Evaluation for Synergistic Effects by Combinations of Photodynamic Therapy (PDT) with Temoporfin (mTHPC) and Pt(II) Complexes Carboplatin, Cisplatin or Oxaliplatin in a Set of Five Human Cancer Cell Lines


Abstract
:
1. Introduction
2. Results
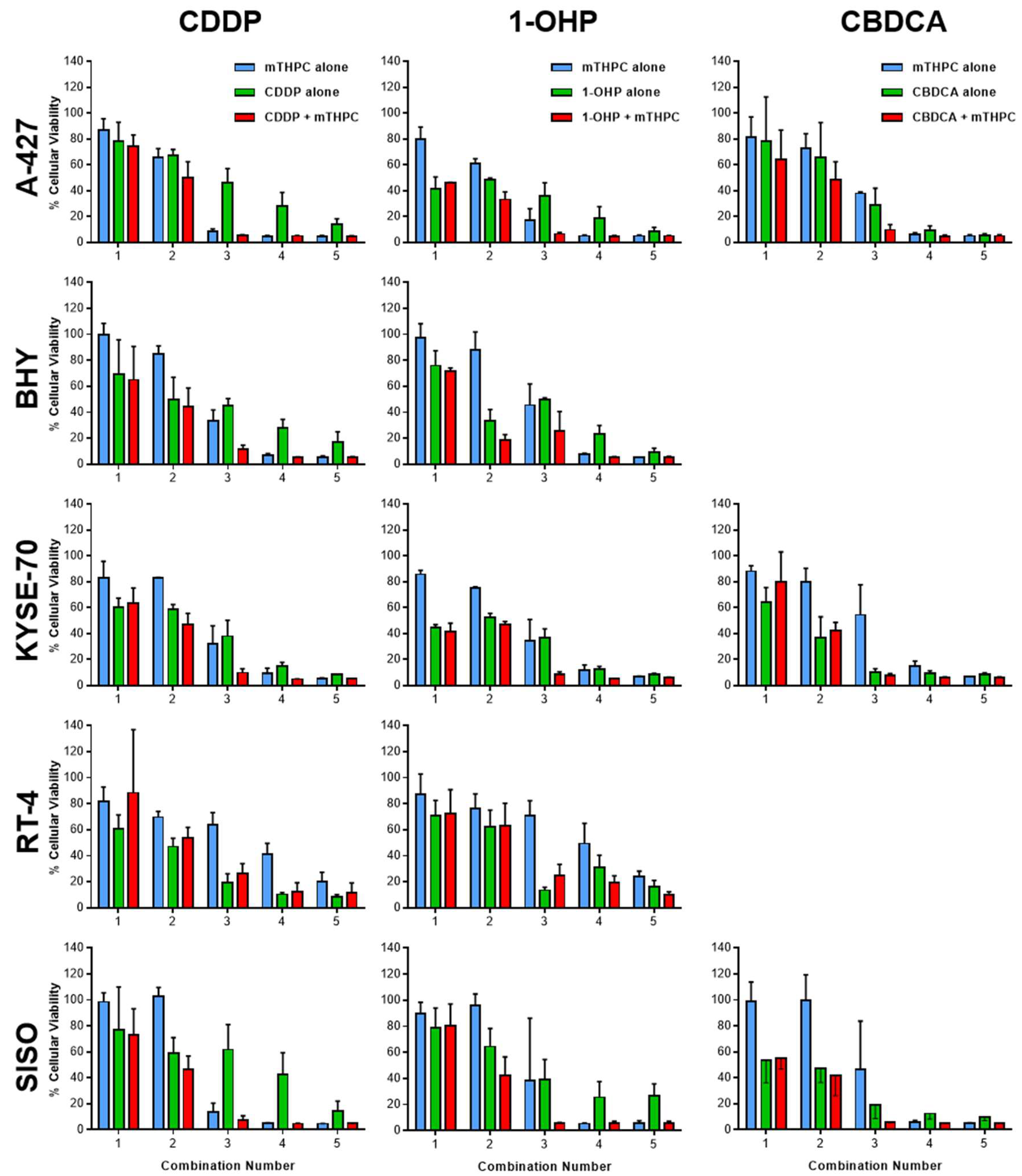
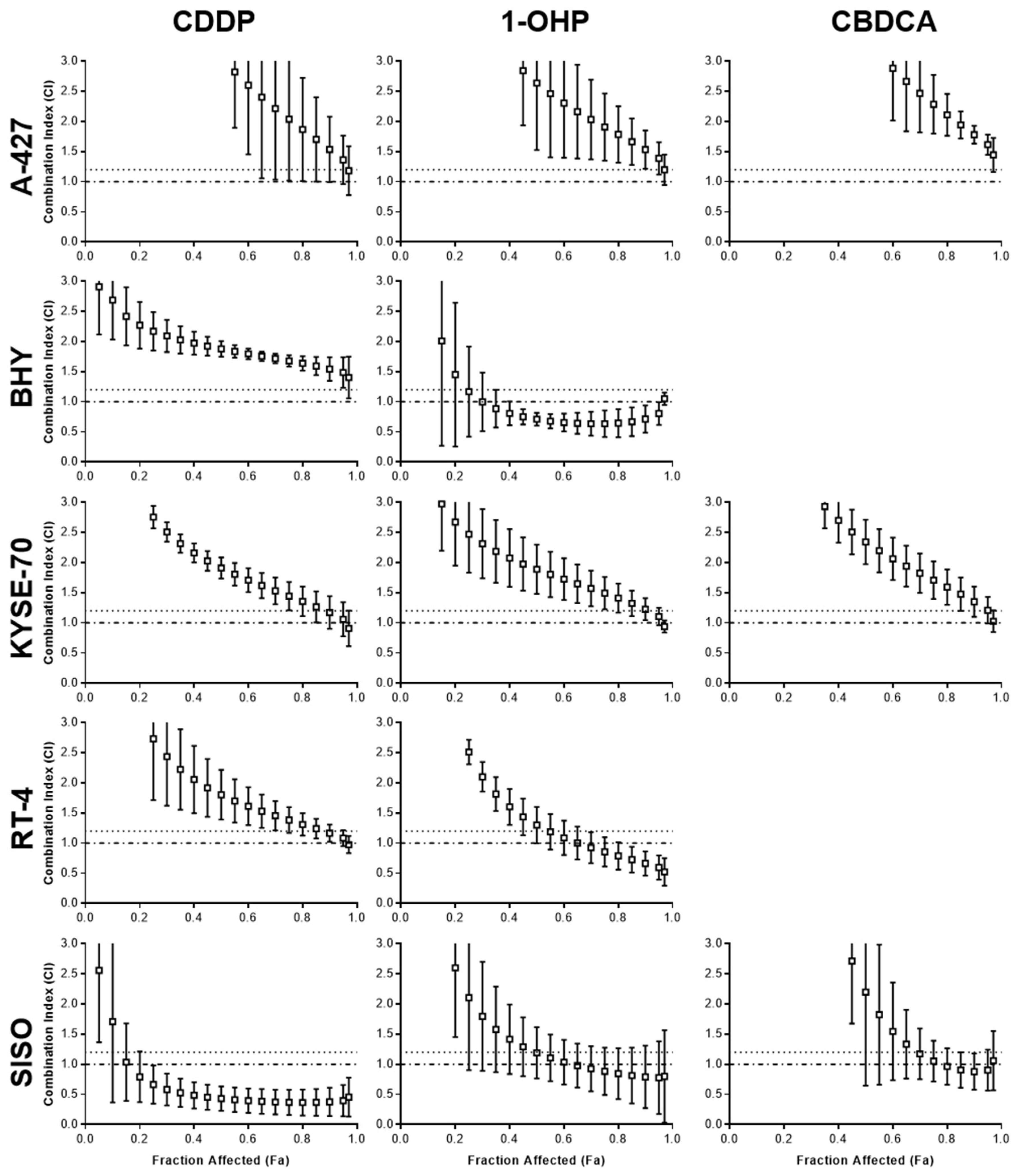
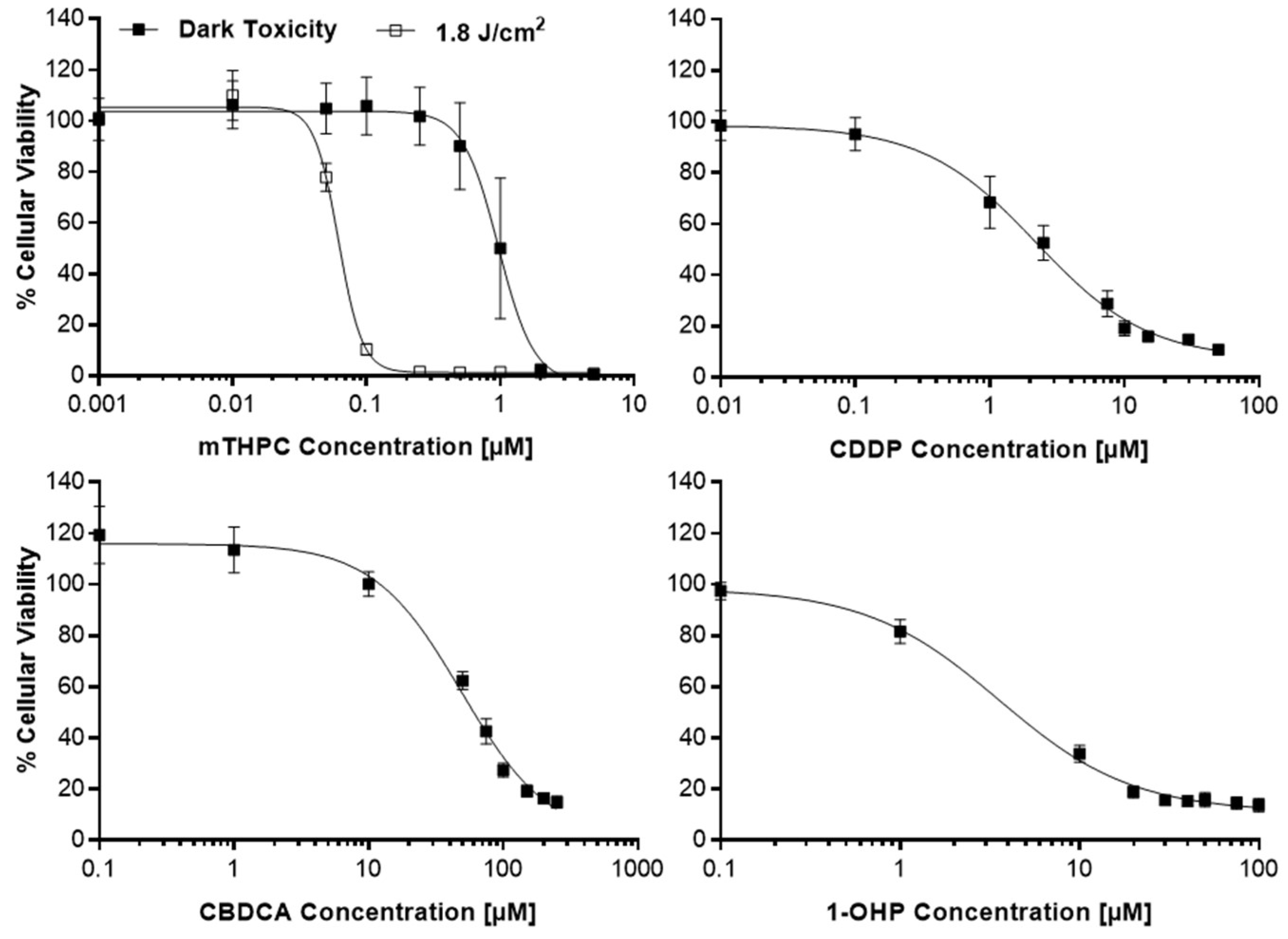
2.1. Detection of Synergism after Combination of mTHPC-PDT and a Pt(II) Complex
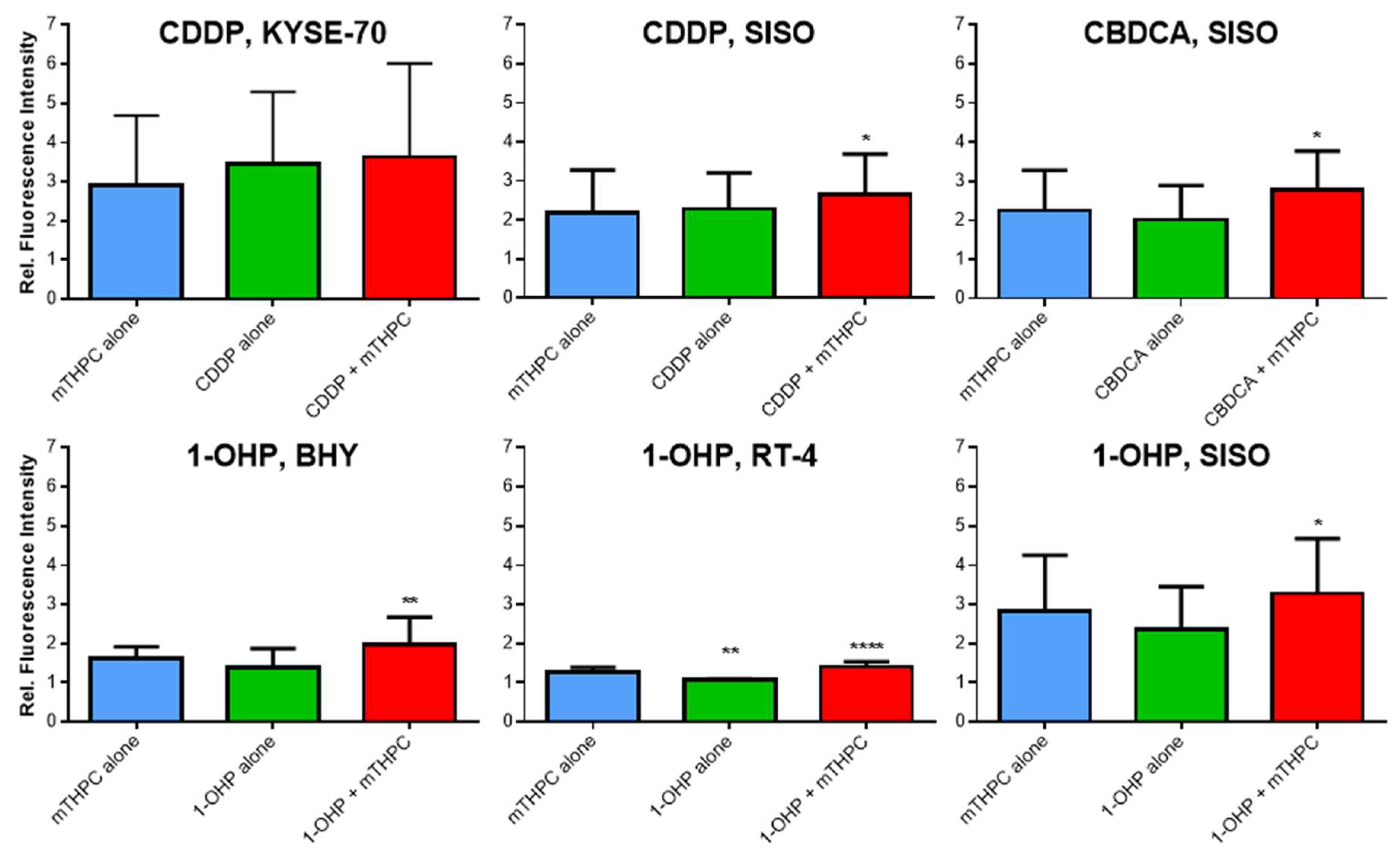
2.2. Elevated ROS Levels after Combination of mTHPC-PDT and a Pt(II) Complex
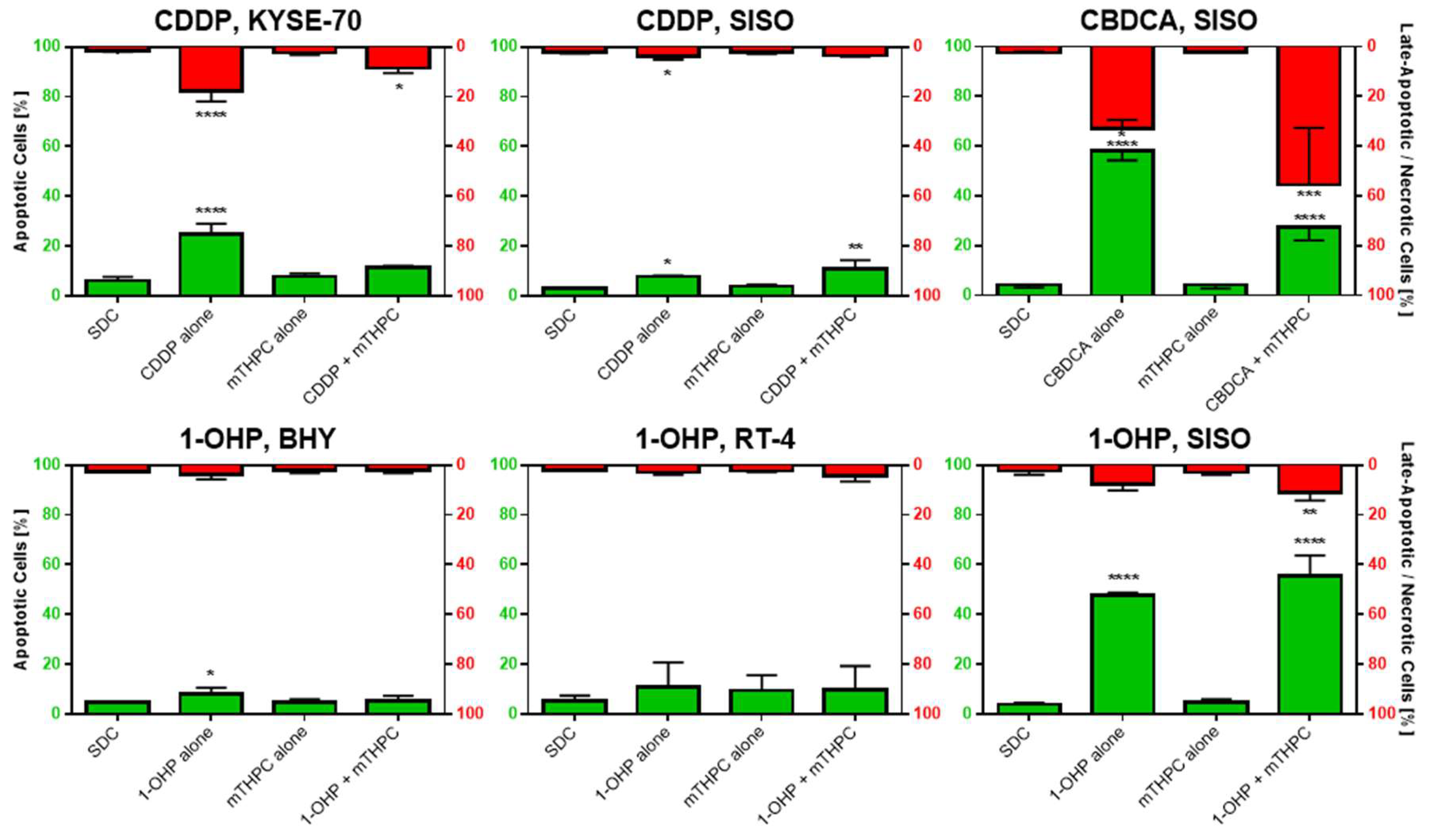
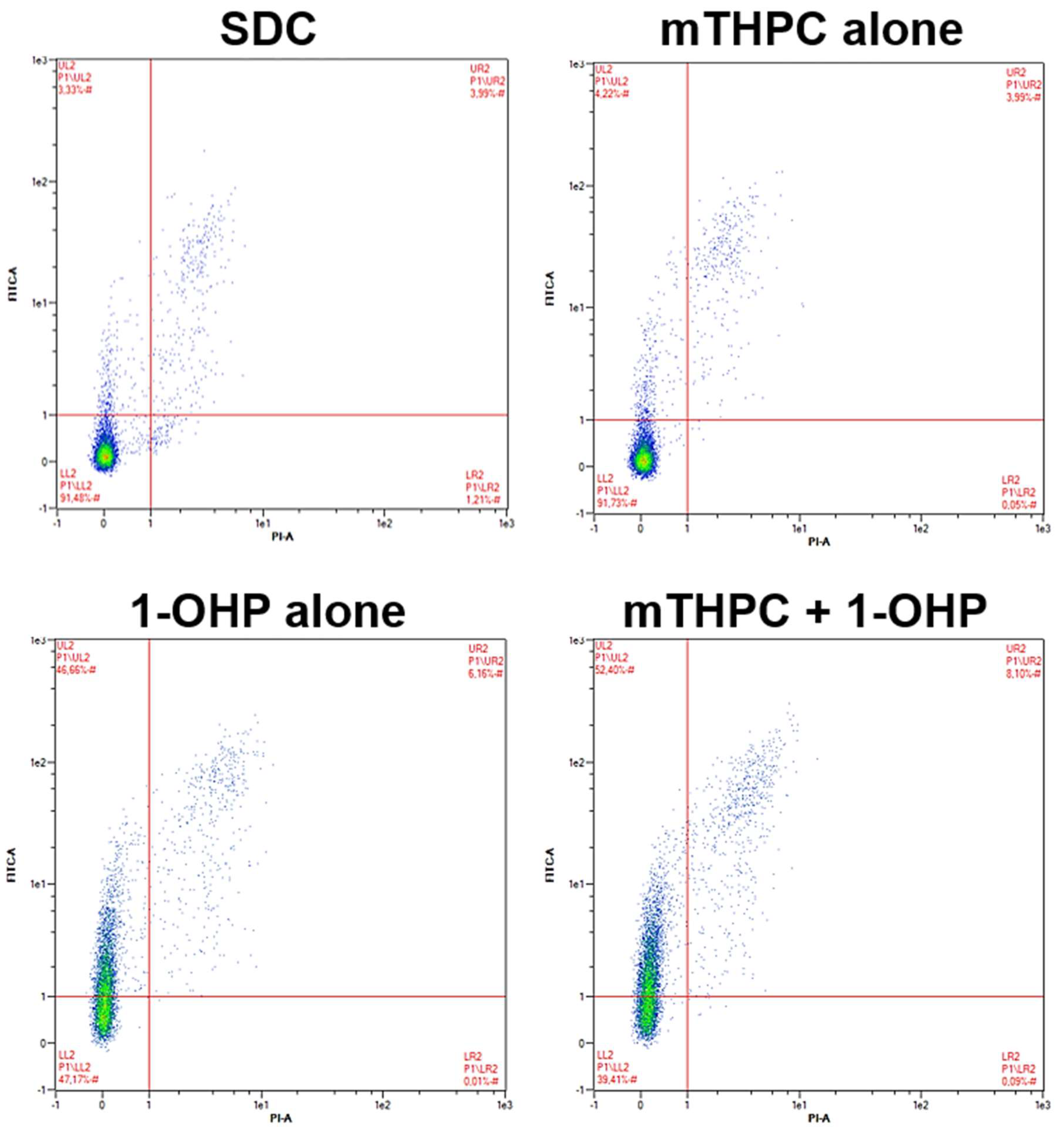
2.3. Combination of mTHPC-PDT and a Pt(II) Complex Can Lead to Enhanced Phosphatidylserine Externalization as a Sign of Increased Apoptosis Induction
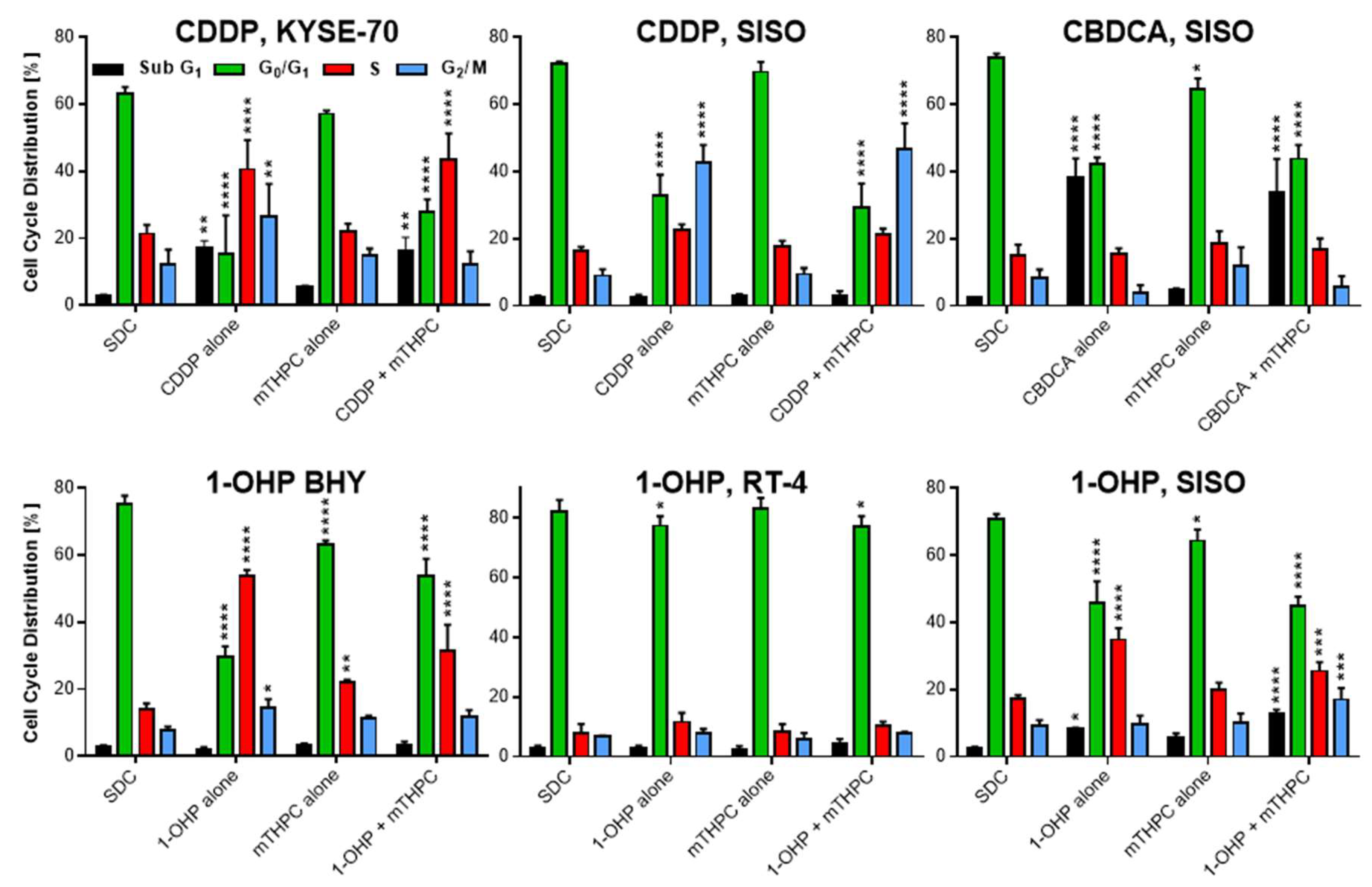
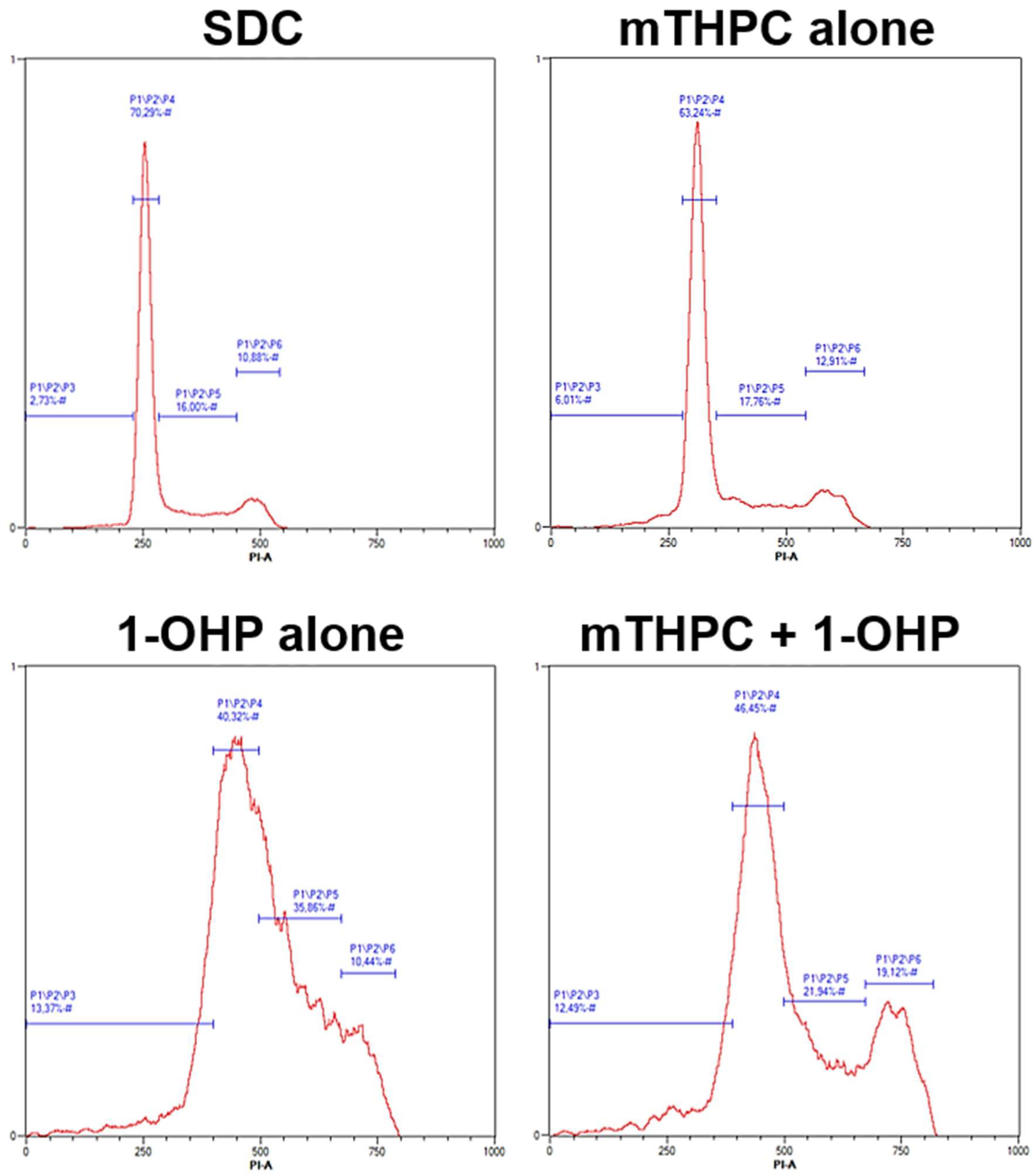
2.4. Cell Growth Arrest and DNA Fragmentation Observed in Cell Cycle Analysis
3. Discussion
4. Materials and Methods
4.1. Cell Culture
4.2. Treatment with Photosensitizer and Pt(II) Complexes
4.3. Photodynamic Treatment
4.4. Analysis of Cell Viability by the MTT Assay
4.5. Analysis of ROS Generation
4.6. Analysis of Apoptosis by the Annexin V-FITC/Propidium Iodide Assay
4.7. Cell Cycle Analysis
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| (N)SCLC | (Non-)Small Cell Lung Cancer |
| 1-OHP | Oxaliplatin, trans-R,R-Cyclohexane-1,2-diamineoxalatoplatinum(II) |
| 9-HPbD | 9-Hydroxypheophorbide α |
| CBDCA | Carboplatin, cis-Diammine-1,1-cyclobutanedicarboxylatoplatinum(II) |
| CDDP | Cisplatin, cis-Diamminedichloridoplatinum(II) |
| CI | Combination Index |
| DCF | 2′,7′-Dichlorofluorescein |
| Fa | Fraction affected |
| FBS | Fetal Bovine Serum |
| GSH | Glutathione |
| H2DCF-DA | 2′,7′-Dichlorodihydrofluorescein Diacetate |
| LED | Light-emitting Diode |
| mTHPC | 5,10,15,20-tetra(m-Hydroxyphenyl)chlorin |
| MTT | 3-(4,5-Dimethyl-2-thiazolyl)-2,5-diphenyl-2H-tetrazolium Bromide |
| PARP | Poly(ADP-Ribose) Polymerase |
| PBS | Phosphate Buffered Saline |
| PDT | Photodynamic Therapy |
| PI | Propidium Iodide |
| PTX | Paclitaxel |
| ROS | Reactive Oxygen Species |
| SDC | Solvent Dark Control |
Appendix A




References
- Barnard, C. Platinum group metal compounds in cancer chemotherapy. Johnson Matthey Technol. Rev. 2017, 61, 52–59. [Google Scholar] [CrossRef]
- Lin, S.; Lei, K.; Du, W.; Yang, L.; Shi, H.; Gao, Y.; Yin, P.; Liang, X.; Liu, J. Enhancement of oxaliplatin sensitivity in human colorectal cancer by hypericin mediated photodynamic therapy via ROS-related mechanism. Int. J. Biochem. Cell. Biol. 2016, 71, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Rozzi, A.; Nardoni, C.; Corona, M.; Restuccia, M.R.; Falbo, T.; Lanzetta, G. Weekly regimen of paclitaxel and carboplatin as first-line chemotherapy in elderly patients with stage IIIB-IV non small cell lung cancer (NSCLC): Results of a phase II study. J. Chemother. 2010, 22, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Comella, P.; Casaretti, R.; Sandomenico, C.; Avallone, A.; Franco, L. Role of oxaliplatin in the treatment of colorectal cancer. Ther. Clin. Risk Manag. 2009, 5, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Galanski, M.; Jakupec, M.A.; Keppler, B.K. Update of the preclinical situation of anticancer platinum complexes: Novel design strategies and innovative analytical approaches. Curr. Med. Chem. 2005, 12, 2075–2094. [Google Scholar] [CrossRef] [PubMed]
- Desoize, B. Metals and metal compounds in cancer treatment. Anticancer Res. 2004, 24, 1529–1544. [Google Scholar] [PubMed]
- Johnstone, T.C.; Park, G.Y.; Lippard, S.J. Understanding and improving platinum anticancer drugs—Phenanthriplatin. Anticancer Res. 2014, 34, 471–476. [Google Scholar] [PubMed]
- Tonetti, M.; Giovine, M.; Gasparini, A.; Benatti, U.; De Flora, A. Enhanced formation of reactive species from cis-diammine-(1,1-cyclobutanedicarboxylato)-platinum(II) (carboplatin) in the presence of oxygen free radicals. Biochem. Pharmacol. 1993, 46, 1377–1383. [Google Scholar] [CrossRef]
- Shylasree, T.S.; Bryant, A.; Athavale, R. Chemotherapy and/or radiotherapy in combination with surgery for ovarian carcinosarcoma. Cochrane Database Syst. Rev. 2013, Cd006246. [Google Scholar] [CrossRef] [PubMed]
- Gabrilovich, D.I. Combination of chemotherapy and immunotherapy for cancer: A paradigm revisited. Lancet Oncol. 2007, 8, 2–3. [Google Scholar] [CrossRef]
- Flaherty, K.T. Chemotherapy and targeted therapy combinations in advanced melanoma. Clin. Cancer Res. 2006, 12, 2366s–2370s. [Google Scholar] [CrossRef] [PubMed]
- Lange, C.; Bednarski, P.J. Photosensitizers for photodynamic therapy: Photochemistry in the service of oncology. Curr. Pharm. Des. 2016, 22, 6956–6974. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.B.; Brown, E.A.; Walker, I. The present and future role of photodynamic therapy in cancer treatment. Lancet Oncol. 2004, 5, 497–508. [Google Scholar] [CrossRef]
- Senge, O.; Brandt, J.C. Temoporfin (Foscan®, 5,10,15,20-tetra(m-hydroxyphenyl)chlorin)—A second-generation photosensitizer. Photochem. Photobiol. 2011, 87, 1240–1296. [Google Scholar] [CrossRef] [PubMed]
- Compagnin, C.; Mognato, M.; Celotti, L.; Canti, G.; Palumbo, G.; Reddi, E. Cell proliferation and cell cycle alterations in oesophageal p53-mutated cancer cells treated with cisplatin in combination with photodynamic therapy. Cell Prolif. 2010, 43, 262–274. [Google Scholar] [CrossRef] [PubMed]
- Nonaka, M.; Ikeda, H.; Inokuchi, T. Effect of combined photodynamic and chemotherapeutic treatment on lymphoma cells in vitro. Cancer Lett. 2002, 184, 171–178. [Google Scholar] [CrossRef]
- Cheng, Y.S.; Peng, Y.B.; Yao, M.; Teng, J.P.; Ni, D.; Zhu, Z.J.; Zhuang, B.F.; Yang, Z.Y. Cisplatin and photodynamic therapy exert synergistic inhibitory effects on small-cell lung cancer cell viability and xenograft tumor growth. Biochem. Biophys. Res. Commun. 2017, 487, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Mao, W.; Sun, Y.; Zhang, H.; Cao, L.; Wang, J.; He, P. A combined modality of carboplatin and photodynamic therapy suppresses epithelial-mesenchymal transition and matrix metalloproteinase-2 (MMP-2)/MMP-9 expression in HEp-2 human laryngeal cancer cells via ROS-mediated inhibition of MEK/ERK signalling pathway. Lasers Med. Sci. 2016, 31, 1697–1705. [Google Scholar] [CrossRef] [PubMed]
- He, P.; Ahn, J.C.; Shin, J.I.; Hwang, H.J.; Kang, J.W.; Lee, S.J.; Chung, P.S. Enhanced apoptotic effect of combined modality of 9-hydroxypheophorbide α-mediated photodynamic therapy and carboplatin on AMC-HN-3 human head and neck cancer cells. Oncol. Rep. 2009, 21, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.; Biswas, R.; Chung, P.S.; Ahn, J.C. Modulation of EGFR and ROS induced cytochrome c release by combination of photodynamic therapy and carboplatin in human cultured head and neck cancer cells and tumor xenograft in nude mice. J. Photochem. Photobiol. B 2013, 128, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, I.; Celli, J.P.; Evans, C.L.; Abu-Yousif, A.O.; Muzikansky, A.; Pogue, B.W.; Finkelstein, D.; Hasan, T. Synergistic enhancement of carboplatin efficacy with photodynamic therapy in a three-dimensional model for micrometastatic ovarian cancer. Cancer Res. 2010, 70, 9319–9328. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Chang, J.E.; Jheon, S.; Han, S.J.; Kim, J.K. Enhanced production of reactive oxygen species in HeLa cells under concurrent lowdose carboplatin and Photofrin(R) photodynamic therapy. Oncol. Rep. 2018, 40, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Chou, T.-C. Drug combination studies and their synergy quantification using the Chou-Talalay method. Cancer Res. 2010, 70, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Melnikova, V.O.; Bezdetnaya, L.N.; Potapenko, A.Y.; Guillemin, F. Photodynamic properties of meta-tetra(hydroxyphenyl)chlorin in human tumor cells. Radiat. Res. 1999, 152, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Fadok, V.A.; Voelker, D.R.; Campbell, P.A.; Cohen, J.J.; Bratton, D.L.; Henson, P.M. Exposure of phosphatidylserine on the surface of apoptotic lymphocytes triggers specific recognition and removal by macrophages. J. Immunol. 1992, 148, 2207–2216. [Google Scholar] [PubMed]
- Nagata, S.; Nagase, H.; Kawane, K.; Mukae, N.; Fukuyama, H. Degradation of chromosomal DNA during apoptosis. Cell Death Differ. 2003, 10, 108–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unger, F.T.; Klasen, H.A.; Tchartchian, G.; de Wilde, R.L.; Witte, I. DNA damage induced by cis- and carboplatin as indicator for in vitro sensitivity of ovarian carcinoma cells. BMC Cancer 2009, 9, 359. [Google Scholar] [CrossRef] [PubMed]
- Faivre, S.; Chan, D.; Salinas, R.; Woynarowska, B.; Woynarowski, J.M. DNA strand breaks and apoptosis induced by oxaliplatin in cancer cells. Biochem. Pharmacol. 2003, 66, 225–237. [Google Scholar] [CrossRef]
- Woynarowski, J.M.; Faivre, S.; Herzig, M.C.; Arnett, B.; Chapman, W.G.; Trevino, A.V.; Raymond, E.; Chaney, S.G.; Vaisman, A.; Varchenko, M.; et al. Oxaliplatin-induced damage of cellular DNA. Mol. Pharmacol. 2000, 58, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Alberts, D.S. Carboplatin versus cisplatin in ovarian cancer. Semin. Oncol. 1995, 22, 88–90. [Google Scholar] [PubMed]
- Canti, G.; Calastretti, A.; Bevilacqua, A.; Reddi, E.; Palumbo, G.; Nicolin, A. Combination of photodynamic therapy + immunotherapy + chemotherapy in murine leukiemia. Neoplasma 2010, 57, 184–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirveliene, V.; Grazeliene, G.; Dabkeviciene, D.; Micke, I.; Kirvelis, D.; Juodka, B.; Didziapetriene, J. Schedule-dependent interaction between Doxorubicin and mTHPC-mediated photodynamic therapy in murine hepatoma in vitro and in vivo. Cancer Chemother. Pharmacol. 2006, 57, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Van Geel, I.P.; Oppelaar, H.; Oussoren, Y.G.; Schuitmaker, J.J.; Stewart, F.A. Mechanisms for optimising photodynamic therapy: Second-generation photosensitisers in combination with mitomycin C. Br. J. Cancer 1995, 72, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Biswas, R.; Chung, P.S.; Moon, J.H.; Lee, S.H.; Ahn, J.C. Carboplatin synergistically triggers the efficacy of photodynamic therapy via caspase 3-, 8-, and 12-dependent pathways in human anaplastic thyroid cancer cells. Lasers Med. Sci. 2014, 29, 995–1007. [Google Scholar] [CrossRef] [PubMed]
- Agostinis, P.; Berg, K.; Cengel, K.A.; Foster, T.H.; Girotti, A.W.; Gollnick, S.O.; Hahn, S.M.; Hamblin, M.R.; Juzeniene, A.; Kessel, D.; et al. Photodynamic therapy of cancer: An update. CA Cancer J. Clin. 2011, 61, 250–281. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.-M.; Kim, H.-K.; Shim, W.; Anwar, M.A.; Kwon, J.-W.; Kwon, H.-K.; Kim, H.J.; Jeong, H.; Kim, H.M.; Hwang, D.; et al. Mechanism of cisplatin-induced cytotoxicity is correlated to impaired metabolism due to mitochondrial ROS generation. PLoS ONE 2015, 10, e0135083. [Google Scholar] [CrossRef] [PubMed]
- Okamura, M.; Hashimoto, K.; Shimada, J.; Sakagami, H. Apoptosis-inducing activity of cisplatin (CDDP) against human hepatoma and oral squamous cell carcinoma cell lines. Anticancer Res. 2004, 24, 655–661. [Google Scholar] [PubMed]
- Di Felice, V.; Lauricella, M.; Giuliano, M.; Emanuele, S.; Vento, R.; Tesoriere, G. The apoptotic effects of cisplatin and carboplatin in retinoblastoma Y79 cells. Int. J. Oncol. 1998, 13, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.; Peng, X.; Peng, W.E.N.; Zhao, Y.; Wei, Y. Enhancement of oxaliplatin-induced cell apoptosis and tumor suppression by 3-methyladenine in colon cancer. Oncol. Lett. 2015, 9, 2056–2062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dasari, S.; Tchounwou, P.B. Cisplatin in cancer therapy: Molecular mechanisms of action. Eur. J. Pharmacol. 2014, 740, 364–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruet-Hennequart, S.; Villalan, S.; Kaczmarczyk, A.; O’Meara, E.; Sokol, A.M.; Carty, M.P. Characterization of the effects of cisplatin and carboplatin on cell cycle progression and DNA damage response activation in DNA polymerase eta-deficient human cells. Cell Cycle 2009, 8, 3043–3054. [Google Scholar] [CrossRef]
- Elmore, S. Apoptosis: A review of programmed cell death. Toxicol Pathol 2007, 35, 495–516. [Google Scholar] [CrossRef] [PubMed]
- Coleman, S.C.; Stewart, Z.A.; Day, T.A.; Netterville, J.L.; Burkey, B.B.; Pietenpol, J.A. Analysis of cell-cycle checkpoint pathways in head and neck cancer cell lines: Implications for therapeutic strategies. Arch. Otolaryngol. Head Neck Surg. 2002, 128, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Alcindor, T.; Beauger, N. Oxaliplatin: A review in the era of molecularly targeted therapy. Curr. Oncol. 2011, 18, 18–25. [Google Scholar] [CrossRef] [PubMed]
- William-Faltaos, S.; Rouillard, D.; Lechat, P.; Bastian, G. Cell cycle arrest and apoptosis induced by oxaliplatin (L-OHP) on four human cancer cell lines. Anticancer Res. 2006, 26, 2093–2099. [Google Scholar] [PubMed]
- Chou, T.-C. Theoretical basis, experimental design, and computerized simulation of synergism and antagonism in drug combination studies. Pharmacol. Rev. 2006, 58, 621–681. [Google Scholar] [CrossRef] [PubMed]
- Pieslinger, A.; Plaetzer, K.; Oberdanner, C.B.; Berlanda, J.; Mair, H.; Krammer, B.; Kiesslich, T. Characterization of a simple and homogeneous irradiation device based on light-emitting diodes: A possible low-cost supplement to conventional light sources for photodynamic treatment. Med. Laser Appl. 2006, 21, 277–283. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Substance | IC50 ± SD (µM) | ||||
|---|---|---|---|---|---|
| A-427 | BHY | KYSE-70 | RT-4 | SISO | |
| mTHPC + light | 0.02 ± 0.01 | 0.06 ± 0.01 | 0.06 ± 0.01 | 0.10 ± 0.01 | 0.06 ± 0.002 |
| Cisplatin | 17.3 ± 0.80 | 3.22 ± 0.63 | 8.15 ± 0.99 | 12.9 ± 6.76 | 2.31 ± 0.89 |
| Carboplatin | 205 ± 39.0 | n.d. | 220 ± 31.0 | n.d. | 50.1 ± 2.09 |
| Oxaliplatin | 45.4 ± 10.7 | 27.1 ± 3.74 | 36.7 ± 7.50 | 11.7 ± 4.73 | 3.41 ± 0.42 |
| Comb. | Cisplatin (µM) | Comb. | Carboplatin (µM) | ||||||
| Number | A-427 | BHY | KYSE-70 | RT-4 | SISO | Number | A-427 | KYSE-70 | SISO |
| 1 | 5.0 | 1.00 | 1.00 | 1.00 | 0.10 | 1 | 50.0 | 50.0 | 10.0 |
| 2 | 10.0 | 2.00 | 5.00 | 5.00 | 0.50 | 2 | 100 | 100 | 50.0 |
| 3 | 15.0 | 4.00 | 10.0 | 10.0 | 1.00 | 3 | 200 | 200 | 100 |
| 4 | 20.0 | 6.00 | 15.0 | 15.0 | 2.50 | 4 | 300 | 300 | 150 |
| 5 | 30.0 | 8.00 | 20.0 | 20.0 | 5.00 | 5 | 100 | 400 | 200 |
| Comb. | Oxaliplatin (µM) | Comb. | mTHPC (µM) | ||||||
| Number | A-427 | BHY | KYSE-70 | RT-4 | SISO | Number | All Cell Lines | ||
| 1 | 10.0 | 1.00 | 10.0 | 1.00 | 1.00 | 1 | 0.001 | ||
| 2 | 25.0 | 10.0 | 25.0 | 5.00 | 5.00 | 2 | 0.010 | ||
| 3 | 50.0 | 25.0 | 50.0 | 10.0 | 7.50 | 3 | 0.025 | ||
| 4 | 75.0 | 50.0 | 75.0 | 15.0 | 10.0 | 4 | 0.050 | ||
| 5 | 100 | 75.0 | 100 | 25.0 | 15.0 | 5 | 0.100 | ||
| Cell Line | mTHPC (µM) | Pt(II) Complex (µM) | ||
|---|---|---|---|---|
| CDDP | CBDCA | 1-OHP | ||
| A-427 | n.t. | n.t. | n.t. | n.t. |
| BHY | 0.025 | n.t. | n.t. | 25.0 |
| KYSE-70 | 0.025 | 10.0 | n.t. | n.t. |
| RT-4 | 0.050 | n.t. | n.t. | 15.0 |
| SISO | 0.010; 0.025 # | 0.50 | 100 | 7.5 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lange, C.; Bednarski, P.J. Evaluation for Synergistic Effects by Combinations of Photodynamic Therapy (PDT) with Temoporfin (mTHPC) and Pt(II) Complexes Carboplatin, Cisplatin or Oxaliplatin in a Set of Five Human Cancer Cell Lines. Int. J. Mol. Sci. 2018, 19, 3183. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19103183
Lange C, Bednarski PJ. Evaluation for Synergistic Effects by Combinations of Photodynamic Therapy (PDT) with Temoporfin (mTHPC) and Pt(II) Complexes Carboplatin, Cisplatin or Oxaliplatin in a Set of Five Human Cancer Cell Lines. International Journal of Molecular Sciences. 2018; 19(10):3183. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19103183
Chicago/Turabian StyleLange, Carsten, and Patrick J. Bednarski. 2018. "Evaluation for Synergistic Effects by Combinations of Photodynamic Therapy (PDT) with Temoporfin (mTHPC) and Pt(II) Complexes Carboplatin, Cisplatin or Oxaliplatin in a Set of Five Human Cancer Cell Lines" International Journal of Molecular Sciences 19, no. 10: 3183. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19103183