Serum Chemerin Does Not Differentiate Colorectal Liver Metastases from Hepatocellular Carcinoma


Abstract
:1. Introduction
2. Results
2.1. Association of Chemerin with Gender, Age and BMI
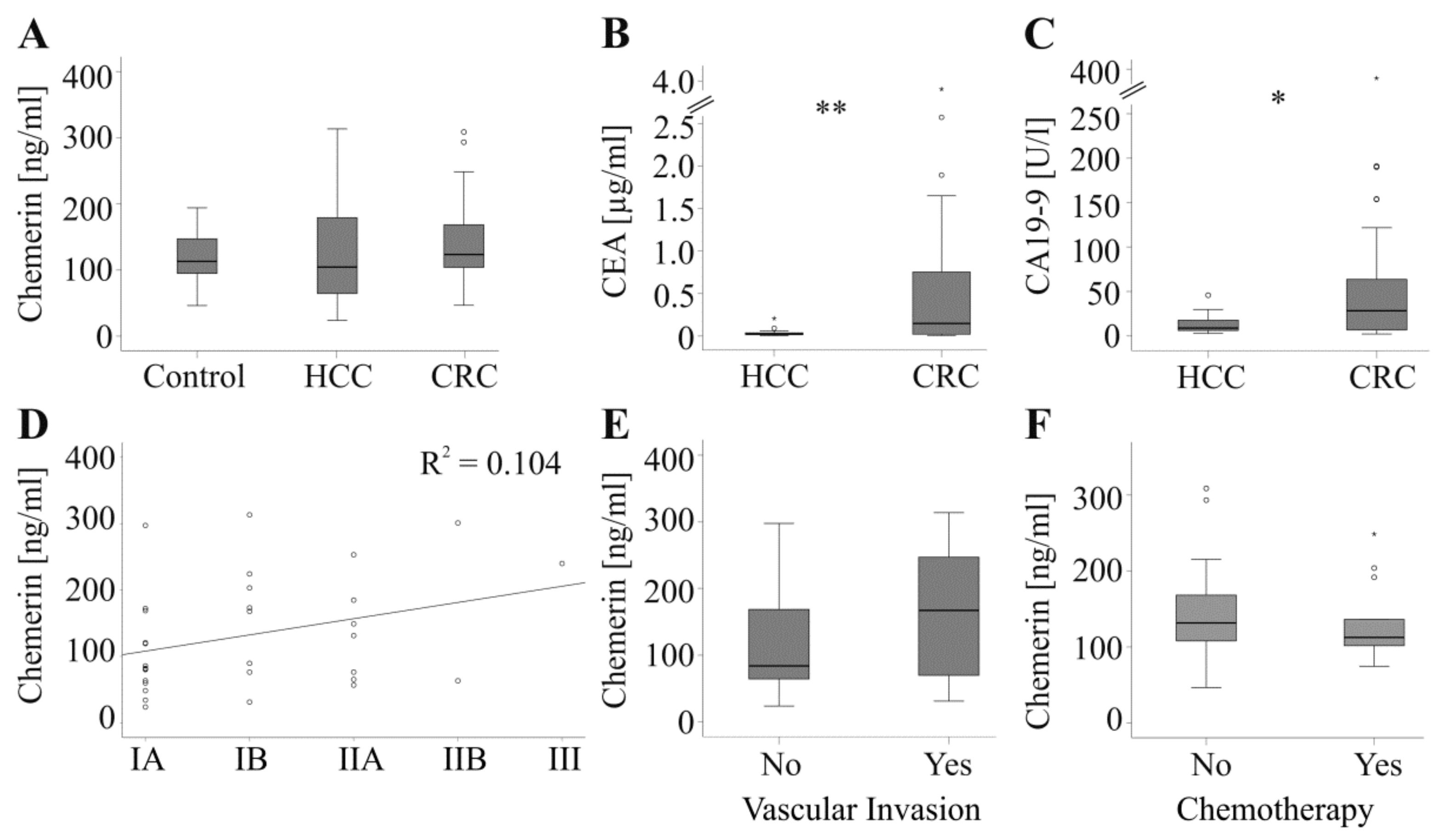
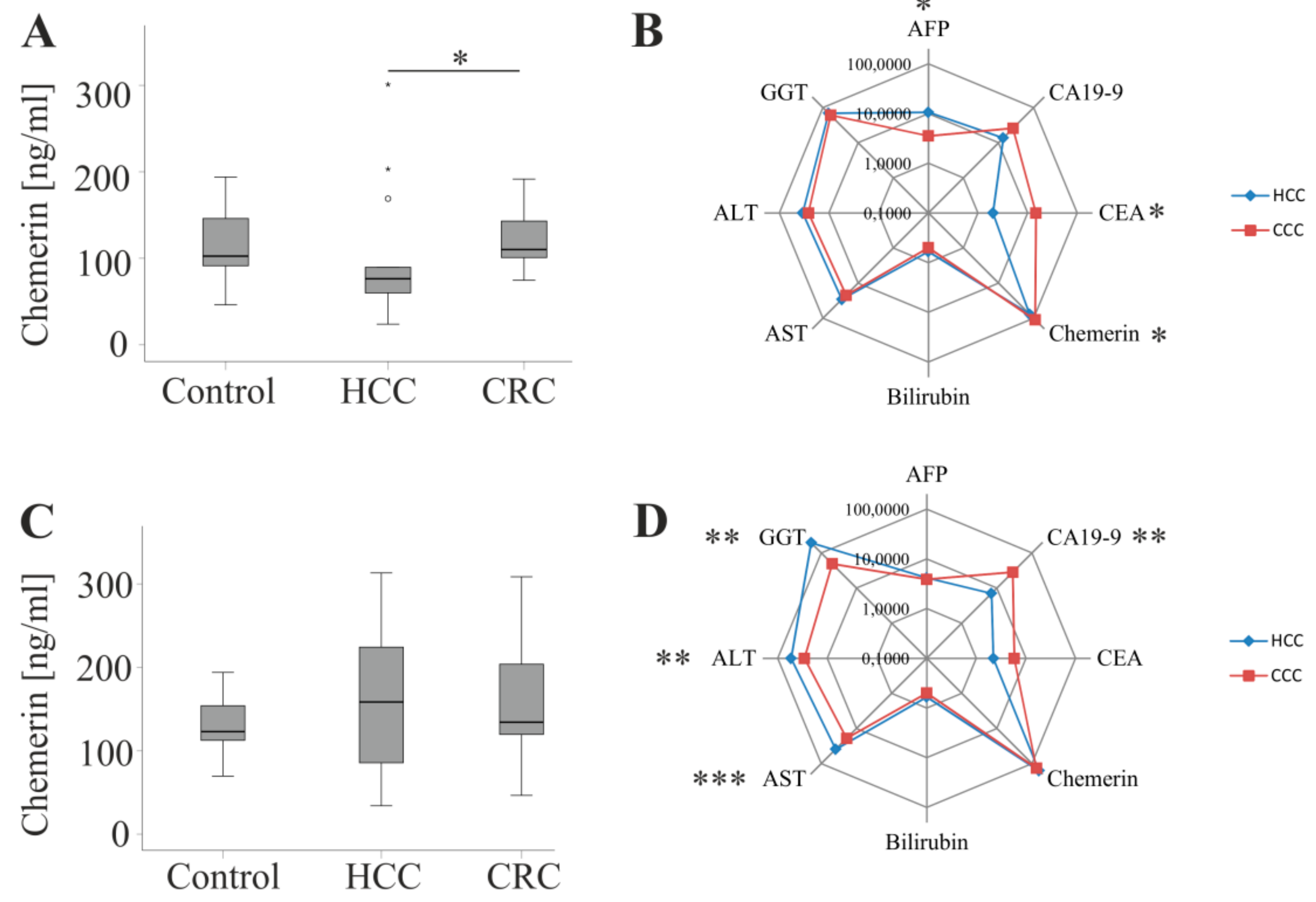
2.2. Chemerin, CEA and CA19-9 in HCC and CRC Patients
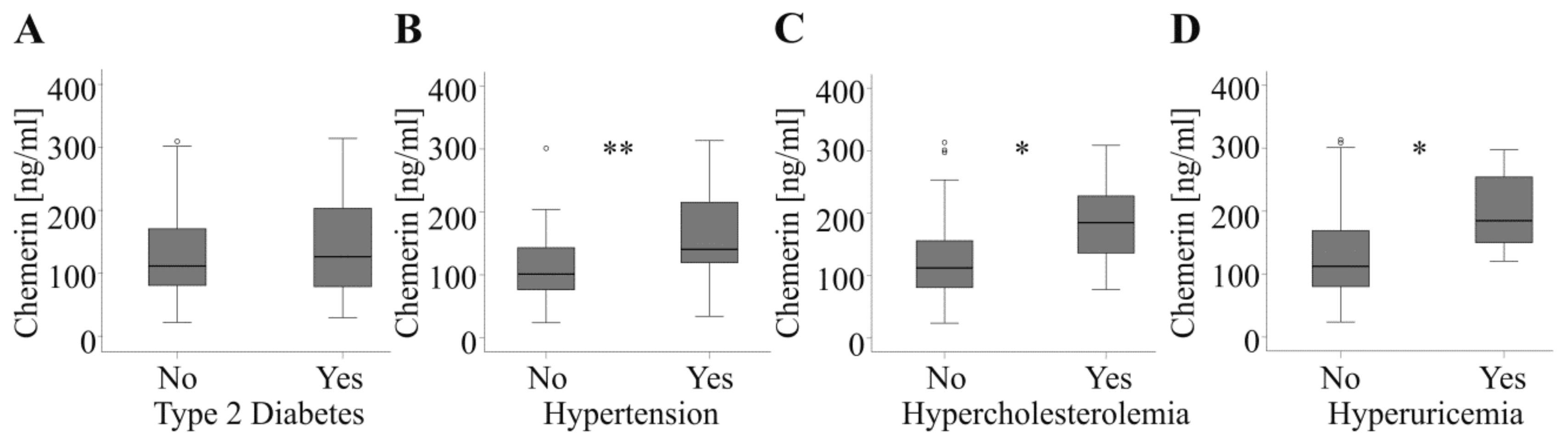
2.3. Association of Chemerin with Type 2 Diabetes, Hypertension, Hypercholesterolemia and Hyperuricemia
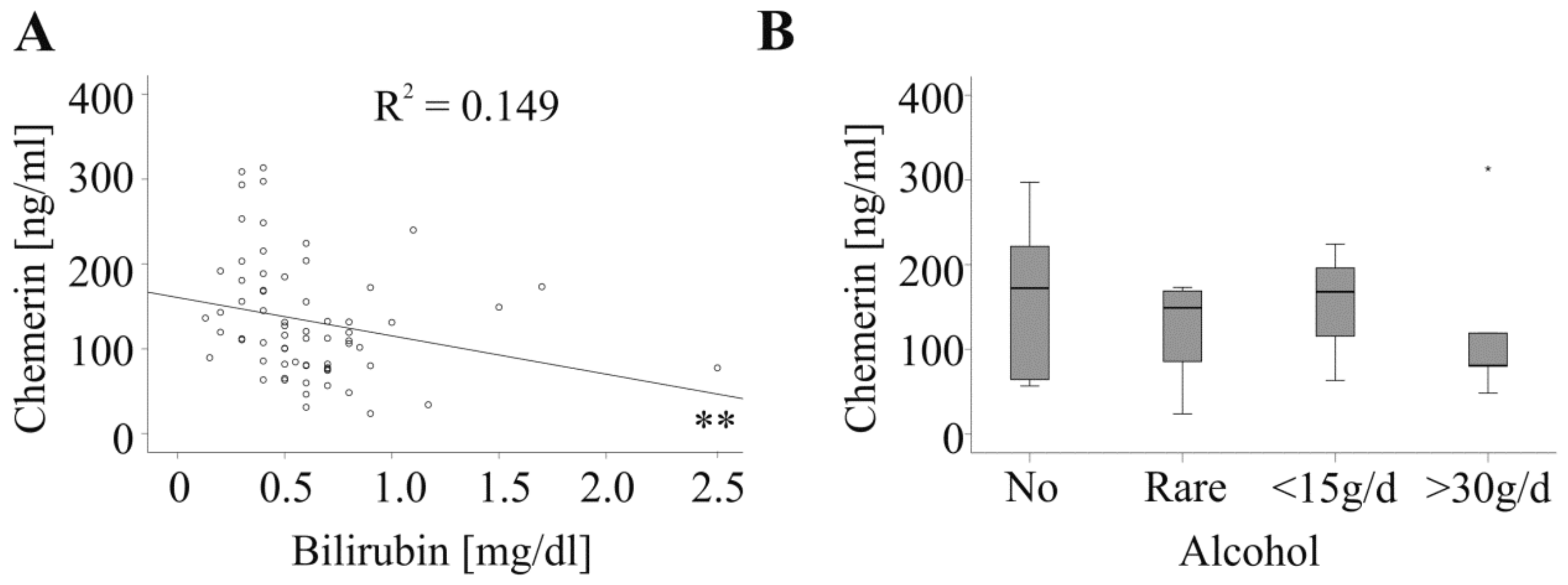
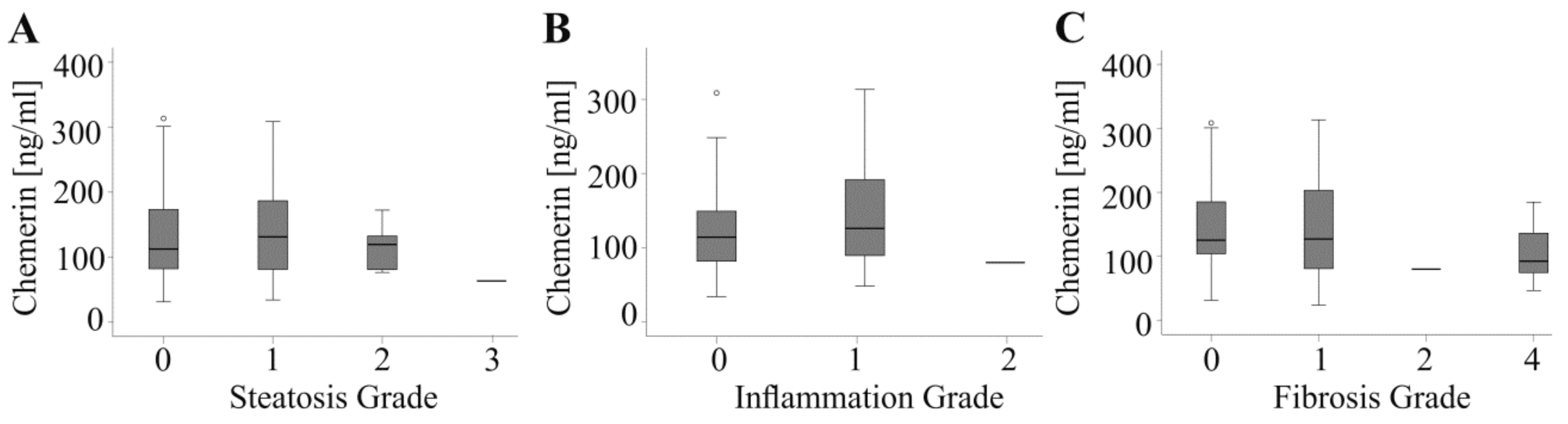
2.4. Association of Chemerin with Liver Dysfunction
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Chemerin ELISA
4.3. Laboratory Values
4.4. Statistics
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ALT | alanine aminotransferase |
| AFP | alpha-fetoprotein |
| AST | aspartate aminotransferase |
| BMI | body mass index |
| CA19-9 | cancer antigen 19-9 |
| CEA | carcinoembryonic antigen |
| CRC | colorectal cancer |
| GGT | γ-glutamyltransferase |
| HCC | hepatocellular carcinoma |
| NAFLD | non-alcoholic fatty liver disease |
| NASH | non-alcoholic steatohepatitis |
| TNM | tumor-node-metastasis |
References
- Abdel-Hamid, N.M.; Abouzied, M.M.; Nazmy, M.H.; Fawzy, M.A.; Gerges, A.S. A suggested guiding panel of seromarkers for efficient discrimination between primary and secondary human hepatocarcinoma. Tumour Biol. 2016, 37, 2539–2546. [Google Scholar] [CrossRef] [PubMed]
- Attallah, A.M.; Al-Ghawalby, N.A.; Aziz, A.A.; El-Sayed, E.A.; Tabll, A.A.; El-Waseef, A.M. Clinical value of serum CEA, CA 19-9, CA 242 and AFP in diagnosis of gastrointestinal tract cancer. Int. J. Cancer Res. 2006, 2, 50–56. [Google Scholar]
- Desai, A.; Sandhu, S.; Lai, J.P.; Sandhu, D.S. Hepatocellular carcinoma in non-cirrhotic liver: A comprehensive review. World J. Hepatol. 2019, 11, 1–18. [Google Scholar] [CrossRef]
- Gozde, A.E.I. Evaluation of Hepatocellular Carcinomas and Liver Metastases––How Far can we Go with Diffusion Weighted Imaging? J. Nucl. Med. Radiat. Ther. 2017, 8, 1–4. [Google Scholar]
- Campos-da-Paz, M.; Dorea, J.G.; Galdino, A.S.; Lacava, Z.G.M.; de Fatima Menezes Almeida Santos, M. Carcinoembryonic Antigen (CEA) and Hepatic Metastasis in Colorectal Cancer: Update on Biomarker for Clinical and Biotechnological Approaches. Recent Pat. Biotechnol. 2018, 12, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.K.; Kim, H.C.; Lee, W.Y.; Yun, S.H.; Cho, Y.B.; Huh, J.W.; Park, Y.A.; Chun, H.K. High preoperative serum CA 19-9 levels can predict poor oncologic outcomes in colorectal cancer patients on propensity score analysis. Ann. Surg. Treat. Res. 2019, 96, 107–115. [Google Scholar] [CrossRef]
- Alkady, M.M.; Abdel-Messeih, P.L.; Nosseir, N.M. Assessment of Serum Levels of the Adipocytokine Chemerin in Colorectal Cancer Patients. J. Med. Biochem. 2018, 37, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Eichelmann, F.; Schulze, M.B.; Wittenbecher, C.; Menzel, J.; Weikert, C.; di Giuseppe, R.; Biemann, R.; Isermann, B.; Fritsche, A.; Boeing, H.; et al. Association of Chemerin Plasma Concentration With Risk of Colorectal Cancer. JAMA Netw. Open 2019, 2, e190896. [Google Scholar] [CrossRef]
- Erdogan, S.; Yilmaz, F.M.; Yazici, O.; Yozgat, A.; Sezer, S.; Ozdemir, N.; Uysal, S.; Purnak, T.; Sendur, M.A.; Ozaslan, E. Inflammation and chemerin in colorectal cancer. Tumour Biol. 2016, 37, 6337–6342. [Google Scholar] [CrossRef]
- Ernst, M.C.; Sinal, C.J. Chemerin: At the crossroads of inflammation and obesity. Trends Endocrinol. Metab. 2010, 21, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Parolini, S.; Santoro, A.; Marcenaro, E.; Luini, W.; Massardi, L.; Facchetti, F.; Communi, D.; Parmentier, M.; Majorana, A.; Sironi, M.; et al. The role of chemerin in the colocalization of NK and dendritic cell subsets into inflamed tissues. Blood 2007, 109, 3625–3632. [Google Scholar] [CrossRef]
- Buechler, C.; Feder, S.; Haberl, E.M.; Aslanidis, C. Chemerin Isoforms and Activity in Obesity. Int. J. Mol. Sci. 2019, 20, 1128. [Google Scholar] [CrossRef]
- Pachynski, R.K.; Zabel, B.A.; Kohrt, H.E.; Tejeda, N.M.; Monnier, J.; Swanson, C.D.; Holzer, A.K.; Gentles, A.J.; Sperinde, G.V.; Edalati, A.; et al. The chemoattractant chemerin suppresses melanoma by recruiting natural killer cell antitumor defenses. J. Exp. Med. 2012, 209, 1427–1435. [Google Scholar] [CrossRef]
- Yagi, M.; Sasaki, Y.; Abe, Y.; Yaoita, T.; Sakuta, K.; Mizumoto, N.; Shoji, M.; Onozato, Y.; Kon, T.; Nishise, S.; et al. Association between High Levels of Circulating Chemerin and Colorectal Adenoma in Men. Digestion 2019, 1–8. [Google Scholar] [CrossRef]
- Lin, W.; Chen, Y.L.; Jiang, L.; Chen, J.K. Reduced expression of chemerin is associated with a poor prognosis and a lowed infiltration of both dendritic cells and natural killer cells in human hepatocellular carcinoma. Clin. Lab. 2011, 57, 879–885. [Google Scholar]
- Lin, Y.; Yang, X.; Liu, W.; Li, B.; Yin, W.; Shi, Y.; He, R. Chemerin has a protective role in hepatocellular carcinoma by inhibiting the expression of IL-6 and GM-CSF and MDSC accumulation. Oncogene 2017, 36, 3599–3608. [Google Scholar] [CrossRef]
- Imai, K.; Takai, K.; Hanai, T.; Shiraki, M.; Suzuki, Y.; Hayashi, H.; Naiki, T.; Nishigaki, Y.; Tomita, E.; Shimizu, M.; et al. Impact of serum chemerin levels on liver functional reserves and platelet counts in patients with hepatocellular carcinoma. Int. J. Mol. Sci. 2014, 15, 11294–11306. [Google Scholar] [CrossRef]
- Buechler, C.; Haberl, E.M.; Rein-Fischboeck, L.; Aslanidis, C. Adipokines in Liver Cirrhosis. Int J. Mol. Sci. 2017, 18, 1392. [Google Scholar] [CrossRef]
- Kukla, M.; Zwirska-Korczala, K.; Gabriel, A.; Waluga, M.; Warakomska, I.; Szczygiel, B.; Berdowska, A.; Mazur, W.; Wozniak-Grygiel, E.; Kryczka, W. Chemerin, vaspin and insulin resistance in chronic hepatitis C. J. Viral. Hepat. 2010, 17, 661–667. [Google Scholar] [CrossRef]
- Ren, R.Z.; Zhang, X.; Xu, J.; Zhang, H.Q.; Yu, C.X.; Cao, M.F.; Gao, L.; Guan, Q.B.; Zhao, J.J. Chronic ethanol consumption increases the levels of chemerin in the serum and adipose tissue of humans and rats. Acta Pharm. Sin. 2012, 33, 652–659. [Google Scholar] [CrossRef] [Green Version]
- Buechler, C. Chemerin in Liver Diseases. Endocrinol. Metab. Syndr. 2014, 3, 1–6. [Google Scholar]
- Uzunlulu, M.; Telci Caklili, O.; Oguz, A. Association between Metabolic Syndrome and Cancer. Ann. Nutr. Metab. 2016, 68, 173–179. [Google Scholar] [CrossRef]
- Sanna, C.; Rosso, C.; Marietti, M.; Bugianesi, E. Non-Alcoholic Fatty Liver Disease and Extra-Hepatic Cancers. Int J. Mol. Sci. 2016, 17, 717. [Google Scholar] [CrossRef]
- Bozaoglu, K.; Bolton, K.; McMillan, J.; Zimmet, P.; Jowett, J.; Collier, G.; Walder, K.; Segal, D. Chemerin is a novel adipokine associated with obesity and metabolic syndrome. Endocrinology 2007, 148, 4687–4694. [Google Scholar] [CrossRef]
- Zylla, S.; Pietzner, M.; Kuhn, J.P.; Volzke, H.; Dorr, M.; Nauck, M.; Friedrich, N. Serum chemerin is associated with inflammatory and metabolic parameters-results of a population-based study. Obesty 2017, 25, 468–475. [Google Scholar] [CrossRef] [Green Version]
- Milette, S.; Sicklick, J.K.; Lowy, A.M.; Brodt, P. Molecular Pathways: Targeting the Microenvironment of Liver Metastases. Clin. Cancer Res. 2017, 23, 6390–6399. [Google Scholar] [CrossRef] [Green Version]
- Bauer, S.; Weiss, T.S.; Wiest, R.; Schacherer, D.; Hellerbrand, C.; Farkas, S.; Scherer, M.N.; Ritter, M.; Schmitz, G.; Schaffler, A.; et al. Soluble CD163 is not increased in visceral fat and steatotic liver and is even suppressed by free fatty acids in vitro. Exp. Mol. Pathol. 2011, 91, 733–739. [Google Scholar] [CrossRef]
- Pohl, R.; Haberl, E.M.; Rein-Fischboeck, L.; Zimny, S.; Neumann, M.; Aslanidis, C.; Schacherer, D.; Krautbauer, S.; Eisinger, K.; Weiss, T.S.; et al. Hepatic chemerin mRNA expression is reduced in human nonalcoholic steatohepatitis. Eur. J. Clin. Invest. 2017, 47, 7–18. [Google Scholar] [CrossRef]
- Yamashita, S.; Sakamoto, Y.; Yamamoto, S.; Takemura, N.; Omichi, K.; Shinkawa, H.; Mori, K.; Kaneko, J.; Akamatsu, N.; Arita, J.; et al. Efficacy of Preoperative Portal Vein Embolization Among Patients with Hepatocellular Carcinoma, Biliary Tract Cancer, and Colorectal Liver Metastases: A Comparative Study Based on Single-Center Experience of 319 Cases. Ann. Surg. Oncol. 2017, 24, 1557–1568. [Google Scholar] [CrossRef]
- Rourke, J.L.; Dranse, H.J.; Sinal, C.J. Towards an integrative approach to understanding the role of chemerin in human health and disease. Obes Rev. 2013, 14, 245–262. [Google Scholar] [CrossRef]
- Weigert, J.; Neumeier, M.; Wanninger, J.; Filarsky, M.; Bauer, S.; Wiest, R.; Farkas, S.; Scherer, M.N.; Schaffler, A.; Aslanidis, C.; et al. Systemic chemerin is related to inflammation rather than obesity in type 2 diabetes. Clin. Endocrinol. 2010, 72, 342–348. [Google Scholar] [CrossRef]
- Boyuk, B.; Guzel, E.C.; Atalay, H.; Guzel, S.; Mutlu, L.C.; Kucukyalcin, V. Relationship between plasma chemerin levels and disease severity in COPD patients. Clin. Respir. J. 2015, 9, 468–474. [Google Scholar] [CrossRef]
- Gisondi, P.; Lora, V.; Bonauguri, C.; Russo, A.; Lippi, G.; Girolomoni, G. Serum chemerin is increased in patients with chronic plaque psoriasis and normalizes following treatment with infliximab. Br. J. Derm. 2013, 168, 749–755. [Google Scholar] [CrossRef]
- Weigert, J.; Obermeier, F.; Neumeier, M.; Wanninger, J.; Filarsky, M.; Bauer, S.; Aslanidis, C.; Rogler, G.; Ott, C.; Schaffler, A.; et al. Circulating levels of chemerin and adiponectin are higher in ulcerative colitis and chemerin is elevated in Crohn’s disease. Inflamm. Bowel Dis. 2010, 16, 630–637. [Google Scholar] [CrossRef]
- Motawi, T.M.K.; Mahdy, S.G.; El-Sawalhi, M.M.; Ali, E.N.; El-Telbany, R.F.A. Serum levels of chemerin, apelin, vaspin, and omentin-1 in obese type 2 diabetic Egyptian patients with coronary artery stenosis. Can. J. Physiol. Pharm. 2018, 96, 38–44. [Google Scholar] [CrossRef]
- Feng, X.; Li, P.; Zhou, C.; Jia, X.; Kang, J. Elevated levels of serum chemerin in patients with obstructive sleep apnea syndrome. Biomarkers 2012, 17, 248–253. [Google Scholar] [CrossRef]
- Liu-Chittenden, Y.; Patel, D.; Gaskins, K.; Giordano, T.J.; Assie, G.; Bertherat, J.; Kebebew, E. Serum RARRES2 Is a Prognostic Marker in Patients With Adrenocortical Carcinoma. J. Clin. Endocrinol. Metab. 2016, 101, 3345–3352. [Google Scholar] [CrossRef] [Green Version]
- Parlee, S.D.; Ernst, M.C.; Muruganandan, S.; Sinal, C.J.; Goralski, K.B. Serum chemerin levels vary with time of day and are modified by obesity and tumor necrosis factor-alpha. Endocrinology 2010, 151, 2590–2602. [Google Scholar] [CrossRef]
- Bauer, S.; Wanninger, J.; Schmidhofer, S.; Weigert, J.; Neumeier, M.; Dorn, C.; Hellerbrand, C.; Zimara, N.; Schaffler, A.; Aslanidis, C.; et al. Sterol regulatory element-binding protein 2 (SREBP2) activation after excess triglyceride storage induces Chemerin in hypertrophic adipocytes. Endocrinology 2011, 152, 26–35. [Google Scholar] [CrossRef]
- Toulany, J.; Parlee, S.D.; Sinal, C.J.; Slayter, K.; McNeil, S.; Goralski, K.B. CMKLR1 activation ex vivo does not increase proportionally to serum total chemerin in obese humans. Endocr Connect. 2016, 5, 70–81. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.S.; Eisenberg, D.; Zhao, L.; Adams, C.; Leib, R.; Morser, J.; Leung, L. Chemerin activation in human obesity. Obesty 2016, 24, 1522–1529. [Google Scholar] [CrossRef] [Green Version]
- Mattern, A.; Zellmann, T.; Beck-Sickinger, A.G. Processing, signaling, and physiological function of chemerin. IUBMB Life 2014, 66, 19–26. [Google Scholar] [CrossRef]
- Eisinger, K.; Krautbauer, S.; Wiest, R.; Weiss, T.S.; Buechler, C. Reduced serum chemerin in patients with more severe liver cirrhosis. Exp. Mol. Pathol. 2015, 98, 208–213. [Google Scholar] [CrossRef]
- Kukla, M.; Zwirska-Korczala, K.; Hartleb, M.; Waluga, M.; Chwist, A.; Kajor, M.; Ciupinska-Kajor, M.; Berdowska, A.; Wozniak-Grygiel, E.; Buldak, R. Serum chemerin and vaspin in non-alcoholic fatty liver disease. Scand. J. Gastroenterol. 2010, 45, 235–242. [Google Scholar] [CrossRef]
- Kajor, M.; Kukla, M.; Waluga, M.; Liszka, L.; Dyaczynski, M.; Kowalski, G.; Zadlo, D.; Berdowska, A.; Chapula, M.; Kostrzab-Zdebel, A.; et al. Hepatic chemerin mRNA in morbidly obese patients with nonalcoholic fatty liver disease. Pol. J. Pathol. 2017, 68, 117–127. [Google Scholar] [CrossRef]
- Sell, H.; Divoux, A.; Poitou, C.; Basdevant, A.; Bouillot, J.L.; Bedossa, P.; Tordjman, J.; Eckel, J.; Clement, K. Chemerin correlates with markers for fatty liver in morbidly obese patients and strongly decreases after weight loss induced by bariatric surgery. J. Clin. Endocrinol. Metab. 2010, 95, 2892–2896. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef]
- Kinoshita, A.; Onoda, H.; Fushiya, N.; Koike, K.; Nishino, H.; Tajiri, H. Staging systems for hepatocellular carcinoma: Current status and future perspectives. World J. Hepatol. 2015, 7, 406–424. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | HCC (32 Patients) | CRC (36 Patients) | Controls (49 Patients) | p-Value |
|---|---|---|---|---|
| Male/Female | 27/5 | 24/12 | 24/25 | #* |
| Age (years) | 63.5 (33.0–85.0) | 67.0 (36.0–79.0)35 | 58.0 (21.0–88.0) | |
| BMI (kg/m2) | 27.2 (19.7–44.6) 31 | 26.6 (16.3–45.4) | 26.2 (20.3–39.7) | |
| Prothrombin Time (%) | 30.8 (26.7–307.0)30 | 28.8 (25.2–39.0)35 | n.d. | |
| Bilirubin (mg/dl) | 0.6 (0.2–2.5) 31 | 0.5 (0.1–1.0)35 | 0.5 (0.2–1.9) | * |
| ALT (U/l) | 49.5 (17.0–378) 30 | 28.0 (10.0–81.0) 34 | 20.0 (12.0–44.0) | **;#*** |
| AST (U/l) | 36.0 (14.0–502.0) 31 | 20.5 (11.0–165.0)34 | 28.0 (20.0–48.0) | *; #* |
| GGT (U/l) | 105 (25–807) 27 | 53 (19–590)33 | n.d. | ** |
| T2D | 15 | 6 | 9 | **; #** |
| HC | 3 | 8 | 8 | |
| HT | 18 | 16 | 18 | |
| HU | 4 | 3 | n.d. | |
| Tumor Grade: G1/G2/G3 | 5/20/429 | 1/23/125 | ||
| Primary Tumor T1/T2/T3/T4 | 13/9/9/1 | 7/20/3/030 | ||
| Vascular Invasion No/yes | 20/12 | 24/226 | ||
| TNM Stage IA/IB/IIA/IIB/III/IV | 14/8/7/2/1/0 | 1/4/13/9/1/1/231 |
| Correlation of Chemerin with: | HCC | CRC | All Tumor Patients | Controls |
|---|---|---|---|---|
| Prothrombin Time (%) | r = −0.103 p = 0.587 | r = −0.262 p = 0.128 | r = −0.172 p = 0.170 | n.d. |
| Bilirubin (mg/dL) | r = −0.316 p = 0.083 | r = −0.477 p = 0.004 | r = −0.386 p = 0.001 | r = −0.930 p = 0.540 |
| ALT (U/L) | r = −0.103 p = 0.590 | r = −0.186 p = 0.292 | r = −0.174 p = 0.169 | r = −0.182 p = 0.215 |
| AST (U/L) | r = 0.100 p = 0.593 | r = −0.267 p = 0.127 | r = −0.070 p = 0.577 | r = −0.196 p = 0.181 |
| GGT (U/L) | r = 0.145 p = 0.469 | r = −0.298 p = 0.092 | r = −0.087 p = 0.511 | n.d. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feder, S.; Kandulski, A.; Schacherer, D.; Weiss, T.S.; Buechler, C. Serum Chemerin Does Not Differentiate Colorectal Liver Metastases from Hepatocellular Carcinoma. Int. J. Mol. Sci. 2019, 20, 3919. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20163919
Feder S, Kandulski A, Schacherer D, Weiss TS, Buechler C. Serum Chemerin Does Not Differentiate Colorectal Liver Metastases from Hepatocellular Carcinoma. International Journal of Molecular Sciences. 2019; 20(16):3919. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20163919
Chicago/Turabian StyleFeder, Susanne, Arne Kandulski, Doris Schacherer, Thomas S. Weiss, and Christa Buechler. 2019. "Serum Chemerin Does Not Differentiate Colorectal Liver Metastases from Hepatocellular Carcinoma" International Journal of Molecular Sciences 20, no. 16: 3919. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20163919