The G-Protein-Coupled Estrogen Receptor (GPER/GPR30) in Ovarian Granulosa Cell Tumors


Abstract
:1. Introduction
2. Results and Discussion
2.1. Patient Characteristics According to GPER Immunoreactivity


{kind=link}
{kind=link}
| Initial Diagnosis (n = 15) | Recurrence (n = 11) | |||||
|---|---|---|---|---|---|---|
| GPER Negative (IRS ≤ 2; n = 7) | GPER Positive (IRS > 2; n = 8) | p | GPER Negative (IRS ≤ 2; n = 5) | GPER Positive (IRS > 2; n = 6) | p | |
| pT | ||||||
| pT1 | 5 | 6 | ns | 1 | 3 | ns |
| pT2, pT3 | 2 | 1 | 4 | 1 | ||
| pN | ||||||
| pN0 | 1 | 3 | na | 0 | 0 | na |
| pN1 | 0 | 0 | 4 | 1 | ||
| subcellular localization | ||||||
| cytoplasm | na | 3 | na | na | 3 | na |
| membr. + cytopl. | na | 4 | na | 2 | ||
| nucleus | na | 1 | na | 1 | ||
| distribution | ||||||
| focal | na | 7 | na | na | 4 | na |
| uniform | na | 1 | na | 2 | ||
| patient age | ||||||
| ≤54.8 years | 3 | 2 | ns | 4 | 2 | ns |
| >54.8 years | 4 | 6 | 1 | 4 | ||
| Initial Diagnosis (n = 15) | Recurrence (n = 11) | ||||||
|---|---|---|---|---|---|---|---|
| GPER Negative (int ≤ 2; n = 12) | GPER Positive (int = 3; n = 3) | p | GPER Negative (int ≤ 2; n = 7) | GPER Positive (int = 3; n = 4) | p | ||
| pT | |||||||
| pT1 | 10 | 1 | ns | 3 | 1 | ns | |
| pT2, pT3 | 2 | 1 | 4 | 1 | |||
| pN | |||||||
| pN0 | 3 | 1 | na | 0 | 0 | na | |
| pN1 | 0 | 0 | 4 | 1 | |||
| subcellular localisation | |||||||
| cytoplasm | na | 1 | na | na | 1 | na | |
| membr. + cytopl. | na | 2 | na | 2 | |||
| nucleus | na | 0 | na | 1 | |||
| distribution | |||||||
| focal | na | 3 | na | na | 3 | na | |
| uniform | na | 0 | na | 1 | |||
| patient age | |||||||
| ≤54.8 years | 5 | 0 | ns | 4 | 2 | ns | |
| >54.8 years | 7 | 3 | 3 | 2 | |||
| Initial Diagnosis | Recurrence | |||
|---|---|---|---|---|
| GPER (n (IRS > 2) = 8) | GPER (n (int = 3) = 3) | GPER (n (IRS > 2) = 6) | GPER (n (int = 3) = 4) | |
| FSHR | 5/8 | 2/3 | 4/6 | 3/4 |
| LHCGR | 6/8 | 2/3 | 4/6 | 3/4 |
| Ki67 (≥10%) | 3/8 | 2/3 | 2/6 | 1/4 |
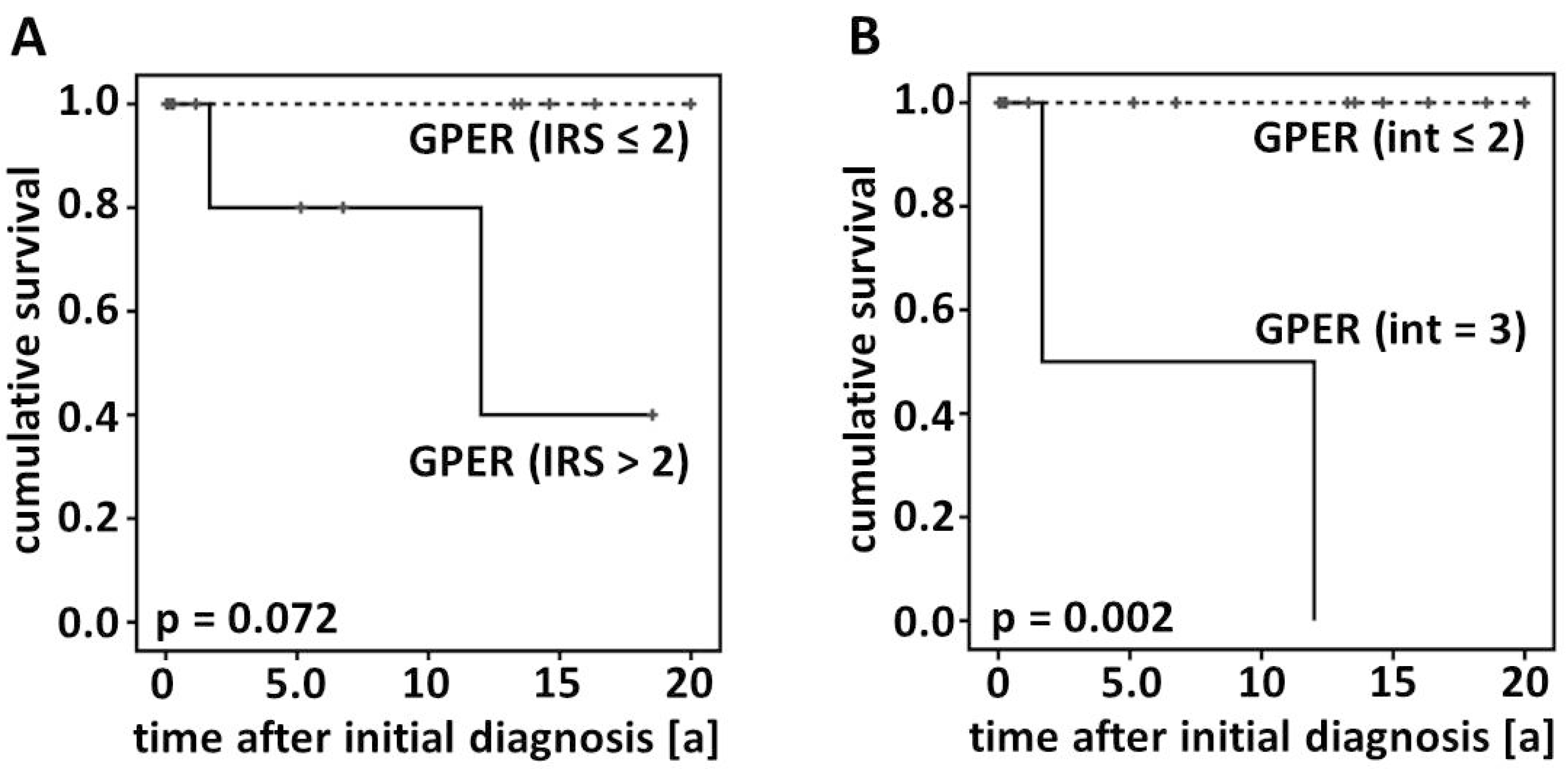
2.2. Survival

2.3. GPER and Hormone Receptor Insensitivity
2.4. Prognostic Significance of GPER in Ovarian Malignancies
3. Experimental Section
3.1. Patients
3.2. Ethical Considerations
3.3. Detection of GPER, Ki67, FSHR and LHCGR
3.4. Statistical Analysis
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Van Meurs, H.S.; van Lonkhuijzen, L.R.; Limpens, J.; van der Velden, J.; Buist, M.R. Hormone therapy in ovarian granulosa cell tumors: A systematic review. Gynecol. Oncol. 2014, 134, 196–205. [Google Scholar] [CrossRef]
- Van Meurs, H.S.; Bleeker, M.C.; van der Velden, J.; Overbeek, L.I.; Kenter, G.G.; Buist, M.R. The incidence of endometrial hyperplasia and cancer in 1031 patients with a granulosa cell tumor of the ovary: Long-term follow-up in a population-based cohort study. Int. J. Gynecol. Cancer 2013, 23, 1417–1422. [Google Scholar] [CrossRef]
- Park, J.Y.; Jin, K.L.; Kim, D.Y.; Kim, J.H.; Kim, Y.M.; Kim, K.R.; Kim, Y.T.; Nam, J.H. Surgical staging and adjuvant chemotherapy in the management of patients with adult granulosa cell tumors of the ovary. Gynecol. Oncol. 2012, 125, 80–86. [Google Scholar] [CrossRef]
- Jamieson, S.; Fuller, P.J. Management of granulosa cell tumour of the ovary. Curr. Opin. Oncol. 2008, 20, 560–564. [Google Scholar] [CrossRef]
- Van Meurs, H.S.; Buist, M.R.; Westermann, A.M.; Sonke, G.S.; Kenter, G.G.; van der Velden, J. Effectiveness of chemotherapy in measurable granulosa cell tumors: A retrospective study and review of literature. Int. J. Gynecol. Cancer 2014, 24, 496–505. [Google Scholar] [CrossRef]
- Davy, M.; Torjesen, P.A.; Aakavaag, A. Demonstration of an FSH receptor in a functioning granulosa cell tumour. The effect of gonadotrophin treatment on its viability following transplantation to nude mice. Acta Endocrinol. 1977, 85, 615–623. [Google Scholar]
- Jarrin Franco, M.; Kirchner, T.; Engel, J.; Lauf, S.; Mayerhofer, A.; Mayr, D. The prelevance of steroid hormone receptors (estrogene alpha and beta, progesterone), luteinizing hormone and follicle-stimulation hormone receptor as well as aromatase activity in granulosa cell tumors (GCTs) of the ovary. In Proceedings of 96 Jahrestagung der Deutschen Gesellschaft für Pathologie e.V., Berlin, Germany, 31 May–3 June 2012.
- Hardy, R.D.; Bell, J.G.; Nicely, C.J.; Reid, G.C. Hormonal treatment of a recurrent granulosa cell tumor of the ovary: Case report and review of the literature. Gynecol. Oncol. 2005, 96, 865–869. [Google Scholar] [CrossRef]
- Heublein, S.; Mayr, D.; Vrekoussis, T.; Friese, K.; Hofmann, S.S.; Jeschke, U.; Lenhard, M. The G-protein coupled estrogen receptor (GPER/GPR30) is a gonadotropin receptor dependent positive prognosticator in ovarian carcinoma patients. PLoS One 2013, 8, e71791. [Google Scholar]
- Heublein, S.; Vrekoussis, T.; Kuhn, C.; Friese, K.; Makrigiannakis, A.; Mayr, D.; Lenhard, M.; Jeschke, U. Inducers of G-protein coupled estrogen receptor (GPER) in endometriosis: potential implications for macrophages and follicle maturation. J. Reprod. Immunol. 2013, 97, 95–103. [Google Scholar] [CrossRef]
- Revankar, C.M.; Cimino, D.F.; Sklar, L.A.; Arterburn, J.B.; Prossnitz, E.R. A transmembrane intracellular estrogen receptor mediates rapid cell signaling. Science 2005, 307, 1625–1630. [Google Scholar] [CrossRef]
- Chevalier, N.; Vega, A.; Bouskine, A.; Siddeek, B.; Michiels, J.F.; Chevallier, D.; Fenichel, P. GPR30, the non-classical membrane G protein related estrogen receptor, is overexpressed in human seminoma and promotes seminoma cell proliferation. PLoS One 2012, 7, e34672. [Google Scholar]
- Smith, H.O.; Arias-Pulido, H.; Kuo, D.Y.; Howard, T.; Qualls, C.R.; Lee, S.J.; Verschraegen, C.F.; Hathaway, H.J.; Joste, N.E.; Prossnitz, E.R. GPR30 predicts poor survival for ovarian cancer. Gynecol. Oncol. 2009, 114, 465–471. [Google Scholar] [CrossRef]
- Pang, Y.; Thomas, P. Role of G protein-coupled estrogen receptor 1, GPER, in inhibition of oocyte maturation by endogenous estrogens in zebrafish. Dev. Biol. 2010, 342, 194–206. [Google Scholar] [CrossRef]
- Wang, C.; Lv, X.; He, C.; Hua, G.; Tsai, M.Y.; Davis, J.S. The G-protein-coupled estrogen receptor agonist G-1 suppresses proliferation of ovarian cancer cells by blocking tubulin polymerization. Cell Death Dis. 2013, 4, e869. [Google Scholar] [CrossRef]
- Lee, H.C.; Ko, H.; Seol, H.; Noh, D.Y.; Han, W.; Kim, T.Y.; Im, S.A.; Park, I.A. Expression of immunohistochemical markers before and after neoadjuvant chemotherapy in breast carcinoma, and their use as predictors of response. J. Breast Cancer 2013, 16, 395–403. [Google Scholar] [CrossRef]
- Arapantoni-Dadioti, P.; Valavanis, C.; Gavressea, T.; Tzaida, O.; Trihia, H.; Lekka, I. Discordant expression of hormone receptors and HER2 in breast cancer. A retrospective comparison of primary tumors with paired metachronous recurrences or metastases. J. BUON 2012, 17, 277–283. [Google Scholar]
- Heublein, S.; Lenhard, M.; Vrekoussis, T.; Schoepfer, J.; Kuhn, C.; Friese, K.; Makrigiannakis, A.; Mayr, D.; Jeschke, U. The G-protein-coupled estrogen receptor (GPER) is expressed in normal human ovaries and is upregulated in ovarian endometriosis and pelvic inflammatory disease involving the ovary. Reprod. Sci. 2012, 19, 1197–1204. [Google Scholar] [CrossRef]
- Kolkova, Z.; Casslen, V.; Henic, E.; Ahmadi, S.; Ehinger, A.; Jirstrom, K.; Casslen, B. The G protein-coupled estrogen receptor 1 (GPER/GPR30) does not predict survival in patients with ovarian cancer. J. Ovarian Res. 2012, 5, 9. [Google Scholar] [CrossRef]
- Ignatov, T.; Modl, S.; Thulig, M.; Weissenborn, C.; Treeck, O.; Ortmann, O.; Zenclussen, A.; Costa, S.D.; Kalinski, T.; Ignatov, A. GPER-1 acts as a tumor suppressor in ovarian cancer. J. Ovarian Res. 2013, 6, 51. [Google Scholar] [CrossRef]
- Smith, H.O.; Leslie, K.K.; Singh, M.; Qualls, C.R.; Revankar, C.M.; Joste, N.E.; Prossnitz, E.R. GPR30: A novel indicator of poor survival for endometrial carcinoma. Am. J. Obstet. Gynecol. 2007, 196, 386. [Google Scholar]
- Rago, V.; Romeo, F.; Giordano, F.; Maggiolini, M.; Carpino, A. Identification of the estrogen receptor GPER in neoplastic and non-neoplastic human testes. Reprod. Biol. Endocrinol. 2011, 9, 135. [Google Scholar] [CrossRef]
- Franco, R.; Boscia, F.; Gigantino, V.; Marra, L.; Esposito, F.; Ferrara, D.; Pariante, P.; Botti, G.; Caraglia, M.; Minucci, S.; et al. GPR30 is overexpressed in post-puberal testicular germ cell tumors. Cancer Biol. Ther. 2011, 11, 609–613. [Google Scholar] [CrossRef]
- Chevalier, N.; Paul-Bellon, R.; Camparo, P.; Michiels, J.F.; Chevallier, D.; Fenichel, P. Genetic variants of GPER/GPR30, a novel estrogen-related G protein receptor, are associated with human seminoma. Int. J. Mol. Sci. 2014, 15, 1574–1589. [Google Scholar] [CrossRef]
- Leitlinienprogramm Onkologie. Available online: http://leitlinienprogramm-onkologie.de/Leitlinien.7.0.html (accessed on 21 September 2014).
- Kriegl, L.; Neumann, J.; Vieth, M.; Greten, F.R.; Reu, S.; Jung, A.; Kirchner, T. Up and downregulation of p16(Ink4a) expression in BRAF-mutated polyps/adenomas indicates a senescence barrier in the serrated route to colon cancer. Mod. Pathol. 2011, 24, 1015–1022. [Google Scholar] [CrossRef]
- Remmele, W.; Stegner, H.E. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987, 8, 138–140. [Google Scholar]
- Lenhard, M.; Lennerova, T.; Ditsch, N.; Kahlert, S.; Friese, K.; Mayr, D.; Jeschke, U. Opposed roles of follicle-stimulating hormone and luteinizing hormone receptors in ovarian cancer survival. Histopathology 2011, 58, 990–994. [Google Scholar] [CrossRef]
- Lenhard, M.; Tsvilina, A.; Schumacher, L.; Kupka, M.; Ditsch, N.; Mayr, D.; Friese, K.; Jeschke, U. Human chorionic gonadotropin and its relation to grade, stage and patient survival in ovarian cancer. BMC Cancer 2012, 12, 2. [Google Scholar] [CrossRef]
- Engelstaedter, V.; Heublein, S.; Schumacher, A.L.; Lenhard, M.; Engelstaedter, H.; Andergassen, U.; Guenthner-Biller, M.; Kuhn, C.; Rack, B.; Kupka, M.; et al. Mucin-1 and its relation to grade, stage and survival in ovarian carcinoma patients. BMC Cancer 2012, 12, 600. [Google Scholar] [CrossRef]
- Heublein, S.; Grasse, K.; Hessel, H.; Burges, A.; Lenhard, M.; Engel, J.; Kirchner, T.; Jeschke, U.; Mayr, D. KRAS, BRAF genotyping reveals genetic heterogeneity of ovarian borderline tumors and associated implants. BMC Cancer 2013, 13, 483. [Google Scholar] [CrossRef]
- Lenhard, M.; Tereza, L.; Heublein, S.; Ditsch, N.; Himsl, I.; Mayr, D.; Friese, K.; Jeschke, U. Steroid hormone receptor expression in ovarian cancer: Progesterone receptor B as prognostic marker for patient survival. BMC Cancer 2012, 12, 553. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Heublein, S.; Mayr, D.; Friese, K.; Jarrin-Franco, M.C.; Lenhard, M.; Mayerhofer, A.; Jeschke, U. The G-Protein-Coupled Estrogen Receptor (GPER/GPR30) in Ovarian Granulosa Cell Tumors. Int. J. Mol. Sci. 2014, 15, 15161-15172. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms150915161
Heublein S, Mayr D, Friese K, Jarrin-Franco MC, Lenhard M, Mayerhofer A, Jeschke U. The G-Protein-Coupled Estrogen Receptor (GPER/GPR30) in Ovarian Granulosa Cell Tumors. International Journal of Molecular Sciences. 2014; 15(9):15161-15172. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms150915161
Chicago/Turabian StyleHeublein, Sabine, Doris Mayr, Klaus Friese, Maria Cristina Jarrin-Franco, Miriam Lenhard, Artur Mayerhofer, and Udo Jeschke. 2014. "The G-Protein-Coupled Estrogen Receptor (GPER/GPR30) in Ovarian Granulosa Cell Tumors" International Journal of Molecular Sciences 15, no. 9: 15161-15172. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms150915161