1. Introduction
Management of patients with bilateral cleft lip and palate (BCLP) requires collaboration from infancy to maturity between the multidisciplinary cleft team, patient, and parents [
1,
2,
3]. Nasal deformity is typically associated with congenital cleft lip and palate [
1,
2,
3]. The reconstruction of a bilateral cleft lip and nasal deformity is especially challenging owing to complex intrinsic characteristics including a short columella, a flattened nasal tip, and splayed nostril bases [
1,
2,
3]. While various surgical strategies are available for repair of bilateral cleft lip and nasal deformity merit recognition for the achievement of outstanding results, the synchronous correction of the nasal deformity (primary rhinoplasty) at the time of lip repair has been recognized as a major advance in the management of patients with BCLP [
4,
5,
6,
7,
8,
9,
10,
11,
12,
13,
14,
15,
16].
Interestingly, proponents of primary rhinoplasty have argued that this approach is essential for reaching an optimal outcome in bilateral cleft lip reconstruction [
7,
8,
9,
10,
11,
12,
13,
14,
15,
16]. On the other hand, opponents have based their opinions mainly on the traditional teaching that “primary rhinoplasty may potentially interfere with nasal growth” [
17,
18,
19,
20]. Studies showing the absence of nasal growth interference had methodological limitations (e.g., mixed sample sizes, age groups, and/or methods used for nasal measurements) that hindered universal acceptance of primary rhinoplasty within cleft centers worldwide [
21,
22,
23,
24,
25,
26,
27]. It is therefore essential that further outcome analyses are conducted by implementing a well-delineated methodology based on accurate quantitative evaluation of nasal dimensions and comparisons between treated patients and normal subjects. Three-dimensional (3D) photogrammetric technology allows for fast image capture with good-resolution color representation and provides an accurate, reliable, and reproducible system for quantifying complex nose structure [
28,
29,
30,
31,
32,
33]. However, we are not aware of any 3D photogrammetric investigation assessing long-term nasal growth after primary rhinoplasty in patients with BCLP. In addition to enabling linear and angular measurements along the topographic contour of the nose [
28,
29,
30,
31,
32,
33], 3D photogrammetry offers the ability to evaluate the nasal surface area and perform volumetric analyses. This allows us to assess nasal growth-related data, with no need to expose the patient to ionizing radiation [
33,
34,
35,
36,
37,
38].
From this perspective, Dr. Noordhoff’s approach to primary rhinoplasty and subsequent modifications have been adopted at the Chang Gung Craniofacial Center over the past three decades [
7,
39]. This center has assessed different outcomes of primary rhinoplasty with or without an intermediate rhinoplasty procedure [
40,
41,
42], but has not performed nasal growth evaluation in those patients who reached skeletal maturity. A senior surgeon (L.-J.L.) treated a subgroup of patients with BCLP using Noordhoff’s principles for bilateral cleft rhinoplasty between the late 1990s and early 2000s. As these patients recently reached skeletal maturity, the potential influence of rhinoplasty procedures on nasal growth can now be fully measured.
The purposes of this 3D photogrammetric study were to assess long-term nasal growth in patients with BCLP who underwent primary rhinoplasty, and to compare the 3D-based data to those in normal controls.
2. Patients and Methods
This was an observational retrospective study involving consecutive non-syndromic patients with complete BCLP who underwent primary rhinoplasty, with or without intermediate rhinoplasty, by a single surgeon (L.-J.L.) at the Chang Gung Craniofacial Center between 1995 and 2002. All included patients had reached skeletal maturity (defined as completing the growth spurt and showing no further increase in height) [
43,
44] at the time of data collection. Subjects with no history of facial trauma, facial surgery, or craniofacial deformity were enrolled as normal controls and matched for age, sex, and ethnicity. For comparisons between patients with BCLP and normal subjects, all patients who underwent rhinoplasty were combined as a single group, regardless of the approach used.
Demographic, clinical, and 3D nasal photogrammetric-based outcome data were collected. Patients were excluded if they were older than 4 months at the time of undergoing primary rhinoplasty, older than 6 years at the time of undergoing intermediate rhinoplasty, had associated syndromes, had a history of nasal surgery between the primary/intermediate rhinoplasty and data collection, did not undergo adequate 3D imaging, or did not complete the follow-up observation (<17 years). Patients who underwent orthognathic surgery were also excluded. The study was approved by the Institutional Review Board (20180309B0) and complied with the 1975 Declaration of Helsinki, as amended in 1983.
2.1. Primary Cleft Rhinoplasty
All primary cleft lip and nose surgical repairs were performed at 3–4 months of age using Noordhoff’s method with muscle-repositioning, banked-fork flap, and primary rhinoplasty [
7,
39]. Presurgical nasoalveolar molding (NAM) and a postsurgical nasal conformer were routinely used [
41]. For primary rhinoplasty, a supraperichondrial dissection of the lower lateral cartilages was performed through the columella and alar bases using blunt tenotomy scissors. For further mobilization of the lower lateral cartilages, the attachments of the alar base at the pyriform rim were bilaterally released by extending the incision from the pyriform aperture upward, between the upper lateral cartilage and lower lateral cartilages, to the dorsal cartilage. Two types of sutures (between the dorsal and lower lateral cartilages and between the upper lateral cartilages and lower lateral cartilages) were placed in each alar dome to advance the lower lateral cartilages superiorly, resulting in widening of the intercartilaginous incision region. The buccal mucosal flap (designated the L flap) was then advanced into the midpoint of the intercartilaginous incision and sutured in place for reconstruction of the intentionally created intercartilaginous defect.
2.2. Intermediate Cleft Rhinoplasty
Intermediate rhinoplasty was performed at preschool age to address select clinical issues and patient/parental complaints, depending upon the magnitude of the nasal deformity (short columella, wide nose, and/or flat tip). Elongation of the columella, repositioning of the lower lateral cartilages, and improvement of tip projection were achieved. We implemented combined maneuvers, including the open tip approach with a columella incision extending intranasally or a nasal tip incision for V to Y advancement; advancement of the nasal floor tissue onto the columella; conchal or costal cartilage grafting into the medial crura; and cinch, intercrural, and transdomal sutures [
40]. Each specific procedure was selected according to the surgeon’s preference and the patient’s diagnosis.
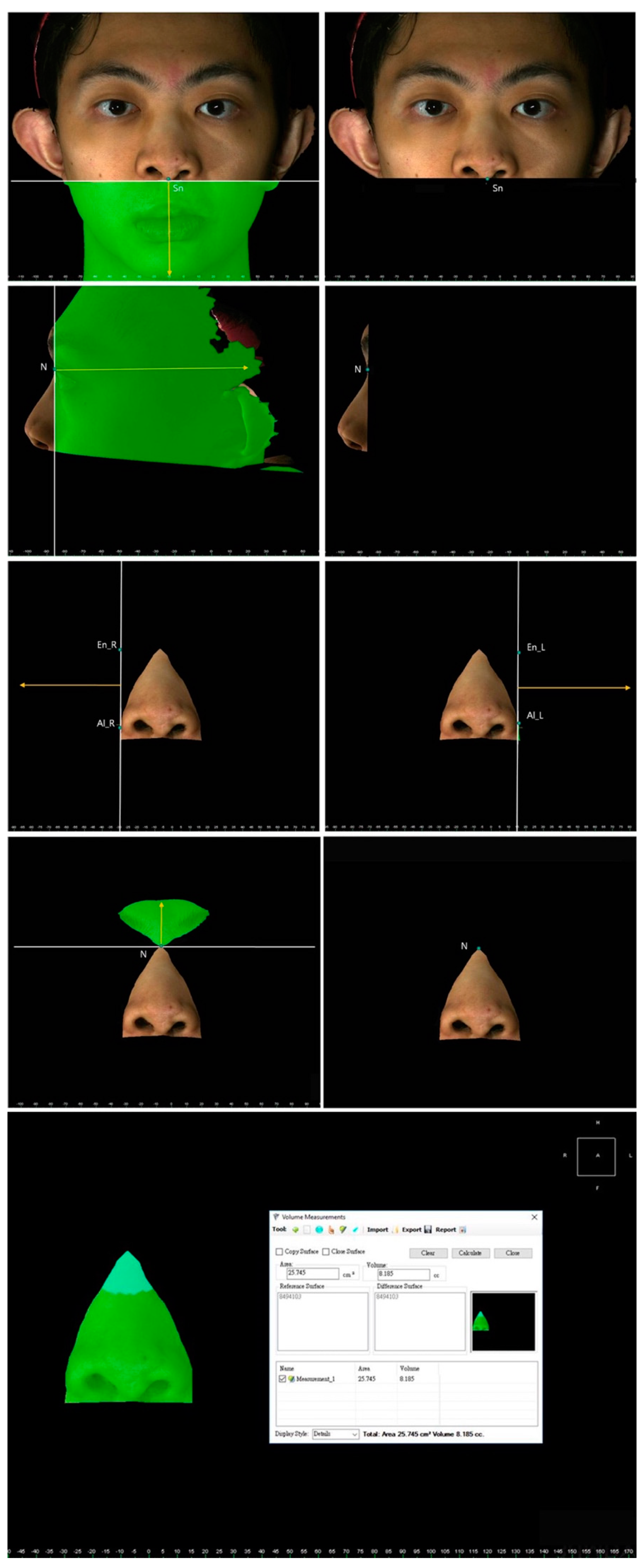
2.3. D Photogrammetric Analysis
Imaging data were acquired using the 3dMD system (3dMD LLC, Atlanta, GA, USA) under standard conditions including natural head position, relaxed facial musculature, and habitual dental occlusion. The system was calibrated before every capture process. Data sets were analyzed using 3dMD Vultus software (version 2.2, 3dMD Inc., Atlanta, GA, USA), with previously verified accuracy and reliability [
45,
46].
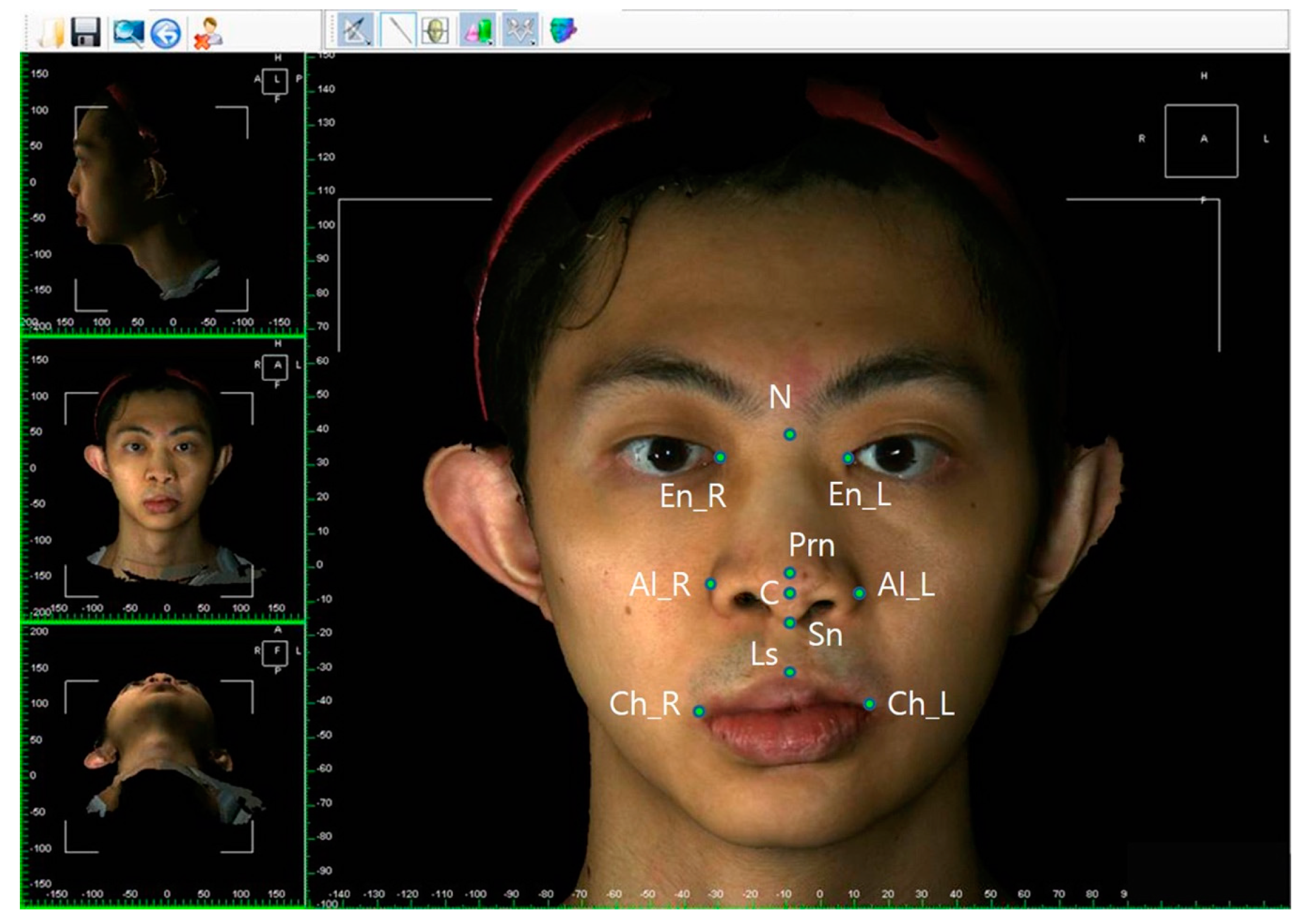
The facial and nasal anatomical landmarks (
Figure 1) were defined according to original Farkas descriptions [
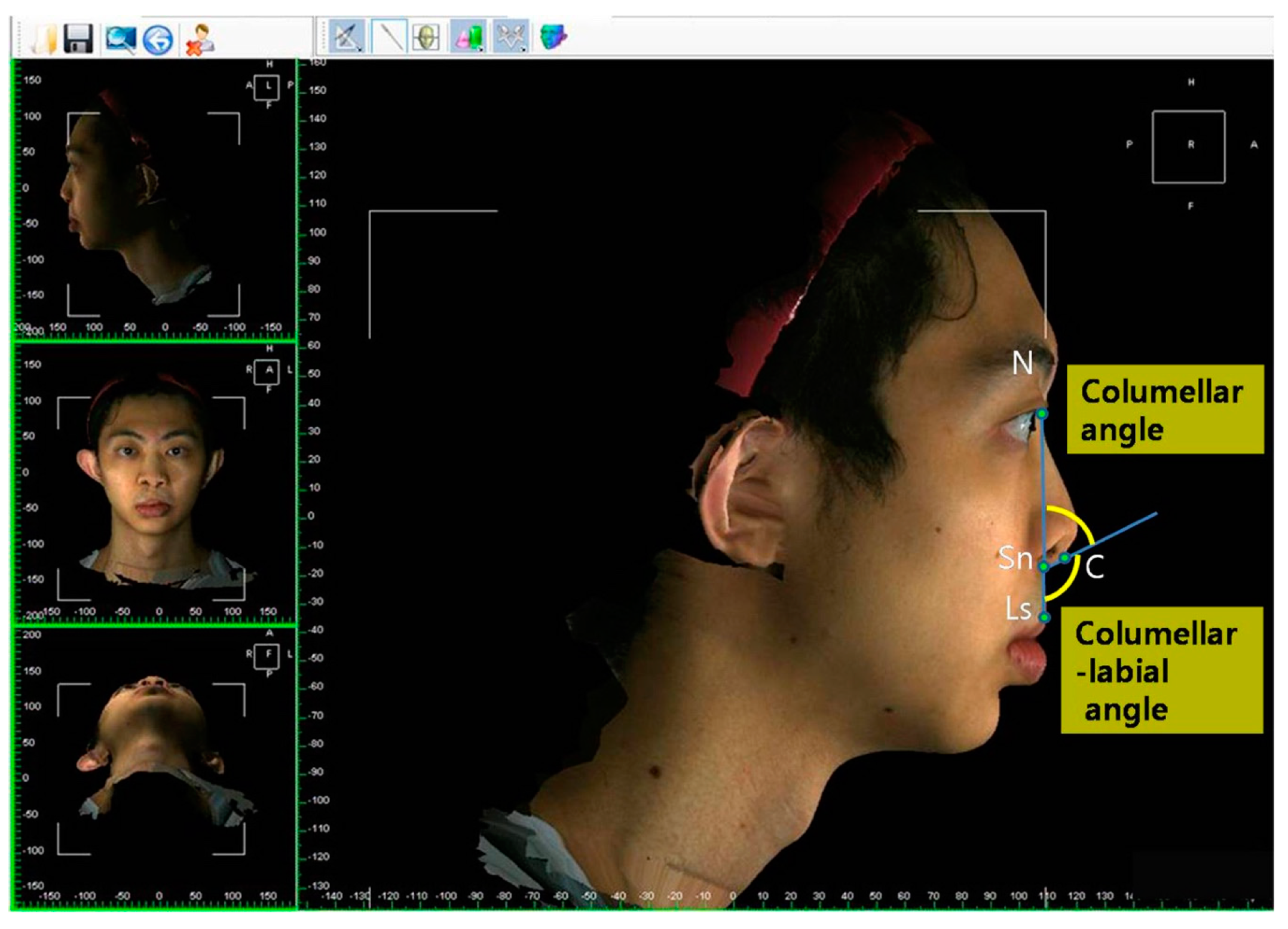
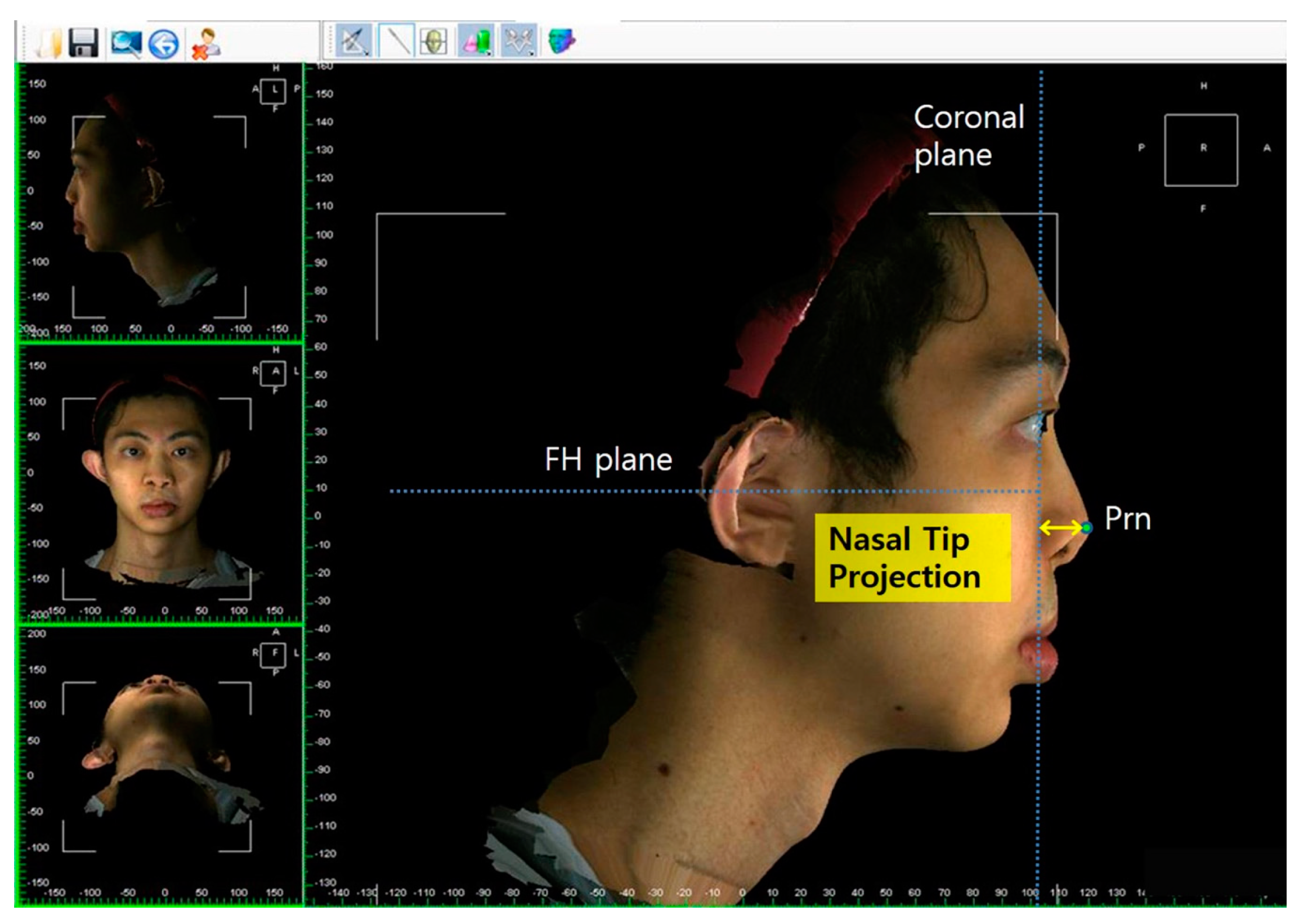
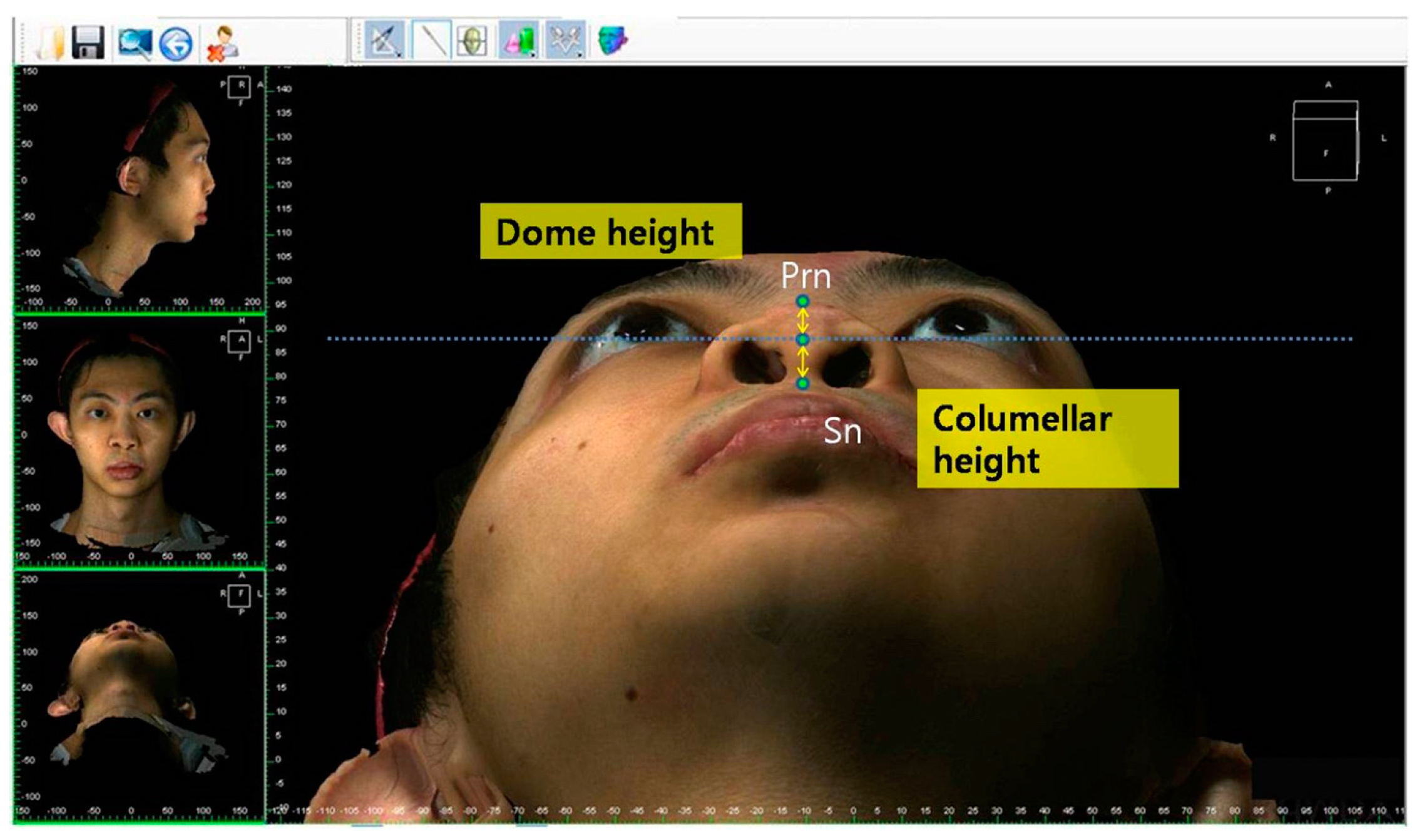
47]. Reference planes and measurements (10 linear, 4 angular, 6 proportional, 1 surface area, and 1 volume parameter;
Figure 2,
Figure 3,
Figure 4,
Figure 5,
Figure 6 and
Figure 7;
Table 1) were standardized based on previous nasal photogrammetric studies [
28,
29,
30,
31,
32,
33,
34,
35,
36,
37,
38,
43,
48,
49,
50,
51]. A standard reference frame (horizontal, coronal, and sagittal plane) was set up before all landmark identifications. The zoom and rotation tools were adopted to properly identify and set the landmarks on the 3D nasal surface. All photogrammetric measurements were collected in duplicate by two independent evaluators, with a 1-month interval between each measurement, and the mean was used for analysis.
2.4. Statistical Analysis
The data distribution was verified by the Kolmogorov–Smirnov test, and the parametric independent t-test or non-parametric Mann–Whitney U test was performed accordingly. Intra- and inter-examiner reliabilities were analyzed with intraclass correlation coefficients (ICCs) based on a two-way random-effects model. For all tests, p < 0.05 was considered statistically significant. All analyses were performed using SPSS Version 20.0 (IBM Corp., Armonk, NY, USA).
4. Discussion
From a historical point of view, the reconstruction of nasal deformities in those with BCLP during the growth period has been considered unacceptable because of concern that early nasal repair may interfere with future nasal growth. This is exemplified by what Aufricht said in 1955: “please do not touch the nasal tip until the child is at least a teenager” [
17]. This dictum has been clinically challenged over time by the benefits of rhinoplasty performed at infancy, including improvement of nasal symmetry, balance, and aesthetics, and by attenuation of the patient/parental psychosocial burden [
7,
8,
9,
10,
11,
12,
13,
14,
15,
16,
21,
22,
23,
24,
25,
26,
27]. However, a recent survey demonstrated that one-half of cleft surgeons continue to deny these potential benefits to their patients [
20], mainly because of the hypothetical disturbance in nasal growth, which remains an open question in cleft care [
17,
18,
19].
Most previous studies attempting to clarify this issue have limited nasal measurements to childhood and teenage years [
17,
18,
19,
21,
23,
24,
25,
27]. Furthermore, investigations reporting nasal growth data at maturity have included only a limited number of patients and the measurements have solely been based on the subjective opinion of the treating surgeon or two-dimensional photogrammetry of a single parameter (columellar–labial angle) [
22,
26]. In our study, we adopted a detailed quantitative evaluation of the nose from different perspectives, including measurements of full-nose structure (area surface and volume), and linear, angular, and proportional dimensions within and between the nasal subunits (dorsum, tip, and columella). In order to assess the two approaches to rhinoplasty (primary rhinoplasty and primary plus intermediate rhinoplasty), we evaluated the data distribution by sex, and compared both approaches to matched normal subjects. For this purpose, a comprehensive 3D nasal photogrammetric analysis was performed, based on prior studies that reported nasal growth in a normal healthy population and evaluated different endpoints in cleft lip and nose repair [
28,
29,
30,
31,
32,
33,
34,
35,
36,
37,
38,
43,
48,
49,
50,
51]. Our excellent intra-and inter-evaluator reliability scores support the rigorous validation process previously performed for the 3D photogrammetric system [
45,
46]. As the same reference planes and parameter definitions were consistently used for all measurements, it was expected that intrinsic errors associated with the 3D system would have been similar in all included subjects, with no or minimum interference with the intragroup and intergroup comparisons. Additionally, as 3D data were collected from healthy, normal individuals matched for sex, age, and ethnic group, valid deductions could be made from these comparisons.
Different parameters in the literature (e.g., nasal protrusion, nasal height, columellar-labial angle, and nasal volume) have been defined as relevant in assessing nasal growth in normal subjects and patients with cleft lip and palate [
24,
25,
26,
27,
34,
35,
36,
37,
38,
43]. Using exactly the same definitions for nasal growth-related parameters [
24,
25,
26,
27,
34,
35,
36,
37,
38,
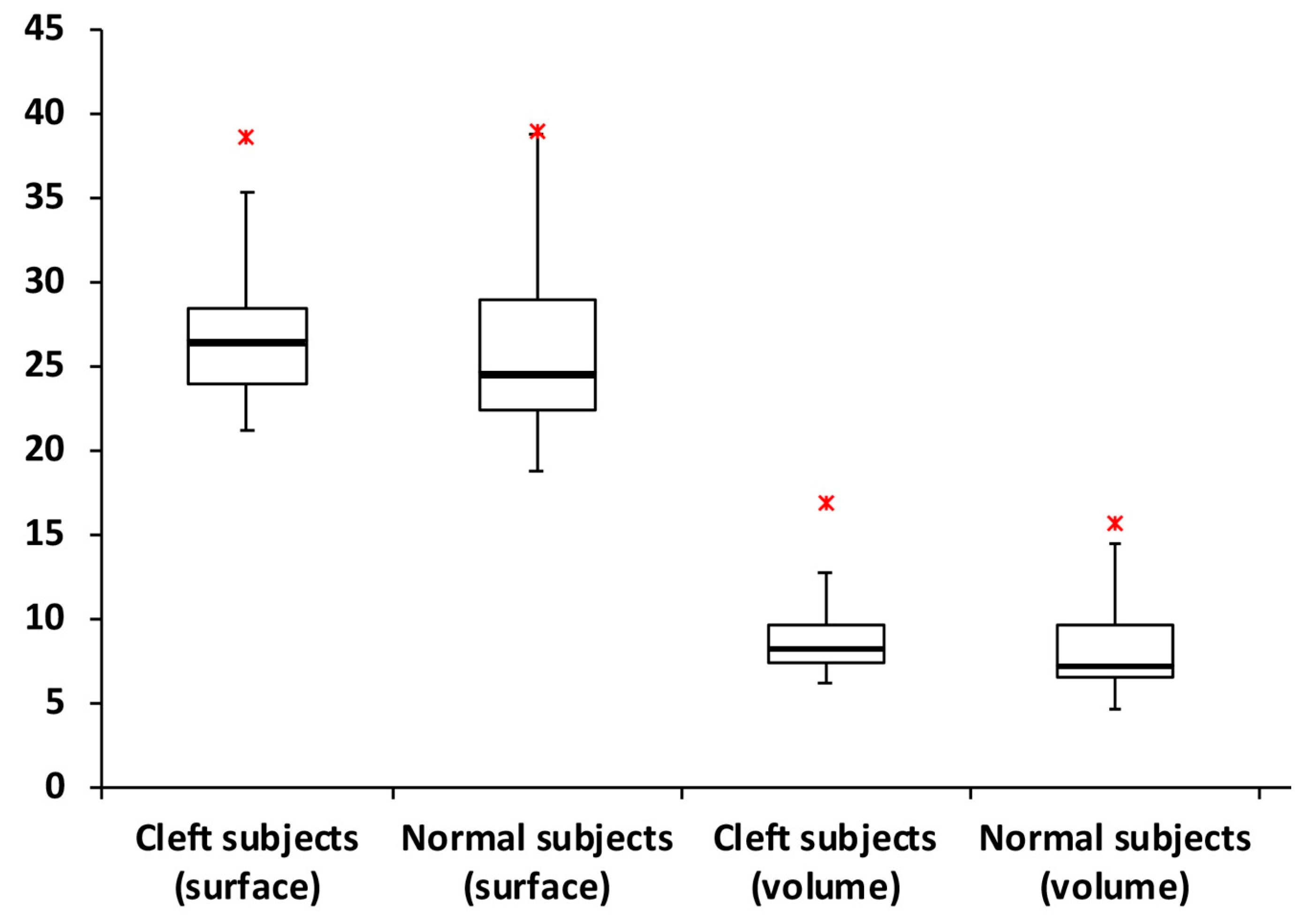
43], this study showed that primary rhinoplasty does not impair linear, angular, and proportional dimensions of the nose in patients with complete BCLP who reach maturity. This study also showed that mature patients with BCLP who have undergone primary rhinoplasty had nasal surface area and nasal volume similar to those of normal subjects. These two particular parameters are extremely important for nasal growth investigations, as they indicate that significant differences in linear, angular, and proportional parameters are not associated with nasal growth disturbance, but rather with the trajectory of growth causing residual nasal deformity at maturity.
Based on our findings, patients with BCLP presented with four main clinical differences compared to normal subjects, including a longer columella (statistically revealed by a greater columellar height and similar dome-to-columella ratio), cephalic rotation of the nasal tip (smaller columella angle and nasal bridge length and greater columellar–labial angle, nasal protrusion, and nasal tip height ratio), insufficient nasal tip projection (smaller nasal tip projection and greater nasal tip angle), and greater alar parameters (greater alar width, alar width/intercanthal distance ratio, alar width/mouth width ratio, and nasal index). Overall, these characteristics are consistent with the typical clinical manifestations of bilateral cleft lip nasal deformity. While the adopted techniques (presurgical NAM, primary rhinoplasty with or without intermediate surgery, and use of a postsurgical nasal retainer) were successful in correcting the typical short columella, the other features were not addressed properly. Unsatisfactory clinical results were found in previous studies [
8,
14,
24,
25,
26,
27]: caudal attachment of the columella base to the premaxilla and scarring process with downward drift of the columella base may explain the cephalic rotation of the nasal tip; inadequate repositioning of lower lateral cartilages during the primary and intermediate rhinoplasty procedures may result in insufficient nasal tip projection and greater alar width; and the greater alar width feature may be further justified by the presence of a narrow mouth width as a consequence of transposition of lateral lip elements below the prolabium during primary repair of bilateral cleft lip deformity.
Despite the benefits of primary rhinoplasty for nasal reconstruction [
7,
8,
9,
10,
11,
12,
13,
14,
15,
16,
21,
22,
23,
24,
25,
26,
27,
39], some patients may require additional nasal surgical intervention at preschool age (intermediate rhinoplasty) to address a residual tip-related deformity, as this is the most critical period of psychosocial development [
40,
52,
53,
54]. If nasal growth disturbance after primary rhinoplasty is secondary to development of heavy scar tissue, as theorized in traditional teaching, patients with two rhinoplasties within the first 6 years of life would have an even greater nasal growth restriction when they reached maturity. However, we found no significant differences for all but one parameter when patients with only primary rhinoplasty were compared with those who underwent primary plus intermediate rhinoplasty. This further supports that primary rhinoplasty is not a harmful procedure, even in patients with cleft lip and palate who undergo two nasal tip surgeries during the growth period.
The evolution of bilateral cleft lip nasal management has led to a group of patients who have undergone primary plus intermediate rhinoplasty. The included patients were treated when presurgical NAM was initiated at our center [
39,
40,
41,
42]. While some of the unsatisfactory results may be explained by failure of NAM to achieve narrowing of the cleft width, the closed primary rhinoplasty technique also failed to attain satisfactory nasal tip reconstruction. Moreover, intermediate rhinoplasty may not have completely resolved residual nasal deformity after unsuccessful primary rhinoplasty, as demonstrated by the current data. We followed up our patients with BCLP over time and our surgical protocol evolved to address each new challenge. All technical modifications implemented over the past 20 years represent a continuous effort to provide our patients with a more predictable long-term outcome. Therefore, the protocol used when patients in this study were first treated differed from the present protocol. Currently, patients with BCLP are treated with a modified NAM approach and a semi-open primary rhinoplasty technique, with overcorrection using the Tajima reverse-U incision for release of interdomal fibrofatty tissue and proper repositioning of the lower lateral cartilages. Preliminary clinical results have demonstrated almost no need for intermediate rhinoplasty, but a study with long-term follow-up is still needed to objectively quantify the intermediate rhinoplasty rate and to monitor the effect of the current approach on nasal growth at maturity.
Based on the current and previous findings [
17,
18,
19,
21,
22,
23,
24,
25,
26,
27], primary rhinoplasty with or without an intermediate procedure should be advocated as a routine intervention for complete BCLP reconstruction, with no risk of potential compromise of normal nasal dimensions. The “no-touch” approach to the nose should be replaced by primary rhinoplasty performed by surgeons devoted to cleft surgery, using a meticulous technique in accordance with published principles [
1,
2,
3]. This paradigm shift in cleft care definitely depends on further scientific evidence from future outcome studies by other senior surgeons as well as the reevaluation of multi-center studies conducted two decades ago [
55]. Meanwhile, young surgeons can interpret and apply the present results in their cleft practice, as this study is based on bilateral cleft lip nasal reconstructions performed by a single surgeon in his first years of practice.
Some inherent limitations to this retrospective study design may have affected our results and must be considered when interpreting our findings. Our center practices primary rhinoplasty exclusively, and thus patients without primary rhinoplasty were not included in our study [
39,
40,
41,
42]. Additionally, we did not include different techniques for primary and intermediate bilateral cleft lip nasal reconstruction for additional comparisons, but we did select normal subjects as our controls, as we assumed that the endpoint of bilateral cleft lip nasal reconstruction should be normal nasal morphology. While a normal nose is theoretically possible, it is not always achievable in all patients. Multiple factors other than growth disturbance, including the severity of initial deformity and the limitations of the repair technique, may influence the final nasal outcome at maturity. Therefore, nasal repair after completion of craniofacial growth (secondary rhinoplasty) is frequently needed to improve both aesthetic and functional aspects in patients with BCLP [
52,
53,
54]. Thus, our observations on residual nasal deformities may be useful for preoperative planning, as specific technical maneuvers can be used to address each type of deformity. Although we did not control for occlusal status, patients underwent standard cleft palate repair (two-flap palatoplasty) and secondary alveolar reconstruction with iliac bone grafting [
56] to attenuate its influence in comparative analysis between primary rhinoplasty only and primary plus intermediate rhinoplasty approaches.
Despite these limitations, our 3D-based findings provide valuable information to guide the decision-making process of cleft teams and to set realistic parental expectations before primary rhinoplasty by predicting nasal growth and the status of residual deformities at maturity.












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}