Difference in Profiles of the Gut-Derived Tryptophan Metabolite Indole Acetic Acid between Transplanted and Non-Transplanted Patients with Chronic Kidney Disease

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Results
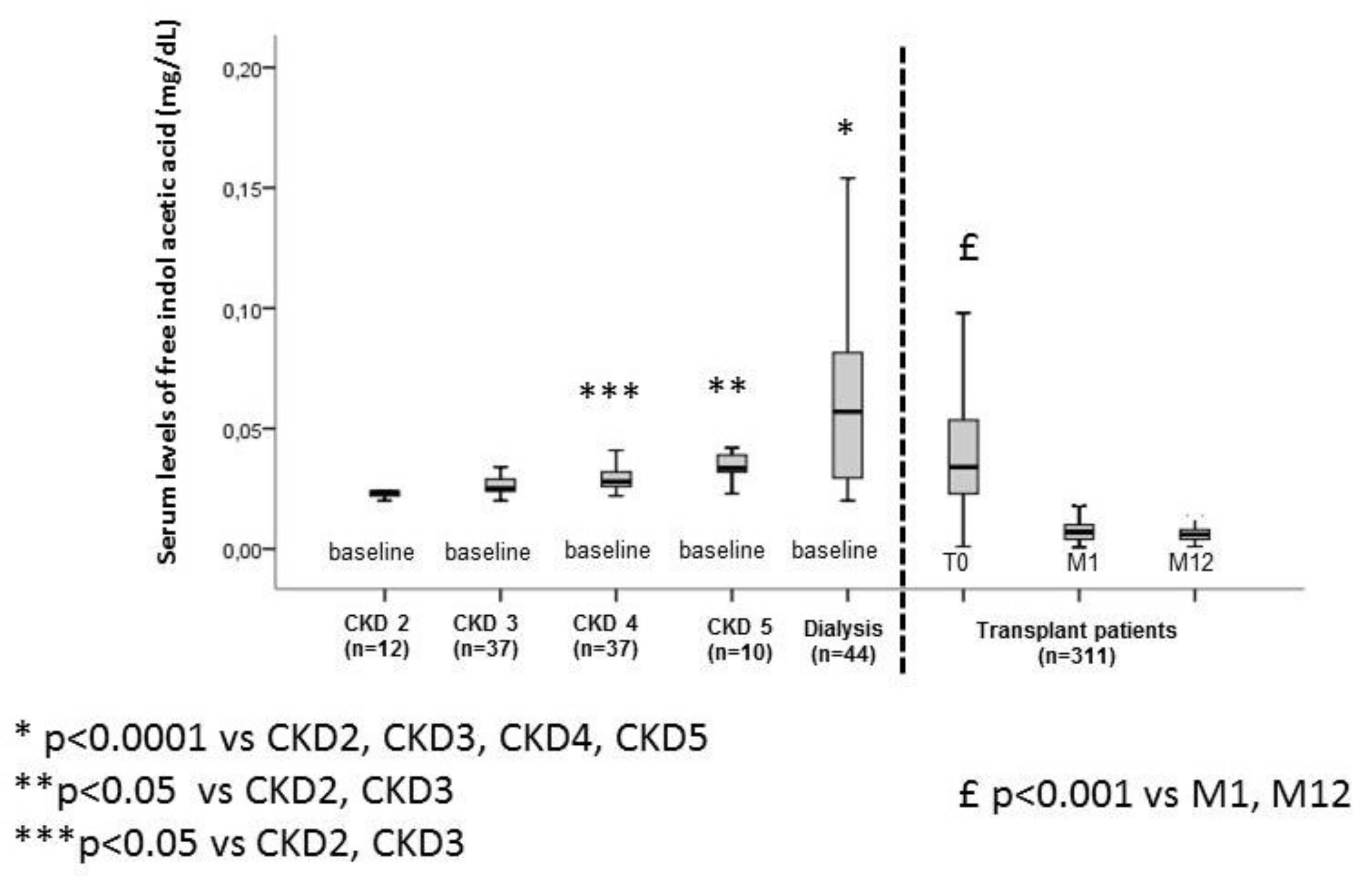
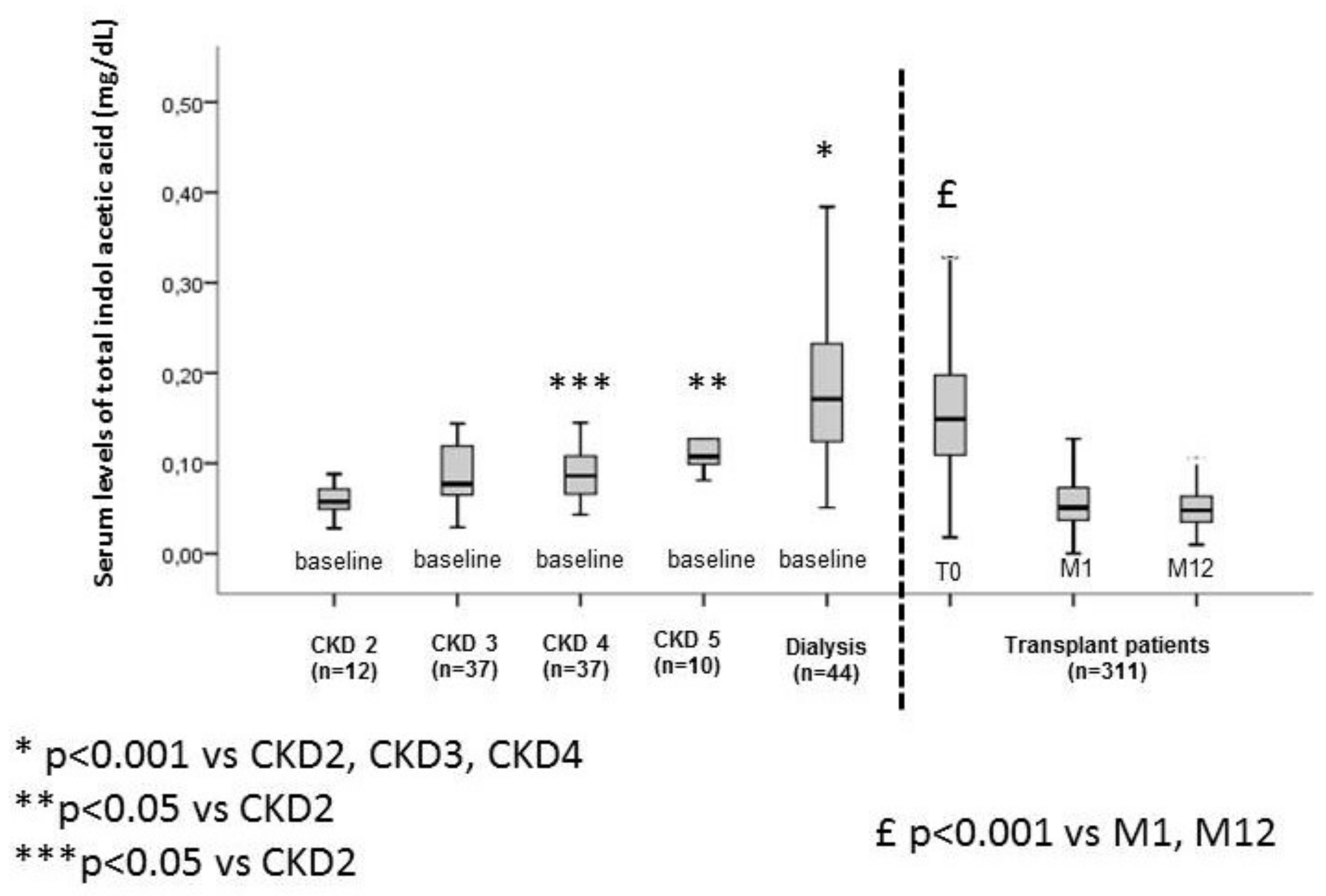
2.1. Levels of IAA

{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Non-Transplanted CKD Cohort (n = 140) | Transplanted Cohort (n = 311) |
|---|---|---|
| Age, years | 67 ± 12 | 56 ± 14 |
| Males, % | 60 | 61.8 |
| Diabetes mellitus, % | 42 | 9 |
| Hypertension, % | 90 | 69 |
| Dyslipidemia, % | 60 | 22 |
| History of cardiovascular disease, % | 31 | 23 |
| Active smoker, % | 41 | 17 |
| Body mass index (kg/m2) | 28 ± 6 | 25 ± 5 |
| Calcium, mmol/L | 2.3 ± 0.2 | 2.3 ± 0.2 |
| Phosphate, mmol/L | 1.3 ± 0.4 | 0.9 ± 0.5 |
| Proteins, g/L | 55.2 ± 6.9 | 69.0 ± 7.0 |
| Free IAA, mg/dL | 0.04 ± 0.03 | 0.19 ± 0.1 |
| Total IAA, mg/dL | 0.12 ± 0.08 | 2.4 ± 1.1 |



2.2. Non-Transplanted Patients with CKD
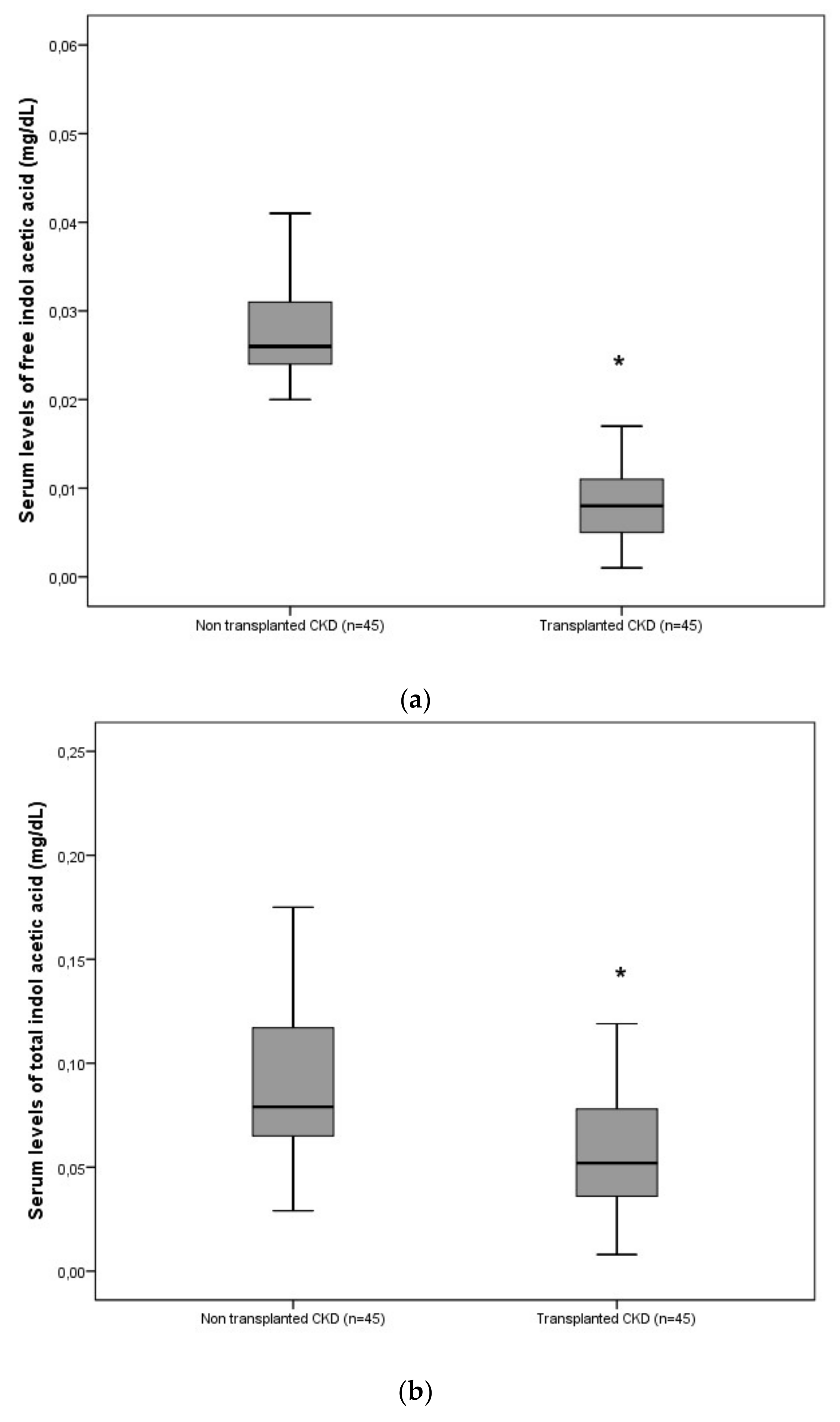
2.3. Transplanted Patients
3. Discussion
4. Methods
4.1. Study Population
4.2. The Transplanted Cohort
4.3. CKD Cohort
4.4. Laboratory Tests
4.5. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
References
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Vanholder, R.; De Smet, R.; Glorieux, G.; Argilés, A.; Baurmeister, U.; Brunet, P.; Clark, W.; Cohen, G.; De Deyn, P.P.; Deppisch, R.; et al. Review on uremic toxins: Classification, concentration, and interindividual variability. Kidney Int. 2003, 63, 1934–1943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schepers, E.; Glorieux, G.; Vanholder, R. The gut: The forgotten organ in uremia? Blood Purif. 2010, 29, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Barreto, F.C.; Barreto, D.V.; Liabeuf, S.; Meert, N.; Glorieux, G.; Temmar, M.; Choukroun, G.; Vanholder, R.; Massy, Z.A. European Uremic Toxin Work Group (EUTox) Serum indoxyl sulfate is associated with vascular disease and mortality in chronic kidney disease patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 1551–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dou, L.; Sallée, M.; Cerini, C.; Poitevin, S.; Gondouin, B.; Jourde-Chiche, N.; Fallague, K.; Brunet, P.; Calaf, R.; Dussol, B.; et al. The cardiovascular effect of the uremic solute indole-3 acetic acid. J. Am. Soc. Nephrol. 2015, 26, 876–887. [Google Scholar] [CrossRef] [PubMed]
- Vanholder, R.; Schepers, E.; Pletinck, A.; Nagler, E.V.; Glorieux, G. The Uremic Toxicity of Indoxyl Sulfate and p-Cresyl Sulfate: A Systematic Review. J. Am. Soc. Nephrol. 2014, 25, 1897–1907. [Google Scholar] [CrossRef] [PubMed]
- Opdebeeck, B.; Maudsley, S.; Azmi, A.; De Maré, A.; De Leger, W.; Meijers, B.; Verhulst, A.; Evenepoel, P.; D’Haese, P.C.; Neven, E. Indoxyl Sulfate and p-Cresyl Sulfate Promote Vascular Calcification and Associate with Glucose Intolerance. J. Am. Soc. Nephrol. 2019, 30, 751–766. [Google Scholar] [CrossRef] [PubMed]
- Dou, L.; Poitevin, S.; Sallée, M.; Addi, T.; Gondouin, B.; McKay, N.; Denison, M.S.; Jourde-Chiche, N.; Duval-Sabatier, A.; Cerini, C.; et al. Aryl hydrocarbon receptor is activated in patients and mice with chronic kidney disease. Kidney Int. 2018, 93, 986–999. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.-T.; Shu, K.-H.; Cheng, C.-H.; Wu, M.-J.; Yu, T.-M.; Chuang, Y.-W.; Chen, C.-H. Serum total p-cresol and indoxyl sulfate correlated with stage of chronic kidney disease in renal transplant recipients. Transpl. Proc. 2012, 44, 621–624. [Google Scholar] [CrossRef] [PubMed]
- Liabeuf, S.; Desjardins, L.; Massy, Z.A.; Brazier, F.; Westeel, P.F.; Mazouz, H.; Titeca-Beauport, D.; Diouf, M.; Glorieux, G.; Vanholder, R.; et al. Levels of Indoxyl Sulfate in Kidney Transplant Patients, and the Relationship With Hard Outcomes. Circ. J. 2016, 80, 722–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poesen, R.; Evenepoel, P.; De Loor, H.; Bammens, B.; Claes, K.; Sprangers, B.; Naesens, M.; Kuypers, D.; Augustijns, P.; Meijers, B. The influence of renal transplantation on retained microbial–human co-metabolites. Nephrol. Dial. Transpl. 2016, 31, 1721–1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liabeuf, S.; Barreto, D.V.; Barreto, F.C.; Meert, N.; Glorieux, G.; Schepers, E.; Temmar, M.; Choukroun, G.; Vanholder, R.; Massy, Z.A.; et al. Free p-cresylsulphate is a predictor of mortality in patients at different stages of chronic kidney disease. Nephrol. Dial. Transpl. 2010, 25, 1183–1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meijers, B.K.I.; Bammens, B.; De Moor, B.; Verbeke, K.; Vanrenterghem, Y.; Evenepoel, P. Free p-cresol is associated with cardiovascular disease in hemodialysis patients. Kidney Int. 2008, 73, 1174–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanholder, R.; Glorieux, G.; Massy, Z.A. Intestinal metabolites, chronic kidney disease and renal transplantation: Enigma Variations? Nephrol. Dial. Transpl. 2016, 31, 1547–1551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.; Xu, S.; Ren, Z.; Jiang, J.; Zheng, S. Gut microbiota and allogeneic transplantation. J. Transl. Med. 2015, 13, 275. [Google Scholar] [CrossRef] [PubMed]
- Dethlefsen, L.; Relman, D.A. Incomplete recovery and individualized responses of the human distal gut microbiota to repeated antibiotic perturbation. Proc. Natl. Acad. Sci. USA 2011, 108 (Suppl. 1), 4554–4561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallée, M.; Dou, L.; Cerini, C.; Poitevin, S.; Brunet, P.; Burtey, S. The aryl hydrocarbon receptor-activating effect of uremic toxins from tryptophan metabolism: A new concept to understand cardiovascular complications of chronic kidney disease. Toxins 2014, 6, 934–949. [Google Scholar] [CrossRef] [PubMed]
- Gondouin, B.; Cerini, C.; Dou, L.; Sallée, M.; Duval-Sabatier, A.; Pletinck, A.; Calaf, R.; Lacroix, R.; Jourde-Chiche, N.; Poitevin, S.; et al. Indolic uremic solutes increase tissue factor production in endothelial cells by the aryl hydrocarbon receptor pathway. Kidney Int. 2013, 84, 733–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Temmar, M.; Liabeuf, S.; Renard, C.; Czernichow, S.; Esper, N.E.; Shahapuni, I.; Presne, C.; Makdassi, R.; Andrejak, M.; Tribouilloy, C.; et al. Pulse wave velocity and vascular calcification at different stages of chronic kidney disease. J. Hypertens. 2010, 28, 163–169. [Google Scholar] [CrossRef] [PubMed]
- De Smet, R.; Dhondt, A.; Eloot, S.; Galli, F.; Waterloos, M.A.; Vanholder, R. Effect of the super-flux cellulose triacetate dialyser membrane on the removal of non-protein-bound and protein-bound uraemic solutes. Nephrol. Dial. Transpl. 2007, 22, 2006–2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| A | ||||
|---|---|---|---|---|
| Models | Free IAA | Total IAA | ||
| HR [95%CI] | p | HR [95%CI] | p | |
| Unadjusted | 3.1 [1.6–6.2] | 0.001 | 2.7 [1.4–5.2] | 0.003 |
| +age | 3.4 [1.7–6.8] | <0.0001 | 2.9 [1.5–5.5] | 0.001 |
| +age + CRP + hemoglobin | 2.3 [1.1–4.9] | 0.027 | 2.9 [1.5–5.5] | 0.002 |
| +age + CRP + albumin | 2.3 [1.1–4.9] | 0.027 | 2.5 [1.3–4.7] | 0.007 |
| +age+ CRP + dialysis | 2.5 [1.2–5.1] | 0.017 | 2.0 [0.9–4.1] | 0.070 |
| B | ||||
| Models | Free IAA | Total IAA | ||
| HR [95%CI] | p | HR [95%CI] | p | |
| Unadjusted | 2.3 [1.3–4.3] | 0.006 | 1.3 [0.7–2.3] | 0.378 |
| +age | 2.5 [1.4–4.7] | 0.002 | 1.3 [0.8–2.4] | 0.322 |
| +age + CRP + hemoglobin | 2.5 [1.3–4.6] | 0.031 | 1.3 [0.7–2.3] | 0.298 |
| +age + CRP + albumin | 2.1 [1.1–3.9] | 0.016 | 1.1 [0.6–2.1] | 0.612 |
| +age + CRP+ history of cardiovascular disease | 2.5 [1.3–4.6] | 0.004 | 1.3 [0.7–2.3] | 0.365 |
| +age + CRP +dialysis | 2.5 [1.3–4.8] | 0.004 | 1.1 [0.6–2.2] | 0.639 |
| A | ||||
|---|---|---|---|---|
| Models | Free IAA (T0) | Total IAA (T0) | ||
| HR [95%CI] | p | HR [95%CI] | p | |
| Unadjusted | 1.0 [0.6–1.8] | 0.980 | 0.8 [0.5–1.5] | 0.841 |
| +age | 0.8 [0.4–1.4] | 0.394 | 0.9 [0.5–1.6] | 0.698 |
| +age + history of cardiovascular disease | 1.2 [0.6–2.4] | 0.629 | 1.3 [0.6–2.5] | 0.511 |
| +age + history of cardiovascular disease + years on dialysis | 1.1 [0.6–2.3] | 0.700 | 1.2 [0.6–2.4] | 0.587 |
| B | ||||
| Models | Free IAA (T0) | Total IAA (T0) | ||
| HR [95%CI] | p | HR [95%CI] | p | |
| Unadjusted | 1.4 [0.8–2.5] | 0.185 | 1.4 [0.8–2.4] | 0.244 |
| +age | 1.2 [0.7–2.2] | 0.412 | 1.5 [0.8–2.5] | 0.167 |
| +age + history of cardiovascular disease | 1.2 [0.6–2.3] | 0.634 | 1.2 [0.6–2.3] | 0.610 |
| +age + history of cardiovascular disease + years on dialysis | 1.2 [0.6–2.4] | 0.517 | 1.3 [0.7–2.5] | 0.478 |
| C | ||||
| Models | Free IAA (T0) | Total IAA (T0) | ||
| HR [95%CI] | p | HR [95%CI] | p | |
| Unadjusted | 1.2 [0.7–2.0] | 0.569 | 0.9 [0.5–1.5] | 0.570 |
| +age | 1.3 [0.7–2.2] | 0.378 | 0.9 [0.5–1.5] | 0.609 |
| +age +years on dialysis | 1.3 [0.8–2.2] | 0.363 | 1.3 [0.5–1.5] | 0.621 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liabeuf, S.; Laville, S.M.; Glorieux, G.; Cheddani, L.; Brazier, F.; Titeca Beauport, D.; Vanholder, R.; Choukroun, G.; Massy, Z.A. Difference in Profiles of the Gut-Derived Tryptophan Metabolite Indole Acetic Acid between Transplanted and Non-Transplanted Patients with Chronic Kidney Disease. Int. J. Mol. Sci. 2020, 21, 2031. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21062031
Liabeuf S, Laville SM, Glorieux G, Cheddani L, Brazier F, Titeca Beauport D, Vanholder R, Choukroun G, Massy ZA. Difference in Profiles of the Gut-Derived Tryptophan Metabolite Indole Acetic Acid between Transplanted and Non-Transplanted Patients with Chronic Kidney Disease. International Journal of Molecular Sciences. 2020; 21(6):2031. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21062031
Chicago/Turabian StyleLiabeuf, Sophie, Solène M. Laville, Griet Glorieux, Lynda Cheddani, François Brazier, Dimitri Titeca Beauport, Raymond Vanholder, Gabriel Choukroun, and Ziad A. Massy. 2020. "Difference in Profiles of the Gut-Derived Tryptophan Metabolite Indole Acetic Acid between Transplanted and Non-Transplanted Patients with Chronic Kidney Disease" International Journal of Molecular Sciences 21, no. 6: 2031. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21062031