C. Stress and depression. Annu. Rev. Clin. Psychol. 2005, 1, 293–319. [Google Scholar] [CrossRef] [Green Version]
- Arul, A.S.S.J. Study of life events and personality dimensions in generalized anxiety disorder. J. Clin. Diagn. Res. 2016, 10, VC05–VC09. [Google Scholar] [CrossRef]
- Van Hooff, M.; McFarlane, A.C.; Baur, J.; Abraham, M.; Barnes, D.J. The stressor criterion-A1 and PTSD: A matter of opinion? J. Anxiety Disord. 2009, 23, 77–86. [Google Scholar] [CrossRef]
- Mol, S.S.L.; Arntz, A.; Metsemakers, J.F.M.; Dinant, G.J.; Vilters-Van Montfort, P.A.P.; Knottnerus, J.A. Symptoms of post-traumatic stress disorder after non-traumatic events: Evidence from an open population study. Br. J. Psychiatry 2005, 186, 494–499. [Google Scholar] [CrossRef]
- Gold, S.D.; Marx, B.P.; Soler-Baillo, J.M.; Sloan, D.M. Is life stress more traumatic than traumatic stress? J. Anxiety Disord. 2005, 19, 687–698. [Google Scholar] [CrossRef]
- Stathopoulou, H.; Karanikola, M.N.K.; Panagiotopoulou, F.; Papathanassoglou, E.D.E. Anxiety Levels and Related Symptoms in Emergency Nursing Personnel in Greece. J. Emerg. Nurs. 2011, 37, 314–320. [Google Scholar] [CrossRef]
- Mealer, M.L.; Shelton, A.; Berg, B.; Rothbaum, B.; Moss, M. Increased prevalence of post-traumatic stress disorder symptoms in critical care nurses. Am. J. Respir. Crit. Care Med. 2007, 175, 693–697. [Google Scholar] [CrossRef]
- Maia, Â.C.; Ribeiro, E. The psychological impact of motor vehicle accidents on emergency service workers. Eur. J. Emerg. Med. 2010, 17, 296–301. [Google Scholar] [CrossRef]
- Antelman, S. Time-dependent sensitization as the cornerstone for a new approach to pharmacotherapy: Drugs as foreign/stressful stimuli. Drug Dev. Res. 1988, 14, 1–30. [Google Scholar] [CrossRef]
- Eisenstein, E.M.; Eisenstein, D.; Smith, J.C. The Evolutionary Significance of Habituation and Sensitization Across Phylogeny: A Behavioral Homeostasis Model. Integr. Physiol. Behav. Sci. 2001, 36, 251–265. [Google Scholar] [CrossRef]
- O’Connor, J.; Jeavons, S. Nurses’ perceptions of critical incidents. J. Adv. Nurs. 2003, 41, 53–62. [Google Scholar] [CrossRef]
- Levy-Gigi, E.; Bonanno, G.A.; Shapiro, A.R.; Richter-Levin, G.; Kéri, S.; Sheppes, G. Emotion regulatory flexibility sheds light on the elusive relationship between repeated traumatic exposure and posttraumatic stress disorder symptoms. Clin. Psychol. Sci. 2016, 4, 28–39. [Google Scholar] [CrossRef] [Green Version]
- Holland, M. The dangers of detrimental coping in emergency medical services. Prehosp. Emerg. Care 2011, 15, 331–337. [Google Scholar] [CrossRef]
- Bianchi, E.R.F. Escala Bianchi de Stress. Rev. Esc. Enferm. USP 2009, 43, 1055–1062. [Google Scholar] [CrossRef]
- Gray-Toft, P.; Anderson, J.G. The Nursing Stress Scale: Development of an instrument. J. Behav. Assess. 1981, 3, 11–23. [Google Scholar] [CrossRef]
- Yang, P. Development of a Career Stress Scale for Hospital Nurses: Implications for Workplace Counseling. J. Employ. Couns. 2017, 54, 156–167. [Google Scholar] [CrossRef]
- French, J.R.P., Jr.; Caplan, R.D.; Harrison, R.V. The Mechanisms of Job Stress and Strain; Wiley: London, UK, 1982. [Google Scholar]
- Yuwanich, N.; Akhavan, S.; Nantsupawat, W.; Martin, L.; Elfström, M.L.; Sandborgh, M. Development and psychometric properties of the stressor scale for emergency nurses. Int. Emerg. Nurs. 2018, 39, 77–88. [Google Scholar] [CrossRef]
- World Medical Association. Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects. 2013. Available online: http://www.wma.net/en/30publications/10policies/b3/index.html (accessed on 20 January 2018).
- Sandín, B.; Valiente, R.M.; Chorot, P.; Santed, M.A.; Lostao, L. SA-45: A brief form of the SCL-90. Psicothema 2008, 20, 290–296. [Google Scholar]
- Davison, M.L.; Bershadsky, B.; Bieber, J.; Silversmith, D.; Maruish, M.E.; Kane, R.L. Development of a brief, multidimensional, self-report instrument for treatment outcomes assessment in psychiatric settings: Preliminary findings. Assessment 1997, 4, 259–276. [Google Scholar] [CrossRef]
- Derogatis, L.R. BSI: Brief Symptom Inventory; National Computer Systems: Minneapolis, MN, USA, 1993; pp. 32–40. [Google Scholar]
- Foa, E.B.; McLean, C.P.; Zang, Y.; Zhong, J.; Powers, M.B.; Kauffman, B.Y.; Rauch, S.; Porter, K.; Knowles, K. Psychometric properties of the posttraumatic diagnostic scale for DSM-5 (PDS-5). Psychol. Assess. 2016, 28, 1166–1171. [Google Scholar] [CrossRef]
- Minnie, L.; Goodman, S.; Wallis, L. Exposure to daily trauma: The experiences and coping mechanism of Emergency Medical Personnel. A cross-sectional study. Afr. J. Emerg. Med. 2015, 5, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Cattell, R.B. The scree test for the number of factors. Multivar. Behav. Res. 1966, 1, 245–276. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data Data for Categorical of Observer Agreement the Measurement. Int. Biom. Soc. 1977, 33, 159–174. [Google Scholar]
- McGraw, K.O.; Wong, S.P. Forming Inferences about Some Intraclass Correlation Coefficients. Psychol. Methods 1996, 1, 30–46. [Google Scholar] [CrossRef]
- Nunnally, J.; Bernstein, I. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Farhood, L.; Dimassi, H.; Lehtinen, T. Exposure to War-Related Traumatic Events, Prevalence of PTSD, and General Psychiatric Morbidity in a Civilian Population from Southern Lebanon. J. Transcult. Nurs. 2006, 17, 333–340. [Google Scholar] [CrossRef]
- Husain, F.; Anderson, M.; Lopes Cardozo, B.; Becknell, K.; Blanton, C.; Araki, D.; Kottegoda Vithana, E. Prevalence of war-related mental health conditions and association with displacement status in postwar Jaffna District, Sri Lanka. JAMA-J. Am. Med. Assoc. 2011, 306, 522–531. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Descriptive Data | Mean | SD | n | Percentage |
|---|---|---|---|---|
| Age (N = 144) | 40.41 | 8.32 | ||
| Children (N = 147) | 0.99 | 1.02 | ||
| Years of experience in the profession (N = 147) | 16.48 | 7.33 | ||
| Years of experience in the same job (N = 147) | 9.9 | 6.69 | ||
| Characteristics | ||||
| Gender | 147 | 100 | ||
| Male | 19 | 12.9 | ||
| Female | 128 | 87.1 | ||
| Marital status | 145 | 100 | ||
| With regular partner | 115 | 79.3 | ||
| Single | 30 | 20.7 | ||
| Studies | 146 | 100 | ||
| DUE | 88 | 60.3 | ||
| General Nurse | 11 | 7,5 | ||
| TCAE | 43 | 29.5 | ||
| Others | 4 | 2,7 | ||
| Employment situation | 147 | 100 | ||
| Permanent | 72 | 49 | ||
| Non-permanent | 75 | 51 | ||
| Percentage with patients | 146 | 100 | ||
| Less than 25% | 8 | 5.5 | ||
| From 25% to 50% | 2 | 1.4 | ||
| From 50% to 75% | 25 | 17.1 | ||
| More than 75% | 111 | 76 |
| Item | Statement | Mean | SD | S | K | IH | Alpha |
|---|---|---|---|---|---|---|---|
| TRSS-EN_1 | Dealing with sudden death of young persons | 4.27 | 1.67 | −0.20 | −0.75 | 0.39 | 0.78 |
| TRSS-EN_2 | Dealing with death or resuscitation of a baby or young child | 4.68 | 1.62 | −0.45 | −0.50 | 0.41 | 0.78 |
| TRSS-EN_3 | Handling victims of car and train crashes | 4.34 | 1.55 | −0.35 | −0.48 | 0.57 | 0.76 |
| TRSS-EN_4 | Confrontation with physical trauma and burns patients | 4.06 | 1.74 | −0.35 | −0.83 | 0.49 | 0.77 |
| TRSS-EN_5 | Dealing with suicide | 3.86 | 1.60 | −0.01 | −0.51 | 0.44 | 0.78 |
| TRSS-EN_6 | Dealing with aggression, violence and threat | 3.26 | 1.43 | 0.18 | −0.45 | 0.57 | 0.77 |
| TRSS-EN_7 | Inability to deliver good quality of care | 3.55 | 1.62 | 0.04 | −0.66 | 0.41 | 0.78 |
| TRSS-EN_8 | Inability to help chronically ill patients | 3.90 | 1.57 | −0.02 | −0.59 | 0.50 | 0.77 |
| TRSS-EN_9 | Dealing with relatives of victims/patients | 5.09 | 2.00 | −0.89 | −0.42 | 0.24 | 0.79 |
| TRSS-EN_10 | Confrontation with child abuse and negligence | 4.00 | 1.46 | 0.14 | −0.20 | 0.52 | 0.77 |
| TRSS-EN_11 | Exposure to sudden death | 5.09 | 2.15 | −0.87 | −0.66 | 0.11 | 0.80 |
| TRSS-EN_12 | Dealing with psychiatric patients | 4.97 | 1.92 | −0.75 | −0.57 | 0.40 | 0.79 |
| TRSS-EN_13 | Management of dead bodies | 3.82 | 1.62 | 0.19 | −0.77 | 0.43 | 0.78 |
| Components | Communalities | |||
|---|---|---|---|---|
| Item | Statement | TS | RS | |
| TRSS-EN_1 | Dealing with sudden death of young persons | 0.704 | 0.325 | 0.602 |
| TRSS-EN_2 | Dealing with death or resuscitation of a baby or young child | 0.846 | 0.101 | 0.726 |
| TRSS-EN_3 | Handling victims of car and train crashes | 0.686 | 0.372 | 0.609 |
| TRSS-EN_4 | Confrontation with physical trauma and burns patients | 0.682 | 0.455 | 0.673 |
| TRSS-EN_5 | Dealing with suicide | 0.725 | 0.300 | 0.617 |
| TRSS-EN_6 | Dealing with aggression, violence and threat | 0.559 | 0.562 | 0.628 |
| TRSS-EN_7 | Inability to deliver good quality of care | 0.212 | 0.819 | 0.715 |
| TRSS-EN_8 | Inability to help chronically ill patients | 0.169 | 0.803 | 0.673 |
| TRSS-EN_9 | Dealing with relatives of victims/patients | 0.270 | 0.767 | 0.661 |
| TRSS-EN_10 | Confrontation with child abuse and negligence | 0.828 | 0.144 | 0.707 |
| TRSS-EN_11 | Exposure to sudden death | 0.835 | 0.249 | 0.759 |
| TRSS-EN_12 | Dealing with psychiatric patients | 0.196 | 0.712 | 0.546 |
| TRSS-EN_13 | Management of dead bodies | 0.283 | 0.620 | 0.464 |
| % explained variance | 35.63 | 28.81 | ||
| Cronbach alpha Omega | 0.911 0.857 | 0.862 0.833 | ||
| Emotional Impact | Frequency | Total Impact | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | TS | RS | Steiger’s Z | TS | RS | Steiger’s Z | TS | RS | Steiger’s Z | |
| Psychopathological symptoms (SA-45) | 31.29 | 24.34 | 0.14 | 0.30 ** | −2.44 * | 0.17 * | 0.22 ** | −0.61 | 0.21 * | 0.35 ** | −2.05 * |
| Hostility | 0.47 | 0.62 | 0.16 | 0.21 ** | −0.78 | 0.14 | 0.16 | −0.17 | 0.23 ** | 0.26 ** | −0.52 |
| Somatization | 1.09 | 0.87 | 0.12 | 0.23 ** | −1.59 | 0.05 | 0.12 | −0.86 | 0.05 | 0.21 * | −2.23 * |
| Depression | 0.84 | 0.75 | 0.04 | 0.24 ** | −2.82 ** | 0.14 | 0.22 ** | −1.82 | 0.13 | 0.31 ** | −2.50 * |
| Obsessive−compulsive | 0.93 | 0.77 | 0.20 * | 0.31 ** | −1.68 | 0.11 | 0.15 | −0.49 | 0.21 * | 0.30 ** | −1.33 |
| Anxiety | 0.86 | 0.70 | 0.19 * | 0.30 ** | −1.59 | 0.18 * | 0.22 ** | −0.39 | 0.26 ** | 0.33 ** | −1.01 |
| Interpersonal sensitivity | 0.82 | 0.79 | 0.08 | 0.26 ** | −2.53 * | 0.20 * | 0.23 ** | −0.31 | 0.19 * | 0.32 ** | −1.88 |
| Phobic anxiety | 0.25 | 0.46 | 0.00 | 0.13 | −1.76 | 0.06 | 0.04 | 0.26 | 0.08 | 0.13 | −0.80 |
| Paranoid ideation | 0.75 | 0.65 | 0.04 | 0.24 ** | −2.79 ** | 0.21 ** | 0.22 ** | −0.04 | 0.15 | 0.29 ** | −2.05 * |
| Psychoticism | 0.25 | 0.42 | 0.13 | 0.25 ** | −1.78 | 0.17 * | 0.27 ** | −1.17 | 0.25 ** | 0.37 ** | −1.70 |
| Symptoms of PTSD (PDS−5) | 12.77 | 13.40 | 0.13 | 0.31 ** | −2.55 * | 0.08 | 0.10 | −0.17 | 0.14 | 0.19 | 0.43 |
| Intrusion | 3.58 | 3.68 | 0.08 | 0.27 ** | −2.74 ** | 0.12 | 0.07 | 0.81 | 0.18 | 0.16 | 0.30 |
| Avoidance | 1.52 | 1.68 | 0.19 | 0.31 ** | −1.87 | 0.05 | 0.10 | −0.60 | 0.13 | 0.18 | −0.73 |
| Changes in mood and cognition | 3.62 | 4.76 | 0.04 | 0.23 * | −2.78 ** | 0.07 | 0.13 | −0.69 | 0.06 | 0.17 | −1.58 |
| Arousal and hyperreactivity | 4.04 | 4.78 | 0.20* | 0.31 ** | −1.54 | 0.05 | 0.07 | −0.18 | 0.14 | 0.19 | −0.59 |
| Impact | Frequency | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Test | Retest | Test | Retest | |||||||||
| Mean | SD | Mean | SD | t | CCI | Mean | SD | Mean | SD | t | CCI | |
| 1 | 4.80 | 1.60 | 4.95 | 1.64 | −0.67 | 0.63 | 1.72 | 0.96 | 1.92 | 0.97 | −1.27 | 0.47 |
| 2 | 4.48 | 2.25 | 5.40 | 2.06 | −2.40 * | 0.75 | 1.19 | 0.62 | 1.08 | 0.36 | 1.67 | 0.69 |
| 3 | 3.80 | 1.57 | 3.97 | 1.51 | −0.75 | 0.55 | 3.35 | 2.20 | 3.15 | 1.95 | 0.82 | 0.73 |
| 4 | 3.77 | 1.64 | 3.95 | 1.58 | −0.76 | 0.60 | 2.52 | 1.66 | 2.75 | 1.53 | −1.00 | 0.60 |
| 5 | 4.20 | 1.87 | 4.54 | 1.73 | −1.27 | 0.58 | 2.23 | 1.51 | 2.41 | 1.55 | −0.89 | 0.67 |
| 6 | 4.55 | 1.39 | 4.70 | 1.71 | −0.61 | 0.50 | 2.95 | 1.60 | 3.10 | 1.69 | −0.59 | 0.53 |
| 7 | 5.00 | 1.63 | 4.67 | 1.65 | 1.24 | 0.49 | 4.10 | 2.23 | 4.40 | 2.05 | −1.06 | 0.65 |
| 8 | 4.08 | 1.78 | 3.97 | 1.68 | 0.45 | 0.66 | 3.27 | 2.01 | 3.75 | 1.75 | −1.93 | 0.65 |
| 9 | 4.18 | 1.62 | 4.15 | 1.60 | 0.09 | 0.45 | 4.51 | 2.27 | 4.95 | −1.27 | −1.27 | 0.51 |
| 10 | 5.27 | 2,14 | 5.62 | 1.78 | −1.38 | 0.69 | 1.49 | 1.24 | 1.40 | 0.36 | 0.36 | 0.42 |
| 11 | 4.76 | 2.00 | 5.19 | 1.81 | −1.65 | 0.64 | 1.51 | 0.87 | 1.57 | −0.29 | −0.29 | 0.39 |
| 12 | 4.05 | 1.60 | 4.00 | 1.59 | 0.24 | 0.65 | 4.74 | 2.14 | 4.74 | 1.92 | 0.00 | 0.67 |
| 13 | 3.33 | 1.75 | 3.33 | 1.34 | 0.00 | 0.67 | 2.68 | 1.71 | 2.69 | 1.38 | −0.11 | 0.57 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campillo-Cruz, M.; González-Gutiérrez, J.L.; Ardoy-Cuadros, J.; Fernández-Muñoz, J.J. The Development and Exploratory Psychometric Properties of the Traumatic and Routine Stressors Scale on Emergency Nurses (TRSS-EN). Int. J. Environ. Res. Public Health 2020, 17, 1963. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061963
Campillo-Cruz M, González-Gutiérrez JL, Ardoy-Cuadros J, Fernández-Muñoz JJ. The Development and Exploratory Psychometric Properties of the Traumatic and Routine Stressors Scale on Emergency Nurses (TRSS-EN). International Journal of Environmental Research and Public Health. 2020; 17(6):1963. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061963
Chicago/Turabian StyleCampillo-Cruz, Manuel, José Luís González-Gutiérrez, Juan Ardoy-Cuadros, and Juan José Fernández-Muñoz. 2020. "The Development and Exploratory Psychometric Properties of the Traumatic and Routine Stressors Scale on Emergency Nurses (TRSS-EN)" International Journal of Environmental Research and Public Health 17, no. 6: 1963. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061963