Differential Involvement of Autophagy and Apoptosis in Response to Chemoendocrine and Endocrine Therapy in Breast Cancer: JBCRG-07TR

 ,
, 
Abstract
:1. Introduction
2. Results
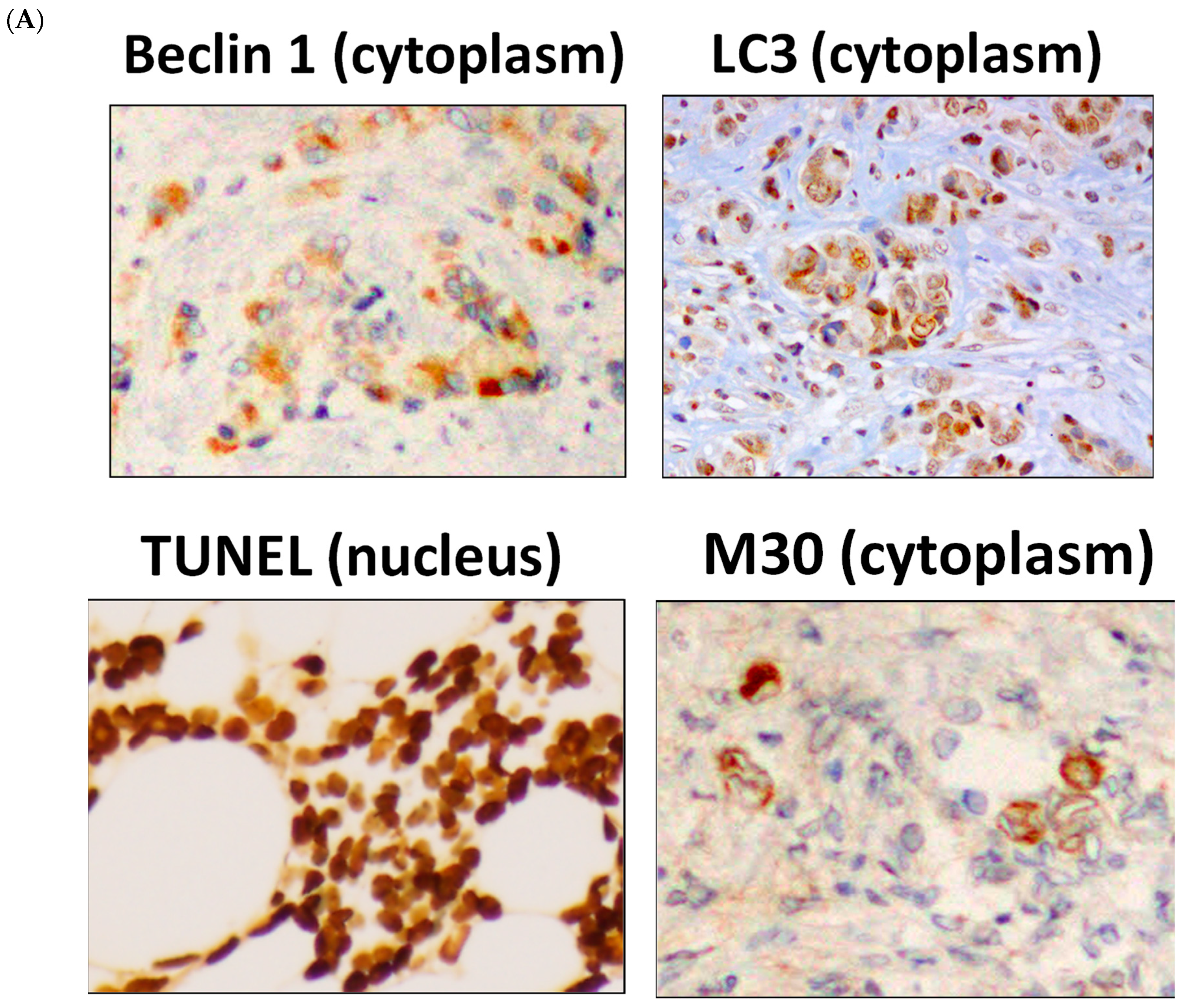
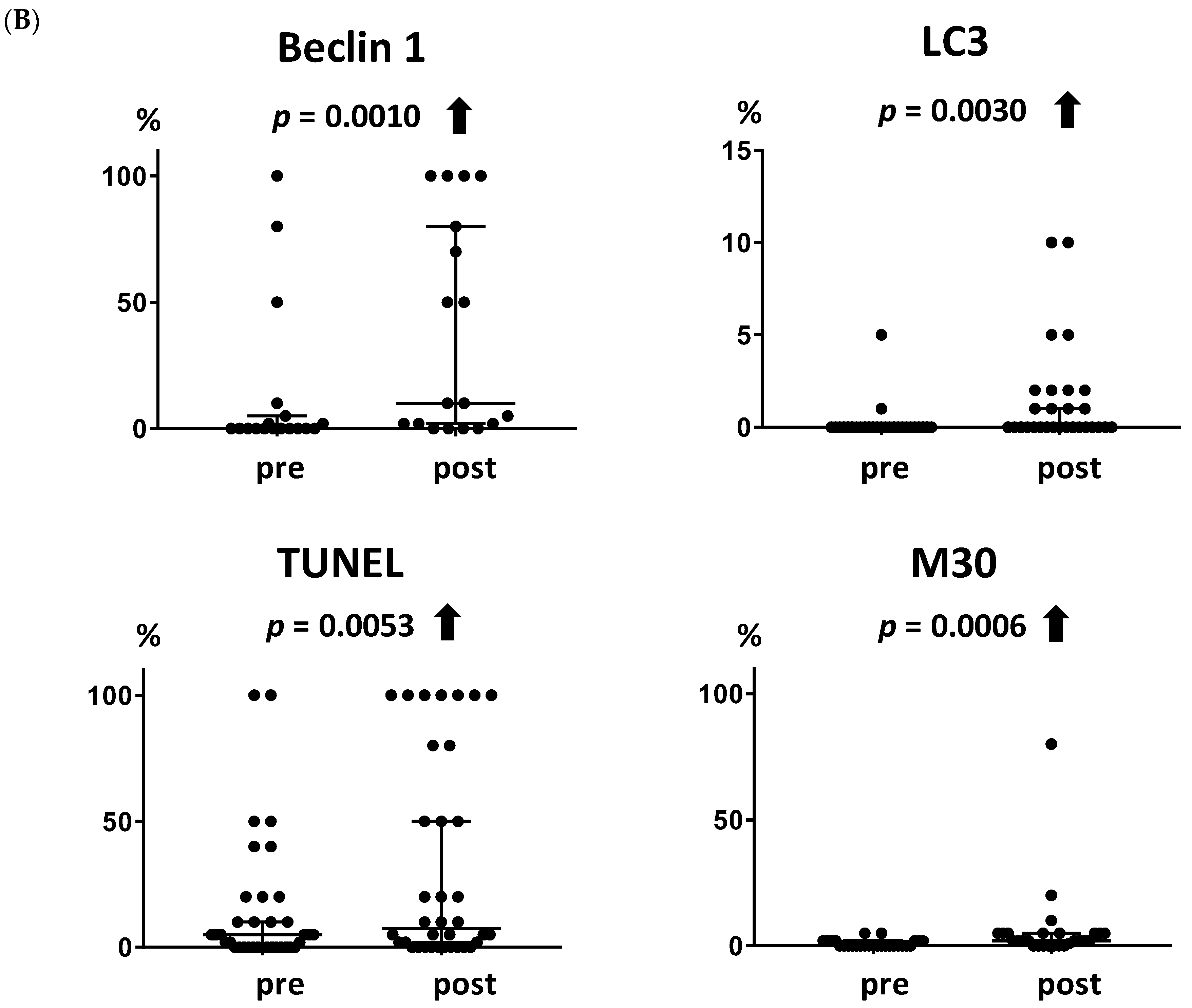
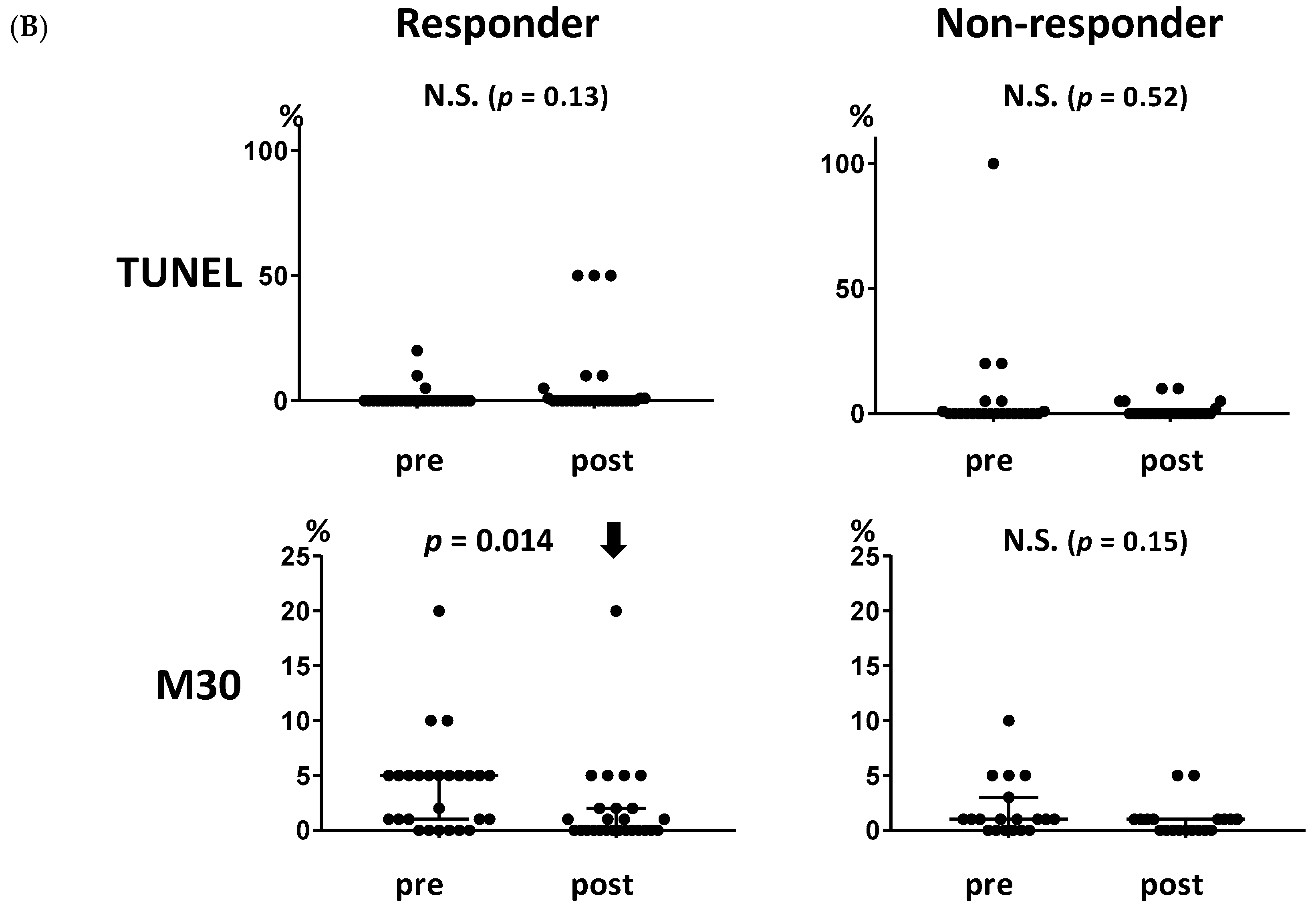
2.1. Induction of Autophagy and Apoptosis by Metronomic Chemoendocrine Therapy
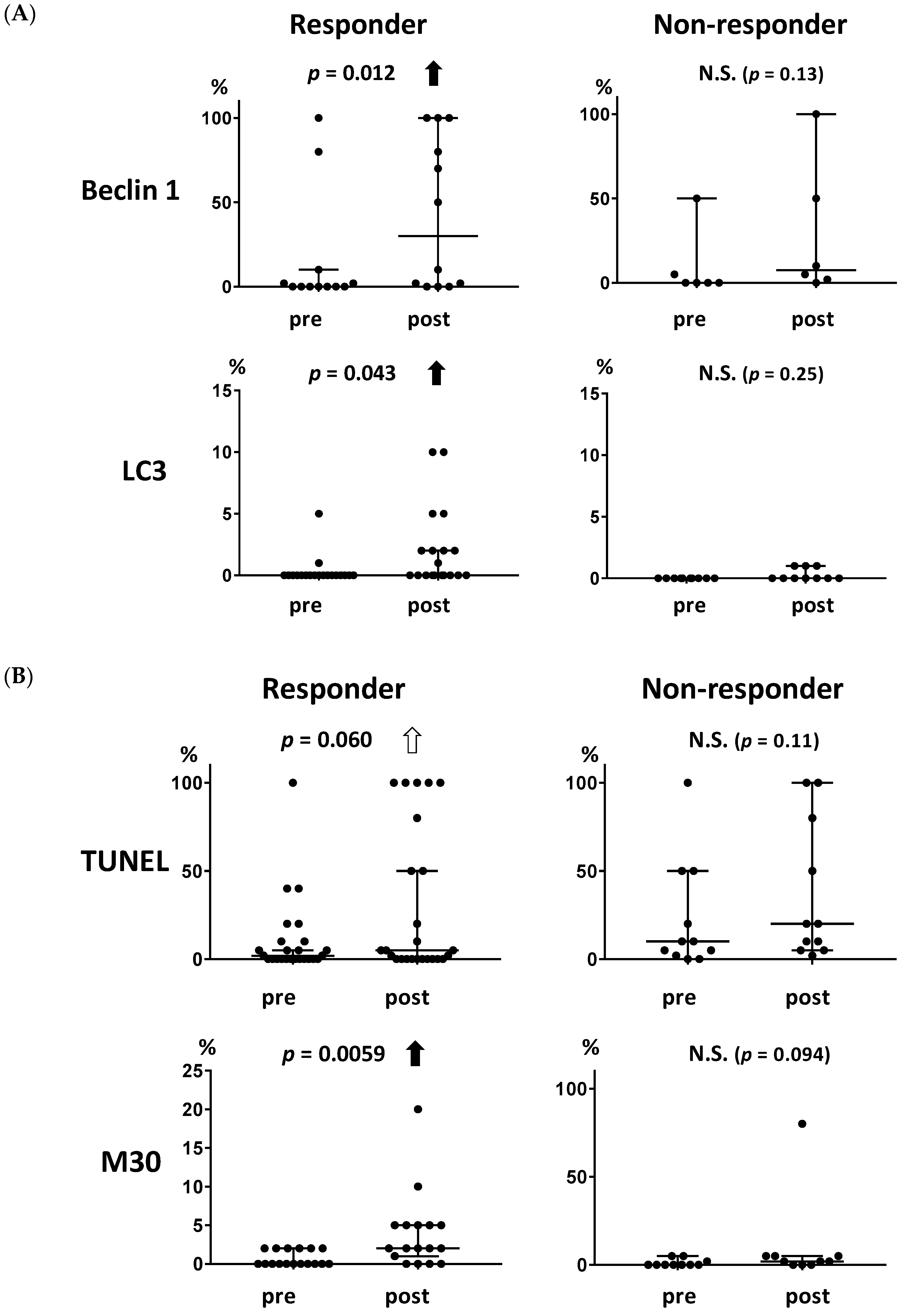
2.2. Association of Autophagy- and Apoptosis-Related Markers with Clinical Response to Metronomic Chemoendocrine Therapy
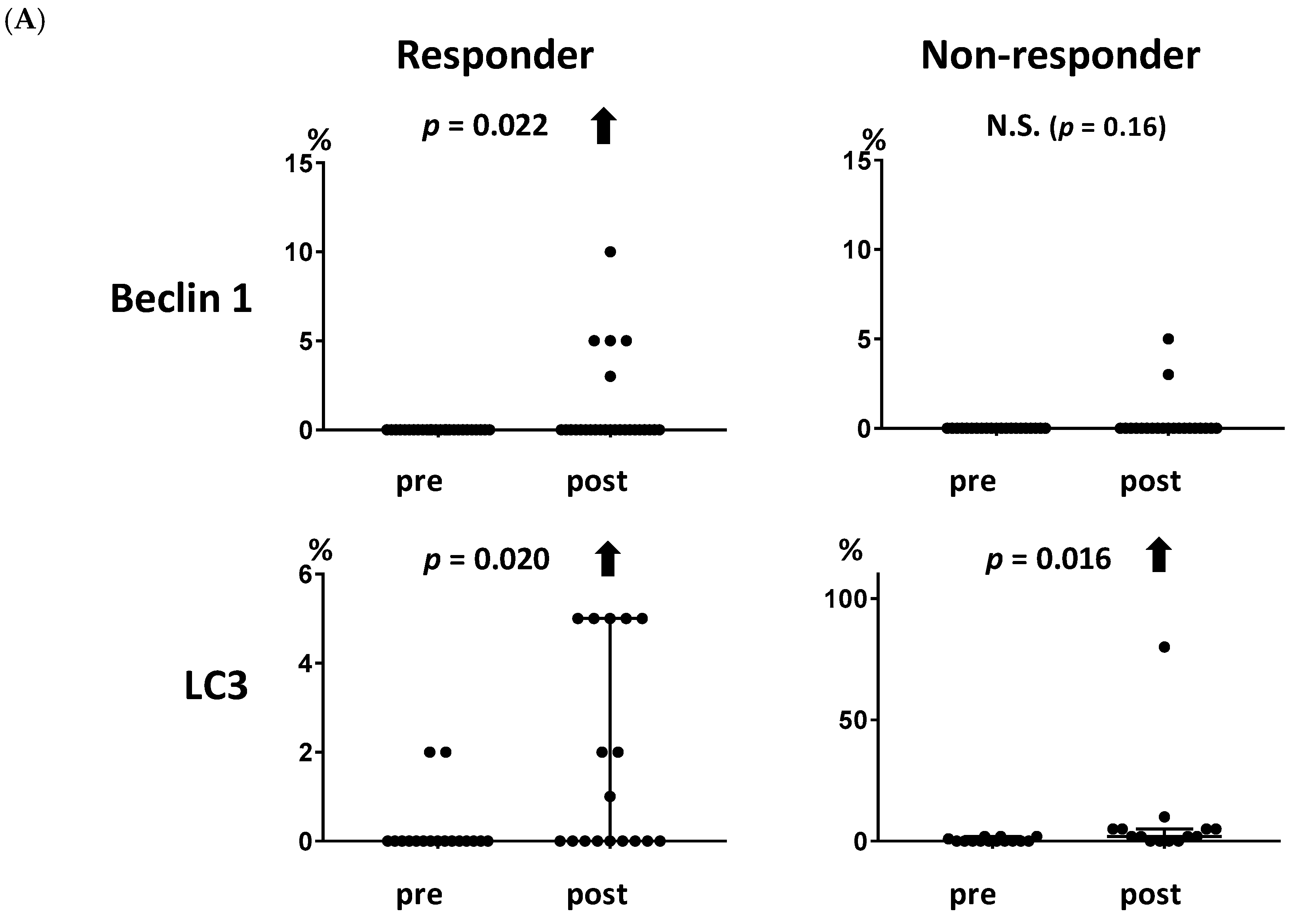
2.3. Association between the Levels of Autophagy- and Apoptosis-Related Markers and the Clinical Response to Endocrine Therapy
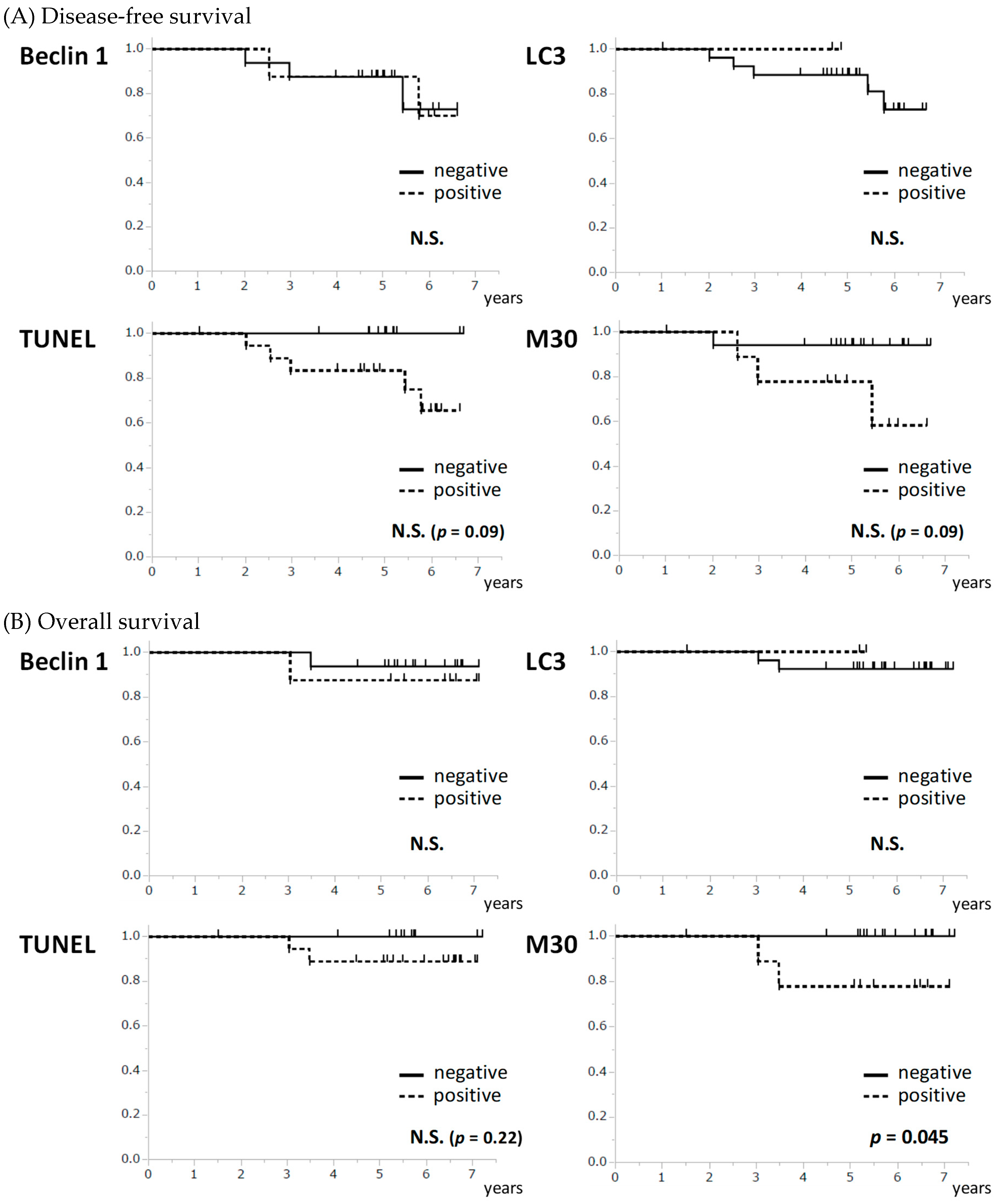
2.4. Association of Autophagy- and Apoptosis-Related Markers with Patients’ Survival
3. Discussion
4. Materials and Methods
4.1. Clinical Trials
4.2. Immunohistochemistry (IHC)
4.3. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CDK | Cyclin-dependent kinase |
| ER | Estrogen receptor |
| HR | Hormone receptor |
| HER2 | Human epidermal growth factor receptor 2 |
| IHC | Immunohistochemistry |
| PD | Progressive disease |
| PgR | Progesterone receptor |
References
- Pan, H.; Gray, R.; Braybrooke, J.; Davies, C.; Taylor, C.; McGale, P.; Peto, R.; Pritchard, K.I.; Bergh, J.; Dowsett, M.; et al. 20-year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years. N. Engl. J. Med. 2017, 377, 1836–1846. [Google Scholar] [CrossRef] [PubMed]
- Davies, C.; Pan, H.; Godwin, J.; Gray, R.; Arriagada, R.; Raina, V.; Abraham, M.; Medeiros Alencar, V.H.; Badran, A.; Bonfill, X.; et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: Atlas, a randomised trial. Lancet 2013, 381, 805–816. [Google Scholar] [CrossRef]
- Baselga, J.; Semiglazov, V.; van Dam, P.; Manikhas, A.; Bellet, M.; Mayordomo, J.; Campone, M.; Kubista, E.; Greil, R.; Bianchi, G.; et al. Phase ii randomized study of neoadjuvant everolimus plus letrozole compared with placebo plus letrozole in patients with estrogen receptor-positive breast cancer. J. Clin. Oncol. 2009, 27, 2630–2637. [Google Scholar] [CrossRef] [PubMed]
- Chow, L.W.C.; Morita, S.; Chow, C.Y.C.; Ng, W.K.; Toi, M. Neoadjuvant palbociclib on ER+ breast cancer (n007): Clinical response and endopredict’s value. Endocr. Relat. Cancer 2018, 25, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Bottini, A.; Generali, D.; Brizzi, M.P.; Fox, S.B.; Bersiga, A.; Bonardi, S.; Allevi, G.; Aguggini, S.; Bodini, G.; Milani, M.; et al. Randomized phase ii trial of letrozole and letrozole plus low-dose metronomic oral cyclophosphamide as primary systemic treatment in elderly breast cancer patients. J. Clin. Oncol. 2006, 24, 3623–3628. [Google Scholar] [CrossRef] [PubMed]
- Andre, N.; Tsai, K.; Carre, M.; Pasquier, E. Metronomic chemotherapy: Direct targeting of cancer cells after all? Trends Cancer 2017, 3, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Browder, T.; Butterfield, C.E.; Kraling, B.M.; Shi, B.; Marshall, B.; O’Reilly, M.S.; Folkman, J. Antiangiogenic scheduling of chemotherapy improves efficacy against experimental drug-resistant cancer. Cancer Res. 2000, 60, 1878–1886. [Google Scholar] [PubMed]
- Andre, N.; Carre, M.; Pasquier, E. Metronomics: Towards personalized chemotherapy? Nat. Rev. Clin. Oncol. 2014, 11, 413–431. [Google Scholar] [CrossRef] [PubMed]
- Bojko, P.; Schimmel, G.; Bosse, D.; Abenhardt, W. Metronomic oral cyclophosphamide in patients with advanced solid tumors. Onkologie 2012, 35, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Gebbia, V.; Boussen, H.; Valerio, M.R. Oral metronomic cyclophosphamide with and without methotrexate as palliative treatment for patients with metastatic breast carcinoma. Anticancer Res. 2012, 32, 529–536. [Google Scholar] [PubMed]
- Wang, Z.; Lu, J.; Leaw, S.; Hong, X.; Wang, J.; Shao, Z.; Hu, X. An all-oral combination of metronomic cyclophosphamide plus capecitabine in patients with anthracycline- and taxane-pretreated metastatic breast cancer: A phase ii study. Cancer Chemother. Pharmacol. 2012, 69, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Yoshimoto, M.; Takao, S.; Hirata, M.; Okamoto, Y.; Yamashita, S.; Kawaguchi, Y.; Takami, M.; Furusawa, H.; Morita, S.; Abe, C.; et al. Metronomic oral combination chemotherapy with capecitabine and cyclophosphamide: A phase ii study in patients with her2-negative metastatic breast cancer. Cancer Chemother. Pharmacol. 2012, 70, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Ueno, T.; Masuda, N.; Kamigaki, S.; Morimoto, T.; Akiyama, F.; Kurosumi, M.; Tsuda, H.; Mikami, Y.; Tanaka, S.; Morita, S.; et al. A multicenter phase ii trial of neoadjuvant letrozole plus low-dose cyclophosphamide in postmenopausal patients with estrogen receptor-positive breast cancer (jbcrg-07): Therapeutic efficacy and clinical implications of circulating endothelial cells. Cancer Med. 2018, 7, 2442–2451. [Google Scholar] [CrossRef] [PubMed]
- Sato, N.; Masuda, N.; Morimoto, T.; Ueno, T.; Kanbayashi, C.; Kaneko, K.; Yasojima, H.; Saji, S.; Sasano, H.; Morita, S.; et al. Neoadjuvant endocrine therapy with exemestane followed by response-guided combination therapy with low-dose cyclophosphamide in postmenopausal patients with estrogen receptor-positive breast cancer: A multicenter, open-label, phase ii study. Cancer Med. 2018, 7, 3044–3056. [Google Scholar] [CrossRef] [PubMed]
- Osborne, C.K.; Hobbs, K.; Clark, G.M. Effect of estrogens and antiestrogens on growth of human breast cancer cells in athymic nude mice. Cancer Res. 1985, 45, 584–590. [Google Scholar] [PubMed]
- Dowsett, M.; Smith, I.E.; Ebbs, S.R.; Dixon, J.M.; Skene, A.; Griffith, C.; Boeddinghaus, I.; Salter, J.; Detre, S.; Hills, M.; et al. Short-term changes in ki-67 during neoadjuvant treatment of primary breast cancer with anastrozole or tamoxifen alone or combined correlate with recurrence-free survival. Clin. Cancer Res. 2005, 11, 951s–958s. [Google Scholar] [PubMed]
- Ueno, T.; Saji, S.; Sugimoto, M.; Masuda, N.; Kuroi, K.; Sato, N.; Takei, H.; Yamamoto, Y.; Ohno, S.; Yamashita, H.; et al. Clinical significance of the expression of autophagy-associated marker, beclin 1, in breast cancer patients who received neoadjuvant endocrine therapy. BMC Cancer 2016, 16, 230. [Google Scholar] [CrossRef] [PubMed]
- Amaral, C.; Borges, M.; Melo, S.; da Silva, E.T.; Correia-da-Silva, G.; Teixeira, N. Apoptosis and autophagy in breast cancer cells following exemestane treatment. PLoS ONE 2012, 7, e42398. [Google Scholar] [CrossRef] [PubMed]
- Amaral, C.; Varela, C.; Azevedo, M.; da Silva, E.T.; Roleira, F.M.; Chen, S.; Correia-da-Silva, G.; Teixeira, N. Effects of steroidal aromatase inhibitors on sensitive and resistant breast cancer cells: Aromatase inhibition and autophagy. J. Steroid Biochem. Mol. Biol. 2013, 135, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Ellis, P.A.; Smith, I.E.; Detre, S.; Burton, S.A.; Salter, J.; A’Hern, R.; Walsh, G.; Johnston, S.R.; Dowsett, M. Reduced apoptosis and proliferation and increased bcl-2 in residual breast cancer following preoperative chemotherapy. Breast Cancer Res. Treat. 1998, 48, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Parton, M.; Krajewski, S.; Smith, I.; Krajewska, M.; Archer, C.; Naito, M.; Ahern, R.; Reed, J.; Dowsett, M. Coordinate expression of apoptosis-associated proteins in human breast cancer before and during chemotherapy. Clin. Cancer Res. 2002, 8, 2100–2108. [Google Scholar] [PubMed]
- Van Slooten, H.J.; van de Vijver, M.J.; van de Velde, C.J.; van Dierendonck, J.H. Loss of bcl-2 in invasive breast cancer is associated with high rates of cell death, but also with increased proliferative activity. Br. J. Cancer 1998, 77, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Rogov, V.; Dotsch, V.; Johansen, T.; Kirkin, V. Interactions between autophagy receptors and ubiquitin-like proteins form the molecular basis for selective autophagy. Mol. Cell 2014, 53, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Schlafli, A.M.; Berezowska, S.; Adams, O.; Langer, R.; Tschan, M.P. Reliable lc3 and p62 autophagy marker detection in formalin fixed paraffin embedded human tissue by immunohistochemistry. Eur. J. Histochem. 2015, 59, 2481. [Google Scholar] [CrossRef] [PubMed]
- Kyrylkova, K.; Kyryachenko, S.; Leid, M.; Kioussi, C. Detection of apoptosis by tunel assay. Meth. Mol. Biol. 2012, 887, 41–47. [Google Scholar]
- Duan, W.R.; Garner, D.S.; Williams, S.D.; Funckes-Shippy, C.L.; Spath, I.S.; Blomme, E.A. Comparison of immunohistochemistry for activated caspase-3 and cleaved cytokeratin 18 with the tunel method for quantification of apoptosis in histological sections of pc-3 subcutaneous xenografts. J. Pathol. 2003, 199, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Kramer, G.; Erdal, H.; Mertens, H.J.; Nap, M.; Mauermann, J.; Steiner, G.; Marberger, M.; Biven, K.; Shoshan, M.C.; Linder, S. Differentiation between cell death modes using measurements of different soluble forms of extracellular cytokeratin 18. Cancer Res. 2004, 64, 1751–1756. [Google Scholar] [CrossRef] [PubMed]
- Ueno, T.; Toi, M.; Linder, S. Detection of epithelial cell death in the body by cytokeratin 18 measurement. Biomed. Pharmacother 2005, 59, S359–S362. [Google Scholar] [CrossRef]
- Lipponen, P. Apoptosis in breast cancer: Relationship with other pathological parameters. Endocr. Relat. Cancer 1999, 6, 13–16. [Google Scholar] [PubMed]
- He, Y.; Zhao, X.; Subahan, N.R.; Fan, L.; Gao, J.; Chen, H. The prognostic value of autophagy-related markers beclin-1 and microtubule-associated protein light chain 3b in cancers: A systematic review and meta-analysis. Tumour Biol. 2014, 35, 7317–7326. [Google Scholar] [CrossRef] [PubMed]
- Takada, M.; Saji, S.; Masuda, N.; Kuroi, K.; Sato, N.; Takei, H.; Yamamoto, Y.; Ohno, S.; Yamashita, H.; Hisamatsu, K.; et al. Relationship between body mass index and preoperative treatment response to aromatase inhibitor exemestane in postmenopausal patients with primary breast cancer. Breast 2012, 21, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Toi, M.; Saji, S.; Masuda, N.; Kuroi, K.; Sato, N.; Takei, H.; Yamamoto, Y.; Ohno, S.; Yamashita, H.; Hisamatsu, K.; et al. Ki67 index changes, pathological response and clinical benefits in primary breast cancer patients treated with 24 weeks of aromatase inhibition. Cancer Sci. 2011, 102, 858–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueno, T.; Masuda, N.; Yamanaka, T.; Saji, S.; Kuroi, K.; Sato, N.; Takei, H.; Yamamoto, Y.; Ohno, S.; Yamashita, H.; et al. Evaluating the 21-gene assay recurrence score(r) as a predictor of clinical response to 24 weeks of neoadjuvant exemestane in estrogen receptor-positive breast cancer. Int. J. Clin. Oncol. 2014, 19, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Ueno, T.; Saji, S.; Masuda, N.; Kuroi, K.; Sato, N.; Takei, H.; Yamamoto, Y.; Ohno, S.; Yamashita, H.; Hisamatsu, K.; et al. Impact of clinical response to neoadjuvant endocrine therapy on patient outcomes: A follow-up study of jfmc34-0601 multicentre prospective neoadjuvant endocrine trial. ESMO Open 2018, 3, e000314. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Subgroup | Number |
|---|---|---|
| Number of patients | 38 | |
| Average age (range) | 69.7 (57–82) | |
| T | T1 | 1 |
| T2 | 33 | |
| T3 | 4 | |
| N | N0 | 33 |
| N1 | 5 | |
| ER | + | 38 |
| − | 0 | |
| PgR | + | 24 |
| − | 14 | |
| HER2 | + | 8 |
| − | 30 | |
| Histological grade | 1 | 13 |
| 2 | 25 | |
| 3 | 0 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ueno, T.; Masuda, N.; Kamigaki, S.; Morimoto, T.; Saji, S.; Imoto, S.; Sasano, H.; Toi, M. Differential Involvement of Autophagy and Apoptosis in Response to Chemoendocrine and Endocrine Therapy in Breast Cancer: JBCRG-07TR. Int. J. Mol. Sci. 2019, 20, 984. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20040984
Ueno T, Masuda N, Kamigaki S, Morimoto T, Saji S, Imoto S, Sasano H, Toi M. Differential Involvement of Autophagy and Apoptosis in Response to Chemoendocrine and Endocrine Therapy in Breast Cancer: JBCRG-07TR. International Journal of Molecular Sciences. 2019; 20(4):984. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20040984
Chicago/Turabian StyleUeno, Takayuki, Norikazu Masuda, Shunji Kamigaki, Takashi Morimoto, Shigehira Saji, Shigeru Imoto, Hironobu Sasano, and Masakazu Toi. 2019. "Differential Involvement of Autophagy and Apoptosis in Response to Chemoendocrine and Endocrine Therapy in Breast Cancer: JBCRG-07TR" International Journal of Molecular Sciences 20, no. 4: 984. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20040984