Combination Therapy with an SGLT2 Inhibitor as Initial Treatment for Type 2 Diabetes: A Systematic Review and Meta-Analysis


 ,
,
Abstract
:1. Introduction
2. Methodology
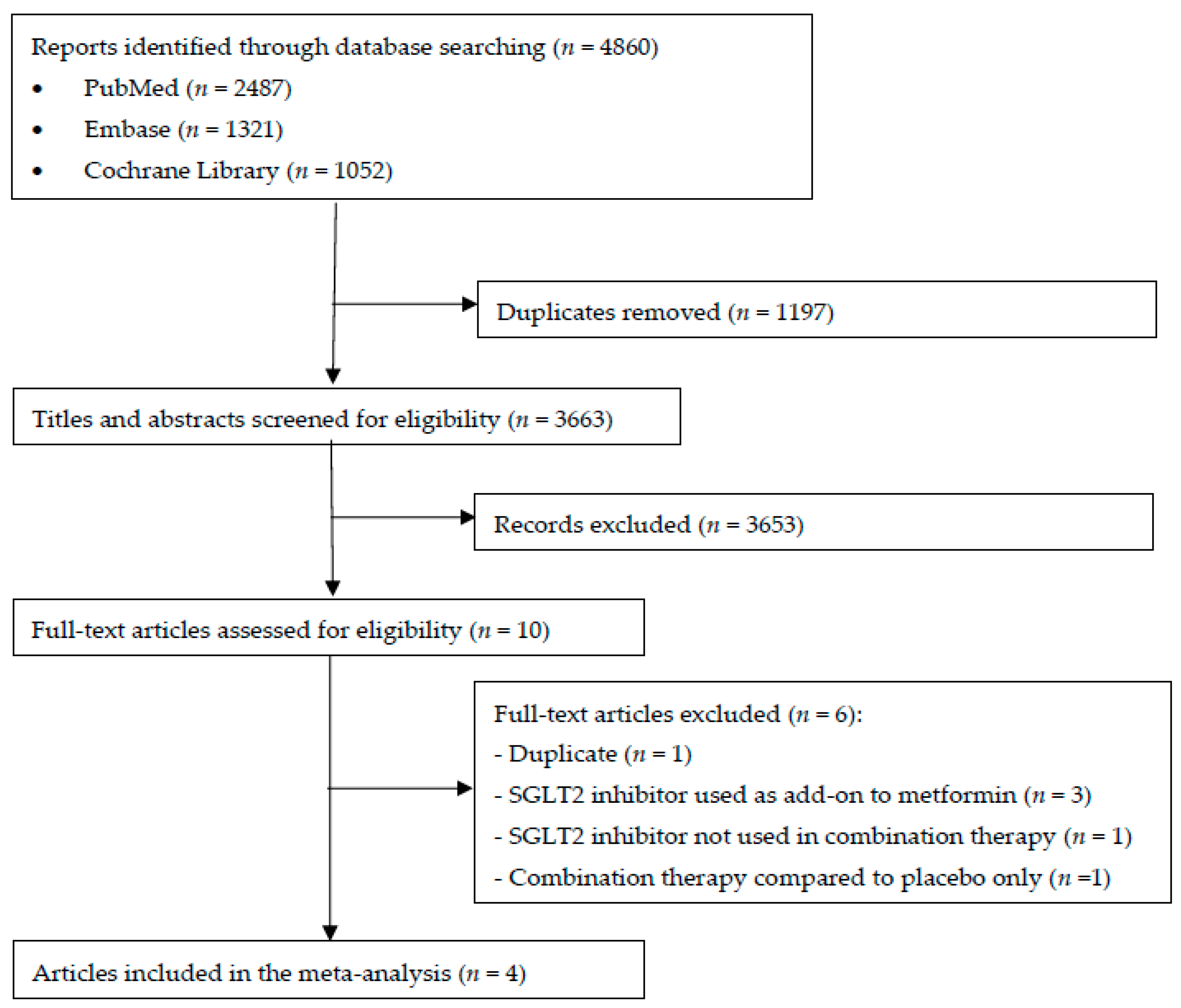
2.1. Study Selection
2.2. Electronic Searches
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Measures of Treatment Effect
2.6. Assessment of Heterogeneity and Reporting Bias
2.7. Data Synthesis
2.8. Overall Quality of Evidence Rating
2.9. Sub Group and Sensitivity Analysis
3. Results
3.1. Risk of Bias Assessments
3.2. Combination SGLT2 Inhibitor and Metformin Therapy versus Metformin Monotherapy
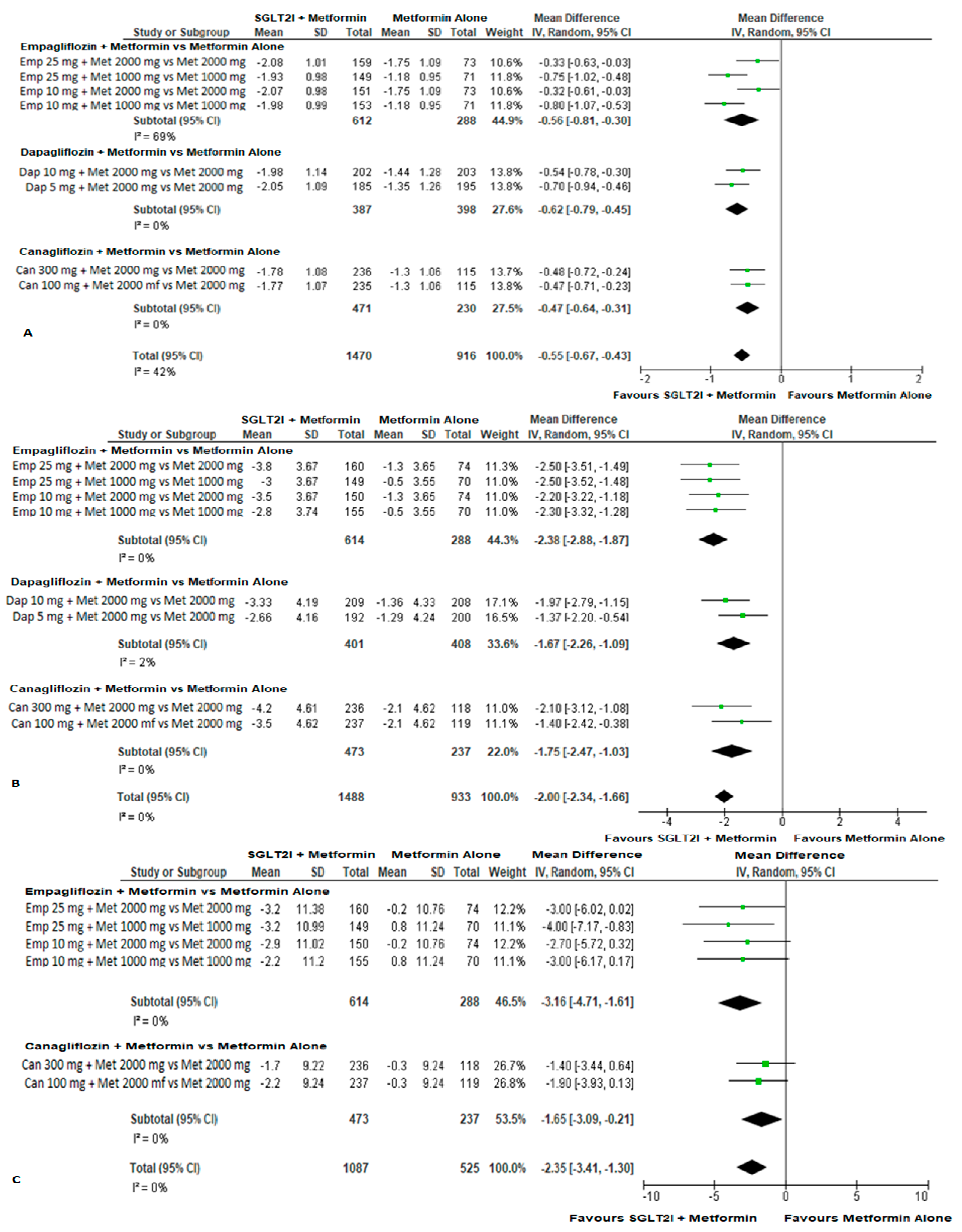
3.2.1. Efficacy
3.2.2. Safety
3.3. Combination SGLT2 Inhibitor and Metformin versus SGLT2 Inhibitor Monotherapy
3.3.1. Efficacy
3.3.2. Safety
3.4. High Dose SGLT2 Inhibitor and Metformin Combination Therapy versus Low Dose SGLT2 Inhibitor and Metformin Combination Therapy
3.4.1. Efficacy
3.4.2. Safety
3.5. Combination SGLT2 Inhibitor and DPP-4 Inhibitor versus Monotherapies
3.5.1. Efficacy
3.5.2. Safety
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Davies, M.J.; D’Alessio, D.A.; Fradkin, J.; Kernan, W.N.; Mathieu, C.; Mingrone, G.; Rossing, P.; Tsapas, A.; Wexler, D.J.; Buse, J.B. Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2018, 41, 2669–2701. [Google Scholar] [CrossRef] [PubMed]
- Garber, A.J.; Abrahamson, M.J.; Barzilay, J.I.; Blonde, L.; Bloomgarden, Z.T.; Bush, M.A.; Dagogo-Jack, S.; DeFronzo, R.A.; Einhorn, D.; Fonseca, V.A.; et al. Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Comprehensive Type 2 Diabetes Management Algorithm—2018 Executive Summary. Endocr. Pract. 2018, 24, 91–120. [Google Scholar] [CrossRef] [PubMed]
- Cersosimo, E.; Johnson, E.L.; Chovanes, C.; Skolnik, N. Initiating therapy in patients newly diagnosed with type 2 diabetes: Combination therapy vs a stepwise approach. Diabetes Obes. Metab. 2018, 20, 497–507. [Google Scholar] [CrossRef]
- Cahn, A.; Cefalu, W.T. Clinical considerations for use of initial combination therapy in type 2 diabetes. Diabetes Care 2016, 39, S137–S145. [Google Scholar] [CrossRef] [PubMed]
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998, 352, 837–853. [Google Scholar] [CrossRef]
- Holman, R.R.; Paul, S.K.; Bethel, M.A.; Matthews, D.R.; Neil, H.A. 10-year follow-up of intensive glucose control in type 2 diabetes. N. Engl. J. Med. 2008, 359, 1577–1589. [Google Scholar] [CrossRef] [PubMed]
- Ferrannini, E. Sodium-glucose co-transporters and their inhibition: Clinical physiology. Cell Metab. 2017, 26, 27–38. [Google Scholar] [CrossRef]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R.; et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N. Engl. J. Med. 2018. [Google Scholar] [CrossRef]
- Zelniker, T.A.; Wiviott, S.D.; Raz, I.; Im, K.; Goodrich, E.L.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Furtado, R.H.M.; et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: A systematic review and meta-analysis of cardiovascular outcome trials. Lancet 2018, 393, 31–39. [Google Scholar] [CrossRef]
- Phung, O.J.; Sobieraj, D.M.; Engel, S.S.; Rajpathak, S.N. Early combination therapy for the treatment of type 2 diabetes mellitus: Systematic review and meta-analysis. Diabetes Obes. Metab. 2014, 16, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.; Gao, X.; Yang, W.; Han, X.; Ji, L. Efficacy and safety of initial combination therapy in treatment-naive type 2 diabetes patients: A systematic review and meta-analysis. Diabetes Ther. 2018, 9, 1995–2014. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE guidelines: 7. Rating the quality of evidence--inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- Hadjadj, S.; Rosenstock, J.; Meinicke, T.; Woerle, H.J.; Broedl, U.C. Initial combination of empagliflozin and metformin in patients with type 2 diabetes. Diabetes Care 2016, 39, 1718–1728. [Google Scholar] [CrossRef]
- Henry, R.R.; Murray, A.V.; Marmolejo, M.H.; Hennicken, D.; Ptaszynska, A.; List, J.F. Dapagliflozin, metformin XR, or both: Initial pharmacotherapy for type 2 diabetes, a randomised controlled trial. Int. J. Clin. Pract. 2012, 66, 446–456. [Google Scholar] [CrossRef]
- Rosenstock, J.; Chuck, L.; Gonzalez-Ortiz, M.; Merton, K.; Craig, J.; Capuano, G.; Qiu, R. Initial combination therapy with canagliflozin plus metformin versus each component as monotherapy for drug-naive type 2 diabetes. Diabetes Care 2016, 39, 353–362. [Google Scholar] [CrossRef]
- Lewin, A.; DeFronzo, R.A.; Patel, S.; Liu, D.; Kaste, R.; Woerle, H.J.; Broedl, U.C. Initial combination of empagliflozin and linagliptin in subjects with type 2 diabetes. Diabetes Care 2015, 38, 394–402. [Google Scholar] [CrossRef]
- Janssen Research & Development, LLC. A study to Evaluate the Effectiveness, Safety, and Tolerability of Canagliflozin In Combination with Metformin in the Treatment of Patients with Type 2 Diabetes Mellitus with Inadequate Glycemic Control with Diet and Exercise. Available online: https://clinicaltrials.gov/ct2/show/results/NCT01809327 (accessed on 8 May 2018).
- Ferrannini, G.; Hach, T.; Crowe, S.; Sanghvi, A.; Hall, K.D.; Ferrannini, E. Energy balance after sodium-glucose cotransporter 2 inhibition. Diabetes Care 2015, 38, 1730–1735. [Google Scholar] [CrossRef] [PubMed]
- Rena, G.; Hardie, D.G.; Pearson, E.R. The mechanisms of action of metformin. Diabetologia 2017, 60, 1577–1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Baar, M.J.B.; van Ruiten, C.C.; Muskiet, M.H.A.; van Bloemendaal, L.; IJzerman, R.G.; van Raalte, D.H. SGLT2 Inhibitors in combination therapy: From mechanisms to clinical considerations in type 2 diabetes management. Diabetes Care 2018, 41, 1543–1556. [Google Scholar] [CrossRef] [PubMed]
- Wulffele, M.G.; Kooy, A.; de Zeeuw, D.; Stehouwer, C.D.; Gansevoort, R.T. The effect of metformin on blood pressure, plasma cholesterol and triglycerides in type 2 diabetes mellitus: A systematic review. J. Intern. Med. 2004, 256, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Domecq, J.P.; Prutsky, G.; Leppin, A.; Sonbol, M.B.; Altayar, O.; Undavalli, C.; Wang, Z.; Elraiyah, T.; Brito, J.P.; Mauck, K.F.; et al. Drugs commonly associated with weight change: A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2015, 100, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Mazidi, M.; Rezaie, P.; Gao, H.K.; Kengne, A.P. Effect of sodium-glucose cotransport-2 inhibitors on blood pressure in people with type 2 diabetes mellitus: A systematic review and meta-analysis of 43 randomized control trials with 22 528 patients. J. Am. Heart. Assoc. 2017, 6. [Google Scholar] [CrossRef]
- Bouchoucha, M.; Uzzan, B.; Cohen, R. Metformin and digestive disorders. Diabetes Metab. 2011, 37, 90–96. [Google Scholar] [CrossRef]
- Roden, M.; Weng, J.; Eilbracht, J.; Delafont, B.; Kim, G.; Woerle, H.J.; Broedl, U.C.; EMPA-REG MONO Trial Investigators. Empagliflozin monotherapy with sitagliptin as an active comparator in patients with type 2 diabetes: A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Diabetes Endocrinol. 2013, 1, 208–219. [Google Scholar] [CrossRef]
- Ferrannini, E.; Ramos, S.J.; Salsali, A.; Tang, W.; List, J.F. Dapagliflozin monotherapy in type 2 diabetic patients with inadequate glycemic control by diet and exercise: A randomized, double-blind, placebo-controlled, phase 3 trial. Diabetes Care 2010, 33, 2217–2224. [Google Scholar] [CrossRef]
- Stenlof, K.; Cefalu, W.T.; Kim, K.A.; Alba, M.; Usiskin, K.; Tong, C.; Canovatchel, W.; Meininger, G. Efficacy and safety of canagliflozin monotherapy in subjects with type 2 diabetes mellitus inadequately controlled with diet and exercise. Diabetes Obes. Metab. 2013, 15, 372–382. [Google Scholar] [CrossRef] [Green Version]
- Wanner, C.; Lachin, J.M.; Inzucchi, S.E.; Fitchett, D.; Mattheus, M.; George, J.; Woerle, H.J.; Broedl, U.C.; von Eynatten, M.; Zinman, B.; et al. Empagliflozin and clinical outcomes in patients with type 2 diabetes mellitus, established cardiovascular disease, and chronic kidney disease. Circulation 2018, 137, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Shi, W.; Wang, T.; Tang, H. SGLT2 inhibitor plus DPP-4 inhibitor as combination therapy for type 2 diabetes: A systematic review and meta-analysis. Diabetes Obes. Metab. 2018, 20, 1972–1976. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.K.; Kang, Y.M.; Lee, S.E.; Lee, J.; Park, J.Y.; Lee, W.J.; Kim, Y.J.; Jung, C.H. Efficacy and safety of combination therapy with SGLT2 and DPP4 inhibitors in the treatment of type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab. 2018, 44, 393–401. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association (ADA). 9. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2018. Diabetes Care 2018, 41, S86–S104. [Google Scholar] [CrossRef] [PubMed]
- Fu, A.Z.; Sheehan, J.J. Treatment intensification for patients with type 2 diabetes and poor glycaemic control. Diabetes Obes. Metab. 2016, 18, 892–898. [Google Scholar] [CrossRef] [PubMed]
- Desai, U.; Kirson, N.Y.; Kim, J.; Khunti, K.; King, S.; Trieschman, E.; Hellstern, M.; Hunt, P.R.; Mukherjee, J. Time to treatment intensification after monotherapy failure and its association with subsequent glycemic control among 93,515 patients with type 2 diabetes. Diabetes Care 2018, 41, 2096–2104. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Perez, L.E.; Alvarez, M.; Dilla, T.; Gil-Guillen, V.; Orozco-Beltran, D. Adherence to therapies in patients with type 2 diabetes. Diabetes Ther. 2013, 4, 175–194. [Google Scholar] [CrossRef] [PubMed]
- Harris, S.B. The power of two: An update on fixed-dose combinations for type 2 diabetes. Expert Rev. Clin. Pharmacol. 2016, 9, 1453–1462. [Google Scholar] [CrossRef] [Green Version]
- Scheen, A.J. Pharmacokinetic characteristics and clinical efficacy of an SGLT2 inhibitor plus DPP-4 inhibitor combination therapy in type 2 diabetes. Clin. Pharmacokinet. 2017, 56, 703–718. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Name, Year, Reference | Study Size, n | Mean Age (years) | Sex (%male) | Mean HbA1c (%) | Mean Body Weight (kg) | Combination Therapy Total Daily Doses | SGLT2 Inhibitor Monotherapy Daily Dose | Monotherapy with Other Anti-Hyperglycaemic Agent Total Daily Dose | Study Duration (weeks) |
|---|---|---|---|---|---|---|---|---|---|
| Combination SGLT2 inhibitor and metformin | |||||||||
| Hadjadj et al., 2016 [17] | 1327 | 53 | 56 | 8.7 | 83 | Empagliflozin 25 mg + metformin 2000 mg Empagliflozin 25 mg + metformin 1000 mg Empagliflozin 10 mg + metformin 2000 mg Empagliflozin 10 mg + metformin 1000 mg | Empagliflozin 25 mg Empagliflozin 10 mg | Metformin 2000 mg Metformin 1000 mg | 24 |
| Henry et al., 2012 [18] | 638 | 52 | 48 | 9.1 | 88 | Dapagliflozin 10 mg + metformin 2000 mg | Dapagliflozin 10 mg | Metformin 2000 mg | 24 |
| Henry et al., 2012 [18] | 598 | 52 | 44 | 9.1 | 85 | Dapagliflozin 5 mg + metformin 2000 mg | Dapagliflozin 5 mg | Metformin 2000 mg | 24 |
| Rosenstock et al., 2016 [19] | 1186 | 55 | 48 | 8.8 | 91 | Canagliflozin 300 mg + metformin 2000 mg Canagliflozin 100 mg + metformin 2000 mg | Canagliflozin 300 mg Canagliflozin 100 mg | Metformin 2000 mg | 26 |
| Combination SGLT2 inhibitor and DPP-4 inhibitor | |||||||||
| Lewin et al., 2015 [20] | 667 | 55 | 54 | 8.0 | 88 | Empagliflozin 25mg + linagliptin 5mg Empagliflozin 10mg + linagliptin 5mg | Empagliflozin 25 mg Empagliflozin 10 mg | Linagliptin 5 mg | 52 |
| Study Name, Year | Random Sequence Generation | Allocation Concealment | Selective Reporting | Other Bias | Blinding of Participants & Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Cochrane Risk of Bias Score |
|---|---|---|---|---|---|---|---|---|
| Hadjadj et al., 2016 [17] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | High risk * | High risk |
| Henry et al., 2012 [18] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Henry et al., 2012 [18] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Rosenstock et al., 2016 [19] | Low risk | Unclear risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Lewin et al., 2015 [20] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | High risk * | High risk |
| Safety Outcome | Comparator 1 | Comparator 2 | I2 | RR (95% CI) |
|---|---|---|---|---|
| Number of Events/Total Subjects | Number of Events/Total Subjects | |||
| i. SGLT2 inhibitor + metformin vs. metformin monotherapy | ||||
| SGLT2 inhibitor + metformin | Metformin monotherapy | |||
| ≥1 AE(s) | 886/1559 | 535/987 | 0% | 1.05 (0.98, 1.13) |
| ≥1 drug-related AE(s) | 219/1559 | 119/987 | 0% | 1.22 (0.98, 1.50) |
| ≥1 serious AE(s) | 33/1559 | 24/987 | 0% | 0.85 (0.49, 1.46) |
| Hypoglycaemia * | 42/1559 | 19/987 | 0% | 1.20 (0.70, 2.06) |
| UTI | 82/1559 | 43/987 | 0% | 1.12 (0.77, 1.61) |
| Events suggestive of genital infection | 63/1559 | 18/987 | 0% | 2.22 (1.33, 3.72) |
| Diarrhoea | 82/1559 | 67/987 | 56% | 0.86 (0.50, 1.48) |
| ii. SGLT2 inhibitor + metformin vs. SGLT2 inhibitor monotherapy | ||||
| SGLT2 inhibitor + metformin | SGLT2 inhibitor monotherapy | |||
| ≥1 AE(s) | 886/1559 | 629/1236 | 43% | 1.08 (0.99, 1.17) |
| ≥1 drug-related AE(s) | 219/1559 | 164/1236 | 55% | 1.06 (0.79, 1.43) |
| ≥1 serious AE(s) | 33/1559 | 29/1236 | 0% | 0.94 (0.56, 1.57) |
| Hypoglycaemia * | 42/1559 | 20/1236 | 0% | 1.67 (0.99, 2.83) |
| UTI | 82/1559 | 59/1236 | 0% | 0.97 (0.69, 1.37) |
| Events suggestive of genital infection | 63/1559 | 76/1236 | 0% | 0.69 (0.50, 0.96) |
| Diarrhoea | 82/1559 | 29/1236 | 0% | 2.23 (1.46, 3.40) |
| iii. High dose SGLT2 inhibitor + metformin vs. low dose SGLT2 inhibitor + metformin | ||||
| High dose SGLT2 inhibitor + metformin | Low dose SGLT2 inhibitor + metformin | |||
| ≥1 AE(s) | 445/788 | 441/771 | 29% | 0.98 (0.89, 1.08) |
| ≥1 drug-related AE(s) | 127/788 | 92/771 | 64% | 1.38 (0.90, 2.12) |
| ≥1 serious AE(s) | 15/788 | 18/771 | 17% | 0.79 (0.36, 1.76) |
| Hypoglycaemia * | 26/788 | 16/771 | 0% | 1.48 (0.80, 2.75) |
| UTI | 48/788 | 34/771 | 34% | 1.37 (0.79, 2.39) |
| Events suggestive of genital infection | 38/788 | 25/771 | 0% | 1.43 (0.87, 2.35) |
| Diarrhoea | 43/788 | 39/771 | 15% | 1.06 (0.66, 1.69) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milder, T.Y.; Stocker, S.L.; Abdel Shaheed, C.; McGrath-Cadell, L.; Samocha-Bonet, D.; Greenfield, J.R.; Day, R.O. Combination Therapy with an SGLT2 Inhibitor as Initial Treatment for Type 2 Diabetes: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 45. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8010045
Milder TY, Stocker SL, Abdel Shaheed C, McGrath-Cadell L, Samocha-Bonet D, Greenfield JR, Day RO. Combination Therapy with an SGLT2 Inhibitor as Initial Treatment for Type 2 Diabetes: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2019; 8(1):45. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8010045
Chicago/Turabian StyleMilder, Tamara Y., Sophie L. Stocker, Christina Abdel Shaheed, Lucy McGrath-Cadell, Dorit Samocha-Bonet, Jerry R. Greenfield, and Richard O. Day. 2019. "Combination Therapy with an SGLT2 Inhibitor as Initial Treatment for Type 2 Diabetes: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 8, no. 1: 45. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8010045