Application of the Sepsis-3 Consensus Criteria in a Geriatric Acute Care Unit: A Prospective Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Population
2.2. Study Procedures
- The Cumulative Index Rating Scale (CIRS) Comorbidity Score (CIRS-CS) and Severity Index (CIRS-SI), a validated index of multimorbidity and clinical complexity designed for geriatric patients [31], which has been shown to be associated with the risk of acute bacterial infections [32,33]. CIRS-CS was calculated as the sum of the scores (from 0 to 4, where 0 = no disease and 4 = likely lethal disease) assigned to each of the 14 items corresponding to the body’s organs/systems. CIRS-SI was calculated as the number of items with a score ranking 3 or 4;
- The Rockwood Clinical Frailty Scale (RCFS) referred to the patient’s performance before admission. This is a validated score evaluating the presence of frailty or disability in geriatric patients, according to the deficit accumulation model, ranging from 1 (very good physical performance in healthy active aging) to 9 (bedridden patient with short term life expectancy) [34].
2.3. Statistical Analyses
2.4. Ethical Statement
3. Results
3.1. General Characteristics of the Population
3.2. qSOFA vs. SIRS for In-Hospital Mortality Prediction
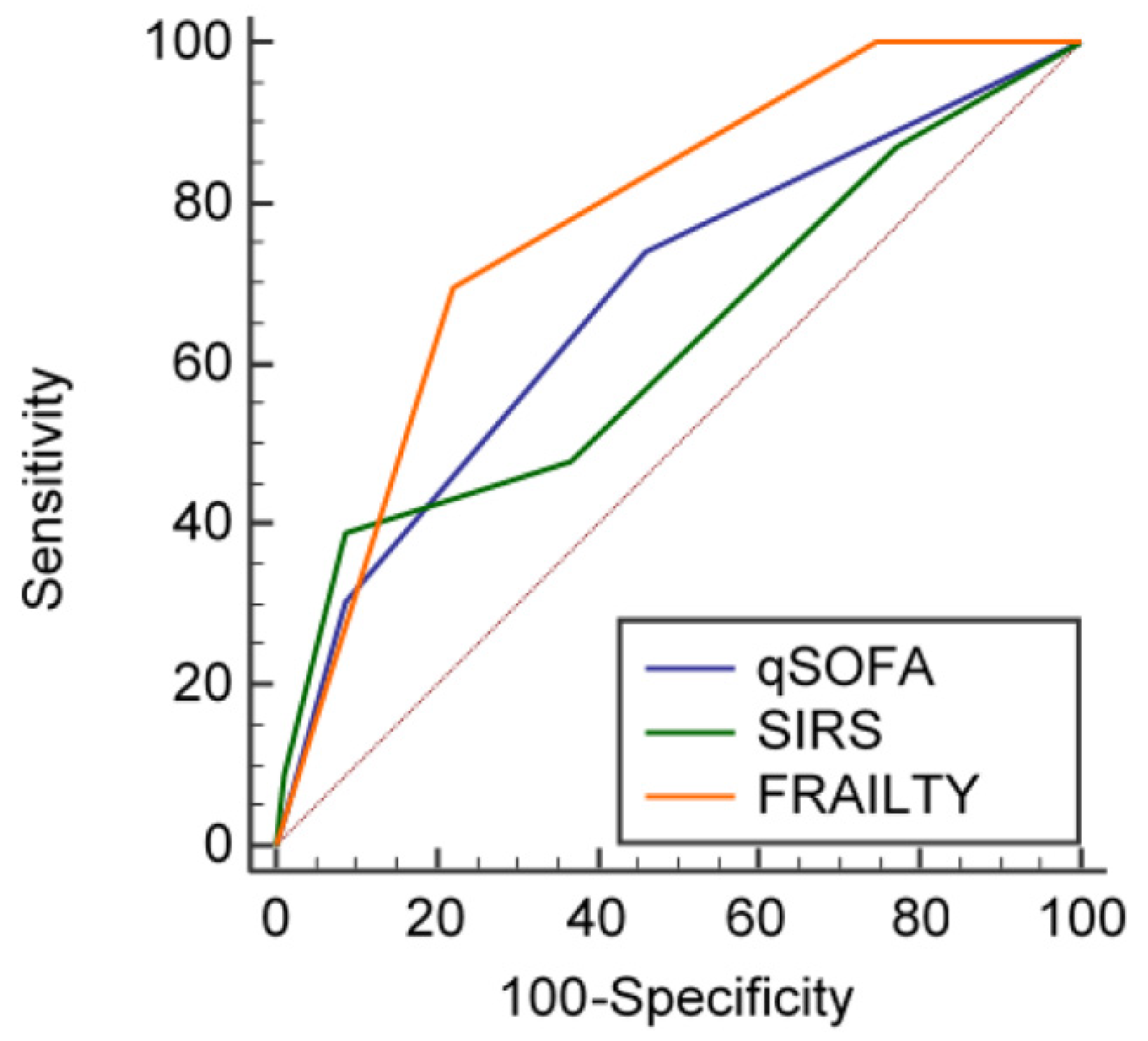
3.3. qSOFA vs. SIRS for Three-Month Mortality Prediction
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.R.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kempker, J.A.; Martin, G.S. The Changing Epidemiology and Definitions of Sepsis. Clin. Chest Med. 2016, 37, 165–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esper, A.M.; Moss, M.; Lewis, C.A.; Nisbet, R.; Mannino, D.M.; Martin, G.S. The role of infection and comorbidity: Factors that influence disparities in sepsis. Crit. Care Med. 2006, 34, 2576–2582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankar-Hari, M.; Bertolini, G.; Brunkhorst, F.M.; Bellomo, R.; Annane, D.; Deutschman, C.S.; Singer, M. Judging quality of current septic shock definitions and criteria. Crit. Care 2015, 19, 445. [Google Scholar] [CrossRef] [PubMed]
- Klein Klouwenberg, P.M.C.; Ong, D.S.Y.; Bonten, M.J.M.; Cremer, O.L. Classification of sepsis, severe sepsis and septic shock: The impact of minor variations in data capture and definition of SIRS criteria. Intensive Care Med. 2012, 38, 811–819. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, P.; Edelson, D.P.; Churpek, M.M. Identifying Patients with Sepsis on the Hospital Wards. Chest 2017, 151, 898–907. [Google Scholar] [CrossRef] [PubMed]
- Raith, E.P.; Udy, A.A.; Bailey, M.; McGloughlin, S.; MacIsaac, C.; Bellomo, R.; Pilcher, D.V.; Australian and New Zealand Intensive Care Society (ANZICS) Centre for Outcomes and Resource Evaluation (CORE). Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality Among Adults with Suspected Infection Admitted to the Intensive Care Unit. JAMA 2017, 317, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [PubMed]
- Rudd, K.E.; Seymour, C.W.; Aluisio, A.R.; Augustin, M.E.; Bagenda, D.S.; Beane, A.; Byiringiro, J.C.; Chang, C.C.H.; Colas, L.N.; Day, N.P.J.; et al. Association of quick sequential (sepsis-related) organ failure assessment (qSOFA) score with excess hospital mortality in adults with suspected infection in low- and middle-income countries. JAMA 2018, 319, 2202–2211. [Google Scholar] [CrossRef] [PubMed]
- Finkelsztein, E.J.; Jones, D.S.; Ma, K.C.; Pabon, M.A.; Delgado, T.; Nakahira, K.; Arbo, J.E.; Berlin, D.A.; Schenck, E.J.; Choi, A.M.; et al. Comparison of qSOFA and SIRS for predicting adverse outcomes of patients with suspicion of sepsis outside the intensive care unit. Crit. Care. 2017, 21, 73. [Google Scholar] [CrossRef] [PubMed]
- Churpek, M.M.; Snyder, A.; Han, X.; Sokol, S.; Pettit, N.; Howell, M.D.; Edelson, D.P. Quick sepsis-related organ failure assessment, systemic inflammatory response syndrome, and early warning scores for detecting clinical deterioration in infected patients outside the Intensive Care Unit. Am. J. Respir. Crit. Care Med. 2017, 195, 906–911. [Google Scholar] [CrossRef] [PubMed]
- Freund, Y.; Lemachatti, N.; Krastinova, E.; van Laer, M.; Claessens, Y.E.; Avondo, A.; Occelli, C.; Fieral-Pierssens, A.L.; Truchot, J.; Ortega, M.; et al. Prognostic Accuracy of Sepsis-3 Criteria for In-Hospital Mortality Among Patients with Suspected Infection Presenting to the Emergency Department. JAMA 2017, 317, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, R.M.; Greenwood, J.C.; Nuckton, T.J.; Darger, B.; Shofer, F.S.; Troeger, D.; Jung, S.Y.; Speich, K.G.; Valencia, J.; Kilgannon, J.H.; et al. Comparison of qSOFA with current emergency department tools for screening of patients with sepsis for critical illness. Emerg. Med. J. 2018, 35, 350–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- April, M.D.; Aguirre, J.; Tannenbaum, L.I.; Moore, T.; Pingree, A.; Thaxton, R.E.; Sessions, D.J.; Lantry, J.H. Sepsis Clinical Criteria in Emergency Department Patients Admitted to an Intensive Care Unit: An External Validation Study of Quick Sequential Organ Failure Assessment. J. Emerg. Med. 2016, 52, 622–631. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.M.; Greenslade, J.H.; McKenzie, J.V.; Chu, K.; Brown, A.F.; Lipman, J. SIRS, qSOFA and organ dysfunction: Insights from a prospective database of emergency department patients with infection. Chest 2017, 151, 586–596. [Google Scholar] [CrossRef] [PubMed]
- Askim, A.; Moser, F.; Gustad, L.T.; Stene, H.; Gundersen, M.; Asvold, B.O.; Dale, J.; Bjornsen, L.P.; Damas, J.K.; Solligard, E. Poor performance of quick-SOFA (qSOFA) score in predicting severe sepsis and mortality—A prospective study of patients admitted with infection to the emergency department. Scand. J. Trauma Resusc. Emerg. Med. 2017, 25, 56. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.P.; Safford, M.M.; Shapiro, N.I.; Baddley, J.W.; Wang, H.E. Application of the Third International Consensus Definitions for Sepsis (Sepsis-3) Classification: A retrospective population-based cohort study. Lancet Infect. Dis. 2017, 17, 661–670. [Google Scholar] [CrossRef]
- Umemura, Y.; Ogura, H.; Gando, S.; Kushimoto, S.; Saitoh, D.; Mayumi, T.; Fujishima, S.; Abe, T.; Ikeda, H.; Kotani, J.; et al. Assessment of mortality by qSOFA in patients with sepsis outside ICU: A post hoc subgroup analysis by the Japanese Association for Acute Medicine Sepsis Registry Study Group. J. Infect. Chemother. 2017, 23, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Fernando, S.M.; Tran, A.; Taljaard, M.; Cheng, W.; Rochwerg, B.; Seely, A.J.E.; Perry, J.J. Prognostic accuracy of the quick sequential organ failure assessment for mortality in patients with suspected infection. Ann. Intern. Med. 2018, 168, 266–275. [Google Scholar] [CrossRef]
- Reunes, S.; Rombaut, V.; Vogelaers, D.; Brusselaers, N.; Lizy, C.; Cankurtaran, M.; Labeau, S.; Petrovic, M.; Blot, S. Risk factors and mortality for nosocomial bloodstream infections in elderly patients. Eur. J. Intern. Med. 2011, 22, e39–e44. [Google Scholar] [CrossRef] [PubMed]
- Gavazzi, G.; Escobar, P.; Olive, F.; Couturier, P.; Franco, A. Nosocomial bacteremia in very old patients: Predictors of mortality. Aging Clin. Exp. Res. 2005, 17, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Choi, H.S.; Ko, Y.G.; Yun, D.H. Performance of the Geriatric Nutritional Risk Index in predicting 28-day hospital mortality in older adult patients with sepsis. Clin. Nutr. 2013, 32, 843–848. [Google Scholar] [CrossRef]
- Tsuruta, R.; Oda, Y. A clinical perspective of sepsis-associated delirium. J. Intensive Care 2016, 4, 18. [Google Scholar] [CrossRef] [PubMed]
- Brummel, M.E.; Bell, S.P.; Girard, T.D.; Pandharipande, P.P.; Jackson, J.C.; Morandi, A.; Thompson, J.L.; Chandrasekhar, R.; Bernard, G.R.; Dittus, R.S.; et al. Frailty and subsequent disability and mortality among patients with critical illness. Am. J. Respir. Crit. Care Med. 2017, 196, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Beck, M.K.; Jensen, A.B.; Nielsen, A.B.; Perner, A.; Moseley, P.L.; Brunak, S. Diagnostic trajectories of prior multi-morbidity predict sepsis mortality. Sci. Rep. 2016, 6, 36624. [Google Scholar] [CrossRef] [PubMed]
- Meschi, T.; Ticinesi, A.; Prati, B.; Montali, A.; Ventura, A.; Nouvenne, A.; Borghi, L. A novel organizational model to face the challenge of multimorbid elderly patients in an internal medicine setting: A case study from Parma Hospital, Italy. Intern. Emerg. Med. 2016, 11, 667–676. [Google Scholar] [CrossRef]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Thai, V.; Lau, F.; Wolch, G.; Yang, J.; Quan, H.; Fassbender, K. Impact of infections on the survival of hospitalized advanced cancer patients. J. Pain Symptom Manag. 2012, 43, 549–557. [Google Scholar] [CrossRef]
- Mazzone, A.; Dentali, F.; La Regina, M.; Foglia, E.; Gambacorta, M.; Garagiola, E.; Bonardi, G.; Clerici, P.; Concia, E.; Colombo, F.; et al. Clinical Features, Short-Term Mortality, and Prognostic Risk Factors of Septic Patients Admitted to Internal Medicine Units: Results of an Italian Multicenter Prospective Study. Medicine 2016, 95, e2124. [Google Scholar] [CrossRef] [PubMed]
- Salvi, F.; Miller, M.D.; Grilli, A.; Giorgi, R.; Towers, A.L.; Morichi, V.; Spazzafumo, L.; Mancinelli, L.; Espinosa, E.; Rappelli, A.; et al. A manual of guidelines to score the modified cumulative illness rating scale and its validation in acute hospitalized elderly patients. J. Am. Geriatr. Soc. 2008, 56, 1926–1931. [Google Scholar] [CrossRef] [PubMed]
- Ticinesi, A.; Nouvenne, A.; Folesani, G.; Prati, B.; Morelli, I.; Guida, L.; Lauretani, F.; Maggio, M.; Meschi, T. An investigation of multimorbidity measures as risk factors for pneumonia in elderly frail patients admitted to hospital. Eur. J. Intern. Med. 2016, 28, 102–106. [Google Scholar] [CrossRef]
- Ticinesi, A.; Nouvenne, A.; Folesani, G.; Prati, B.; Morelli, I.; Guida, L.; Turroni, F.; Ventura, M.; Lauretani, F.; Maggio, M.; et al. Multimorbidity in elderly hospitalised patients and risk of Clostridium difficile infection: A retrospective study with the Cumulative Illness Rating Scale (CIRS). BMJ Open 2015, 5, e009316. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [PubMed]
- Estella, A.; Gamazo-Del Rio, J.; Alvarez-Manzanares, J.; Julian-Jimenez, A.; Gonzalez del Castillo, J. Prognostic accuracy of qsofa according to the site of infection in older patient attendend in Emergency Department. Eur. J. Intern. Med. 2018, 50, e13–e15. [Google Scholar] [CrossRef]
- Gonzalez del Castillo, J.; Julian-Jimenez, A.; Gonzalez-Martinez, F.; Alvarez-Manzanares, J.; Pinera, P.; Navarro-Bustos, C.; Martinez-Ortiz de Zarate, M.; Llopis-Roca, F.; Deban Fernandez, M.; Gamazo-Del Rio, J.; et al. Prognostic accuracy of SIRS criteria, qSOFA score and GYM score for 30-day mortality in older non-severely dependent infected patients attended in the emergency department. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 2361–2369. [Google Scholar] [CrossRef]
- Camm, C.F.; Hayward, G.; Elias, T.C.N.; Bowen, J.S.T.; Hassanzadeh, R.; Fanshawe, T.; Pendlebury, S.T.; Lasserson, D.S. Sepsis recognition tools in acute ambulatory care: Associations with process of care and clinical outcomes in a service evaluation of an Emergency Multidisciplinary Unit in Oxfordshire. BMJ Open 2018, 8, e020497. [Google Scholar] [CrossRef]
- Zucchelli, A.; Vetrano, D.L.; Marengoni, A.; Grande, G.; Romanelli, G.; Calderón-Larrañaga, A.; Fratiglioni, L.; Rizzuto, D. Frailty predicts short-term survival even in older adults without multimorbidity. Eur. J. Intern. Med. 2018, 56, 53–56. [Google Scholar]
- Vetrano, D.L.; Palmer, K.; Marengoni, A.; Marzetti, E.; Lattanzio, F.; Roller-Wirnsberger, R.; Lopez Samaniego, L.; Rordriguez-Mañas, L.; Bernabei, R.; Onder, G.; Joint Action ADVANTAGE WP4 Group. Frailty and multimorbidity: A systematic review and meta-analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2018, in press. [Google Scholar]
- Onder, G.; Vetrano, D.L.; Marengoni, A.; Bell, J.S.; Johnell, K.; Palmer, K.; Optimising Pharmacotherapy through Pharmacoepidemiology Network (OPPEN). Accounting for frailty when treating chronic diseases. Eur. J. Intern. Med. 2018, 56, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Ticinesi, A.; Lauretani, F.; Nouvenne, A.; Porro, E.; Fanelli, G.; Maggio, M.; Meschi, T. C-reactive protein (CRP) measurement in geriatric patients hospitalized for acute infection. Eur. J. Intern. Med. 2017, 37, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Soysal, P.; Stubbs, B.; Lucato, P.; Luchini, C.; Solmi, M.; Peluso, R.; Sergi, G.; Isik, A.T.; Manzato, E.; Maggi, S.; et al. Inflammation and frailty in the elderly: A systematic review and meta-analysis. Ageing Res. Rev. 2016, 31, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szakmany, T.; Pugh, R.; Kopczynska, M.; Lundin, R.M.; Sharif, B.; Morgan, P.; Ellis, G.; Abreu, J.; Kulikouskaya, S.; Bashir, K.; et al. Defining sepsis on the wards: Results of a multi-centre point-prevalence study comparing two sepsis definitions. Anaesthesia 2018, 73, 195–204. [Google Scholar] [CrossRef]
- Kopczynska, M.; Sharif, B.; Cleaver, S.; Spencer, N.; Kurani, A.; Lee, C.; Davis, J.; Durie, C.; Jospeh-Gubral, J.; Sharma, A.; et al. Sepsis-related deaths in the at-risk population of the wards: Attributable fraction of mortality in a large point-prevalence study. BMC Res. Notes 2018, 11, 720. [Google Scholar] [CrossRef]
- Shankar-Hari, M.; Harrison, D.A.; Rowan, K.M.; Rubenfeld, G.D. Estimating attributable fraction of mortality from sepsis to inform clinical trials. J. Crit. Care 2018, 45, 33–39. [Google Scholar] [CrossRef]
- Kopczynska, M.; Sharif, B.; Cleaver, S.; Spencer, N.; Kurani, A.; Lee, C.; Davis, J.; Durie, C.; Joseph-Gubral, J.; Sharma, A.; et al. Red-flag sepsis and SOFA identifies different patient population at risk of sepsis-related deaths on the general ward. Medicine 2018, 97, e13238. [Google Scholar] [CrossRef] [PubMed]
- Abou Dagher, G.; El Khuri, C.; Chehadeh, A.A.; Chami, A.; Bachir, R.; Zebian, D.; Bou Chebl, R. Are patients with cancer with sepsis and bacteraemia at a higher risk of mortality? A retrospective chart review of patients presenting to a tertiary care center in Lebanon. BMJ Open 2017, 7, e013502. [Google Scholar] [CrossRef]
- Ranzani, O.T.; Prina, E.; Menendez, R.; Ceccato, A.; Cilloniz, C.; Mendez, R.; Gabarrus, A.; Barbeta, E.; Bassi, G.L.; Ferrer, M.; et al. New sepsis definition (Sepsis-3) and community-acquired pneumonia mortality. A validation and clinical decision-making study. Am. J. Respir. Crit. Care Med. 2017, 196, 1287–1297. [Google Scholar] [CrossRef]
- Muller, M.; Guignard, V.; Schefold, J.C.; Leichtle, A.B.; Exadaktylos, A.K.; Pfortmueller, C.A. Utility of quick sepsis-related organ failure assessment (qSOFA) to predict outcome in patients with pneumonia. PLoS ONE 2017, 12, e0188913. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameters | Overall Population (n = 272) | Survivors at Discharge (n = 241) | Dead during Hospital Stay (n = 31) | p * |
|---|---|---|---|---|
| Females, n (%) | 144 (52.9) | 126 (52.3) | 18 (58.1) | 0.54 |
| Age, years | 83.7 ± 7.4 | 83.3 ± 7.3 | 86.3 ± 7.1 | 0.04 |
| Institutionalized, n (%) | 44 (16.2) | 31 (12.8) | 13 (41.9) | <0.001 |
| Frailty (RCFS score 4–5), n (%) | 109 (40.1) | 102 (42.3) | 7 (22.5) | <0.001 |
| Disability (RCFS score >5), n (%) | 123 (45.2) | 99 (41.1) | 24 (77.4) | |
| RCFS, score | 5 [4–6] | 5 [4–6] | 7 [6–8] | <0.001 |
| Cancer, n (%) | 35 (12.9) | 30 (12.5) | 5 (16.1) | 0.56 |
| Dementia, n (%) | 94 (34.6) | 76 (31.5) | 18 (58.1) | 0.004 |
| CIRS-CS, score | 14 [10–17] | 13 [10–17] | 14 [13–16] | 0.88 |
| CIRS-SI, score | 2 [2–3] | 2 [2–3] | 3 [2–3] | <0.001 |
| Drugs taken before admission, n | 6.2 ± 3.1 | 6.1 ± 3.1 | 7.3 ± 3.0 | 0.06 |
| Pulmonary infection, n (%) | 156 (57.6) | 141 (58.5) | 15 (48.3) | 0.40 |
| Gastrointestinal infection, n (%) | 32 (11.8) | 32 (13.3) | 1 (3.2) | |
| Urinary tract infection, n (%) | 70 (25.8) | 55 (22.8) | 15 (48.4) | |
| Other primary infection, n (%) | 13 (4.8) | 13 (5.4) | 0 (0) | |
| qSOFA, score | 1 [0–1] | 0 [0–1] | 1 [0–2] | <0.001 |
| SIRS, score | 1 [1–2] | 1 [1–2] | 2 [1–3] | 0.003 |
| C-reactive protein, mg/L | 109 [61–182] | 104 [57–170] | 194 [96–250] | <0.001 |
| Body temperature, °C | 37.1 ± 0.7 | 37.1 ± 0.7 | 37.1 ± 0.5 | 0.70 |
| Heart rate, bpm | 85.9 ± 17.8 | 84.6 ± 17.2 | 96.8 ± 18.9 | 0.08 |
| Systolic blood pressure, mmHg | 127.4 ± 21.9 | 127.8 ± 21.2 | 123.5 ± 26.8 | 0.31 |
| Diastolic blood pressure, mmHg | 72.5 ± 10.6 | 72.8 ± 10.2 | 70.9 ± 13.7 | 0.38 |
| Peripheral oxygen saturation, % | 95.0 ± 2.9 | 95.2 ± 2.7 | 94.3 ± 3.8 | 0.11 |
| Respiratory rate, bpm | 19.3 ± 5.1 | 19.2 ± 4.9 | 20.3 ± 6.9 | 0.28 |
| GCS, score | 14.6 ± 1.5 | 14.7 ± 1.3 | 13.8 ± 2.7 | 0.001 |
| PaCO2, mmHg | 38.3 ± 11.2 | 37.3 ± 8.8 | 45.1 ± 20.4 | 0.004 |
| WBC count, n/mm ×1000 | 9.8 [6.5–13.9] | 9.6 [6.6–13.9] | 11.6 [6.4–15.4] | 0.59 |
| Procalcitonin, ng/mL | 0.7 [0.1–3.0] | 0.5 [0.1–2.7] | 2 [0.9–9.6] | 0.72 |
| Parameters | OR (95% CI) | p * |
|---|---|---|
| Model 1—Univariable | ||
| qSOFA score | 2.114 (1.308–3.419) | <0.001 |
| Model 2—Bivariable | ||
| qSOFA score | 1.454 (0.801–2.637) | 0.21 |
| Frailty | 5.242 (2.101–13.083) | <0.001 |
| Model 3—Multivariable | ||
| qSOFA score | 0.828 (0.245–2.796) | 0.76 |
| Frailty | 2.534 (0.523–12.270) | 0.24 |
| Age | 1.005 (0.905–1.116) | 0.93 |
| Sex (female vs. male) | 0.594 (0.138–2.552) | 0.44 |
| Institutionalization | 1.928 (0.324–11.461) | 0.47 |
| Dementia | 0.347 (0.050–2.401) | 0.28 |
| CIRS-SI | 0.991 (0.480–2.048) | 0.98 |
| CRP | 1.010 (1.001–1.020) | 0.045 |
| PaCO2 | 1.041 (0.986–1.100) | 0.14 |
| Parameters | OR (95% CI) | p * |
|---|---|---|
| Model 1—Univariable | ||
| SIRS score | 1.703 (1.180–2.457) | <0.001 |
| Model 2—Bivariable | ||
| SIRS score | 1.438 (0.932–2.219) | 0.10 |
| Frailty | 5.710 (2.372–13.744) | <0.001 |
| Model 3—Multivariable | ||
| SIRS score | 1.084 (0.542–2.168) | 0.82 |
| Frailty | 2.629 (0.533–12.968) | 0.23 |
| Age | 1.004 (0.903–1.115) | 0.95 |
| Sex (female vs. male) | 0.583 (0.136–2.502) | 0.47 |
| Institutionalization | 1.766 (0.330–9.436) | 0.51 |
| Dementia | 0.379 (0.058–2.473) | 0.32 |
| CIRS-SI | 0.984 (0.477–2.030) | 0.97 |
| CRP | 1.009 (1.001–1.019) | 0.041 |
| PaCO2 | 1.042 (0.987–1.099) | 0.14 |
| Parameters | OR (95% CI) | p * |
|---|---|---|
| Model 1—Univariable | ||
| qSOFA score | 2.255 (1.510–3.368) | <0.001 |
| Model 2—Bivariable | ||
| qSOFA score | 1.915 (1.151–3.188) | 0.012 |
| Frailty | 3.958 (2.131–7.352) | <0.001 |
| Model 3—Multivariable | ||
| qSOFA score | 2.249 (1.009–5.013) | 0.04 |
| Frailty | 2.336 (1.002–5.729) | 0.04 |
| Age | 0.992 (0.915–1.077) | 0.85 |
| Sex (female vs. male) | 0.369 (0.128–1.066) | 0.07 |
| Institutionalization | 0.550 (0.135–2.236) | 0.40 |
| Dementia | 1.474 (0.393–5.528) | 0.56 |
| CIRS-SI | 1.669 (0.979–2.847) | 0.06 |
| CRP | 0.998 (0.991–1.005) | 0.56 |
| PaCO2 | 1.032 (0.987–1.078) | 0.16 |
| Parameters | OR (95% CI) | p * |
|---|---|---|
| Model 1—Univariable | ||
| SIRS score | 1.369 (1.032–1.816) | 0.03 |
| Model 2—Bivariable | ||
| SIRS score | 1.260 (0.876–1.812) | 0.21 |
| Frailty | 4.855 (2.632–8.954) | <0.001 |
| Model 3—Multivariable | ||
| SIRS score | 1.149 (0.696–1.897) | 0.57 |
| Frailty | 2.505 (1.038–6.044) | 0.04 |
| Age | 0.995 (0.920–1.077) | 0.91 |
| Sex (female vs. male) | 0.414 (0.149–1.148) | 0.09 |
| Institutionalization | 0.693 (0.180–2.665) | 0.59 |
| Dementia | 1.105 (0.319–3.829) | 0.88 |
| CIRS-SI | 1.543 (0.930–2.562) | 0.09 |
| CRP | 0.999 (0.992–1.005) | 0.68 |
| PaCO2 | 1.011 (0.969–1.033) | 0.22 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bastoni, D.; Ticinesi, A.; Lauretani, F.; Calamai, S.; Catalano, M.L.; Catania, P.; Cecchia, M.; Cerundolo, N.; Galluzzo, C.; Giovini, M.; et al. Application of the Sepsis-3 Consensus Criteria in a Geriatric Acute Care Unit: A Prospective Study. J. Clin. Med. 2019, 8, 359. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8030359
Bastoni D, Ticinesi A, Lauretani F, Calamai S, Catalano ML, Catania P, Cecchia M, Cerundolo N, Galluzzo C, Giovini M, et al. Application of the Sepsis-3 Consensus Criteria in a Geriatric Acute Care Unit: A Prospective Study. Journal of Clinical Medicine. 2019; 8(3):359. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8030359
Chicago/Turabian StyleBastoni, Davide, Andrea Ticinesi, Fulvio Lauretani, Simone Calamai, Maria Letizia Catalano, Pamela Catania, Martina Cecchia, Nicoletta Cerundolo, Claudia Galluzzo, Manuela Giovini, and et al. 2019. "Application of the Sepsis-3 Consensus Criteria in a Geriatric Acute Care Unit: A Prospective Study" Journal of Clinical Medicine 8, no. 3: 359. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8030359