Ceftaroline Efficacy and Safety in Treatment of Complicated Skin and Soft Tissue Infection: A Systemic Review and Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Search and Selection
2.2. Definitions and Outcomes
2.3. Data Analysis
3. Results
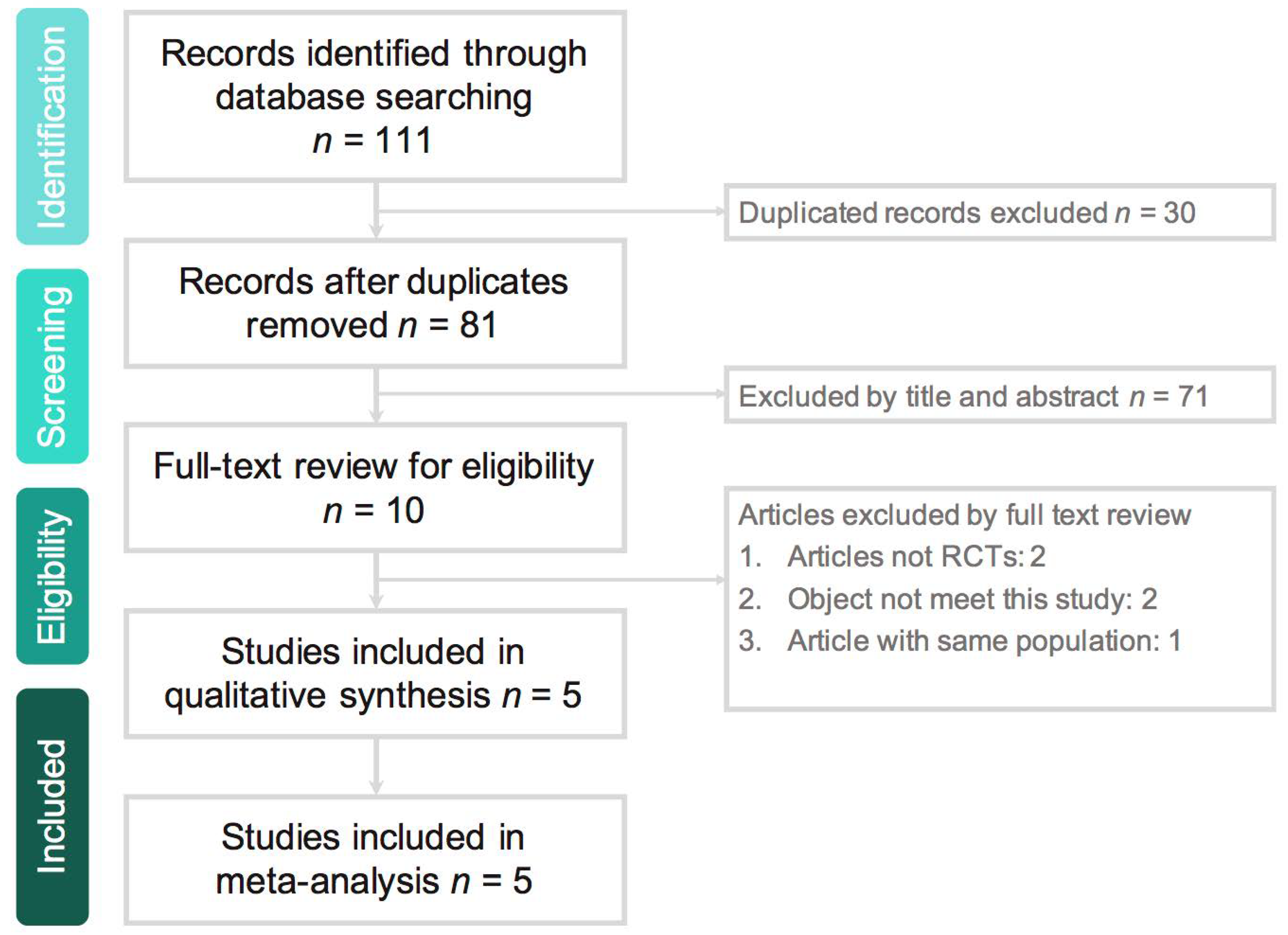
3.1. Study Selection and Characteristics
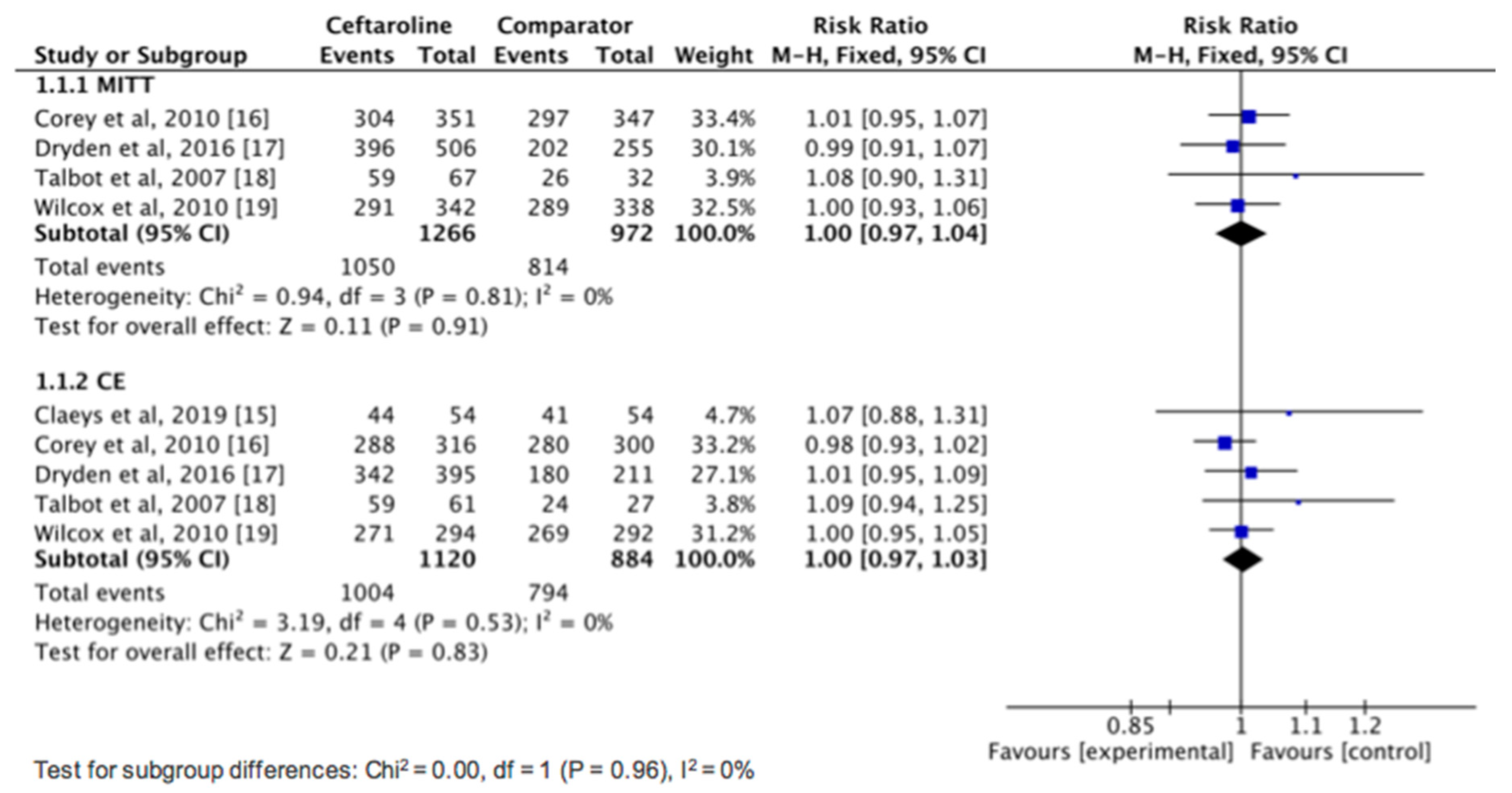
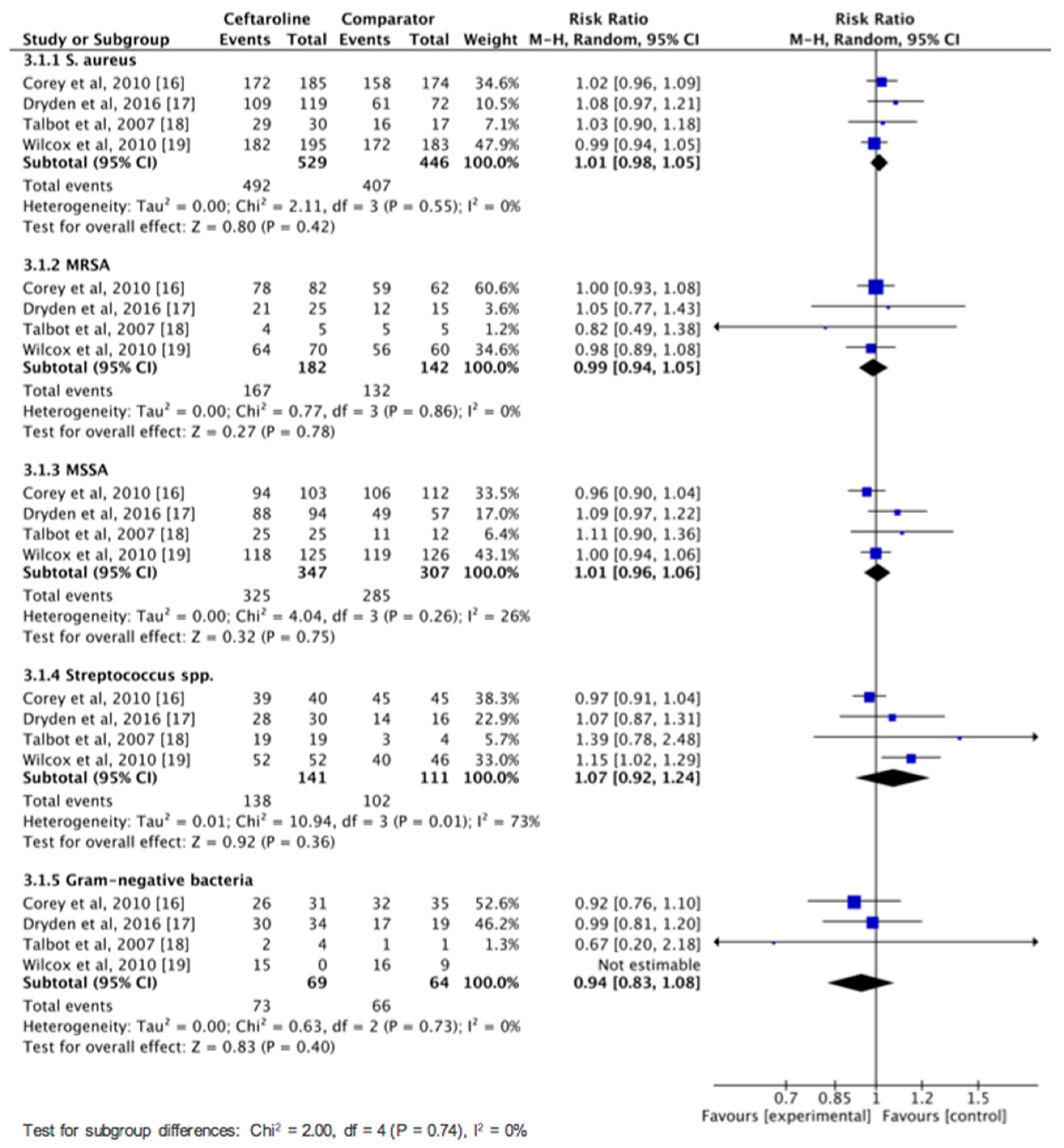
3.2. Clinical Efficacy and Microbiologic Response
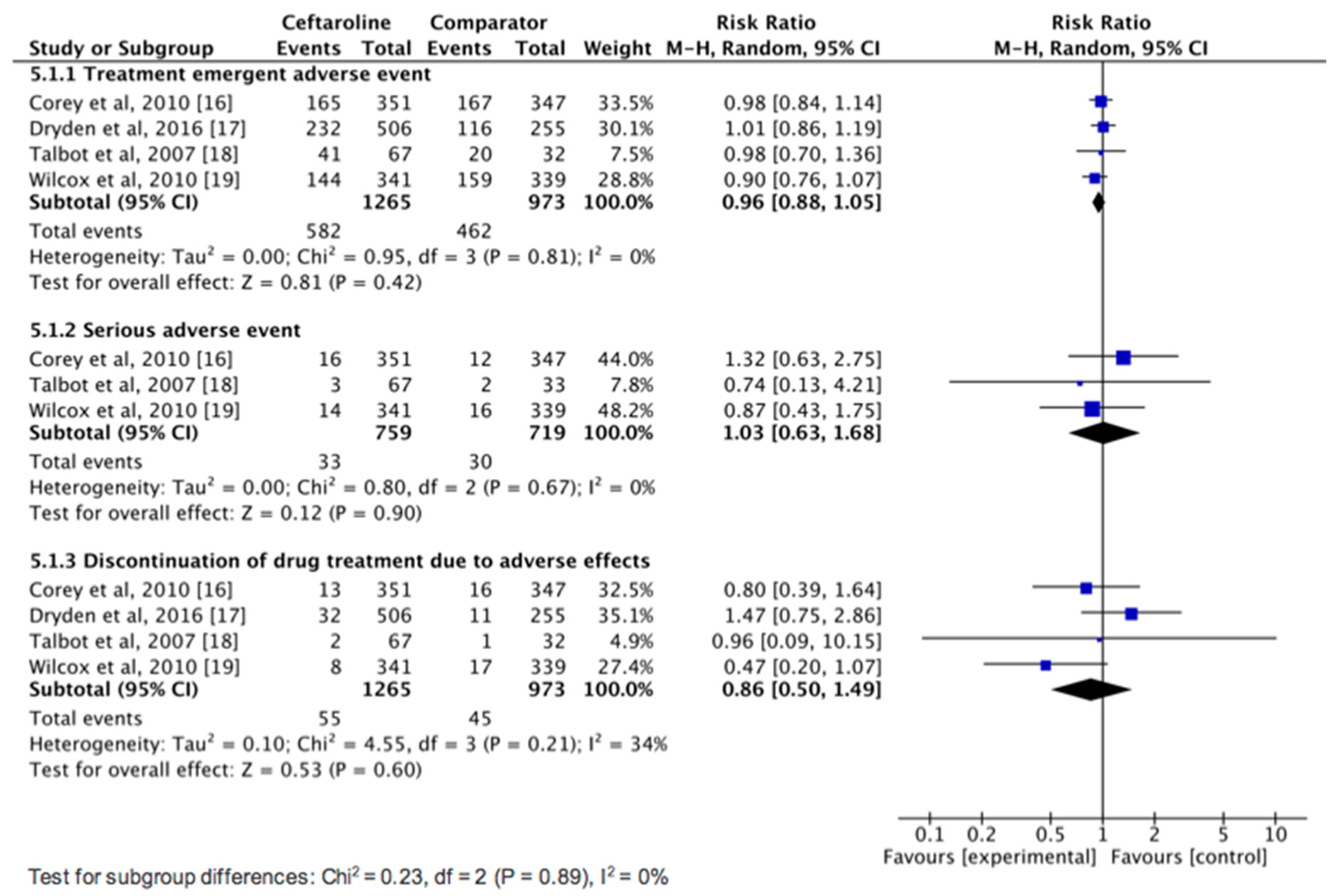
3.3. AEs
4. Discussion
Author Contributions
Conflicts of Interest
References
- Edelsberg, J.; Taneja, C.; Zervos, M.; Haque, N.; Moore, C.; Reyes, K.; Oster, G. Trends in US hospital admissions for skin and soft tissue infections. Emerg. Infect. Dis. 2009, 15, 1516–1518. [Google Scholar] [CrossRef]
- Klein, E.Y.; Mojica, N.; Jiang, W.; Cosgrove, S.E.; Septimus, E.; Morgan, D.J.; Laxminarayan, R. Trends in methicillin-resistant Staphylococcus aureus hospitalizations in the United States, 2010–2014. Clin. Infect. Dis. 2017, 65, 1921–1923. [Google Scholar] [CrossRef] [PubMed]
- Kaye, K.S.; Patel, D.A.; Stephens, J.M.; Khachatryan, A.; Patel, A.; Johnson, K. Rising United States hospital admissions for acute bacterial skin and skin structure infections: Recent trends and economic impact. PLoS ONE 2015, 10, e0143276. [Google Scholar] [CrossRef] [PubMed]
- Stryjewski, M.E.; Chambers, H.F. Skin and soft-tissue infections caused by community-acquired methicillin-resistant Staphylococcus aureus. Clin. Infect. Dis. 2008, 46, S368–S377. [Google Scholar] [CrossRef] [PubMed]
- Stevens, D.L.; Bisno, A.L.; Chambers, H.F.; Everett, E.D.; Dellinger, P.; Goldstein, E.J.; Wade, J.C. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2014, 59, e10–e52. [Google Scholar] [CrossRef]
- Jorgenson, M.R.; DePestel, D.D.; Carver, P.L. Ceftaroline fosamil: A novel broad-spectrum cephalosporin with activity against methicillin-resistant Staphylococcus aureus. Ann. Pharmacother. 2011, 45, 1384–1398. [Google Scholar] [CrossRef]
- Poon, H.; Chang, M.H.; Fung, H.B. Ceftaroline fosamil: A cephalosporin with activity against methicillin-resistant Staphylococcus aureus. Clin. Ther. 2012, 34, 743–765. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Mendes, R.E.; Castanheira, M.; Flamm, R.K.; Jones, R.N.; Sader, H.S. Ceftaroline activity tested against bacterial isolates causing community-acquired respiratory tract infections and skin and skin structure infections in pediatric patients from United States hospitals: 2012–2014. Pediatr. Infect. Dis. J. 2017, 36, 486–491. [Google Scholar] [CrossRef]
- Rolston, K.V.I.; Jamal, M.A.; Nesher, L.; Shelburne, S.A.; Raad, I.; Prince, R.A. In vitro activity of ceftaroline and comparator agents against Gram-positive and Gram-negative clinical isolates from cancer patients. Int. J. Antimicrob. Agents 2017, 49, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Farrell, D.J.; Castanheira, M.; Mendes, R.E.; Sader, H.S.; Jones, R.N. In vitro activity of ceftaroline against multidrug-resistant Staphylococcus aureus and Streptococcus pneumoniae: A review of published studies and the AWARE Surveillance Program (2008–2010). Clin. Infect. Dis. 2012, 55, S206–S214. [Google Scholar] [CrossRef]
- Sader, H.S.; Farrell, D.J.; Flamm, R.K.; Jones, R.N. Antimicrobial Activity of ceftaroline tested against Staphylococcus aureus from surgical skin and skin structure infections in US medical centers. Surg. Infect. 2016, 17, 443–447. [Google Scholar] [CrossRef]
- Zhong, N.S.; Sun, T.; Zhuo, C.; D’Souza, G.; Lee, S.H.; Lan, N.H.; Melnick, D. Ceftaroline fosamil versus ceftriaxone for the treatment of Asian patients with community-acquired pneumonia: A randomised, controlled, double-blind, phase 3, non-inferiority with nested superiority trial. Lancet Infect. Dis. 2015, 15, 161–171. [Google Scholar] [CrossRef]
- File, T.M., Jr.; Low, D.E.; Eckburg, P.B.; Talbot, G.H.; Friedland, H.D.; Lee, J.; Pullman, J. FOCUS 1: A randomized, double-blinded, multicentre, Phase III trial of the efficacy and safety of ceftaroline fosamil versus ceftriaxone in community-acquired pneumonia. J. Antimicrob. Chemother. 2011, 66, 19–32. [Google Scholar] [CrossRef]
- Low, D.E.; File, T.M., Jr.; Eckburg, P.B.; Talbot, G.H.; David Friedland, H.; Lee, J.; Corral, J. FOCUS 2: A randomized, double-blinded, multicentre, Phase III trial of the efficacy and safety of ceftaroline fosamil versus ceftriaxone in community-acquired pneumonia. J. Antimicrob. Chemother. 2011, 66, 33–44. [Google Scholar] [CrossRef]
- Claeys, K.C.; Zasowski, E.J.; Trinh, T.D.; Casapao, A.M.; Pogue, J.M.; Bhatia, N.; Sherwin, R. Open-label randomized trial of early clinical outcomes of ceftaroline fosamil versus vancomycin for the treatment of acute bacterial skin and skin structure infections at risk of methicillin-resistant Staphylococcus aureus. Infect. Dis. Ther. 2019, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Corey, G.R.; Wilcox, M.H.; Talbot, G.H.; Thye, D.; Friedland, D.; Baculik, T. CANVAS 1: The first Phase III, randomized, double-blind study evaluating ceftaroline fosamil for the treatment of patients with complicated skin and skin structure infections. J. Antimicrob. Chemother. 2010, 65, 41–51. [Google Scholar] [CrossRef]
- Dryden, M.; Zhang, Y.; Wilson, D.; Iaconis, J.P.; Gonzalez, J. A Phase III, randomized, controlled, non-inferiority trial of ceftaroline fosamil 600 mg every 8 h versus vancomycin plus aztreonam in patients with complicated skin and soft tissue infection with systemic inflammatory response or underlying comorbidities. J. Antimicrob. Chemother. 2016, 71, 3575–3584. [Google Scholar] [CrossRef]
- Talbot, G.H.; Thye, D.; Das, A.; Ge, Y. Phase 2 study of ceftaroline versus standard therapy in treatment of complicated skin and skin structure infections. Antimicrob. Agents Chemother. 2007, 51, 3612–3616. [Google Scholar] [CrossRef]
- Wilcox, M.H.; Corey, G.R.; Talbot, G.H.; Thye, D.; Friedland, D.; Baculik, T. CANVAS 2: The second Phase III, randomized, double-blind study evaluating ceftaroline fosamil for the treatment of patients with complicated skin and skin structure infections. J. Antimicrob. Chemother. 2010, 65, iv53–iv65. [Google Scholar] [CrossRef]
- Sotgiu, G.; Aliberti, S.; Gramegna, A.; Mantero, M.; Di Pasquale, M.; Trogu, F.; Blasi, F. Efficacy and effectiveness of Ceftaroline Fosamil in patients with pneumonia: A systematic review and meta-analysis. Respir. Res. 2018, 19, 205. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Bmj 2011, 343, d5928. [Google Scholar] [CrossRef]
- El Hajj, M.S.; Turgeon, R.D.; Wilby, K.J. Ceftaroline fosamil for community-acquired pneumonia and skin and skin structure infections: A systematic review. Int. J. Clin. Pharm. 2017, 39, 26–32. [Google Scholar] [CrossRef]
- Sader, H.S.; Mendes, R.E.; Streit, J.M.; Flamm, R.K. Antimicrobial susceptibility trends among Staphylococcus aureus isolates from U.S. Hospitals: Results from 7 Years of the Ceftaroline (AWARE) surveillance program, 2010 to 2016. Antimicrob. Agents Chemother. 2017, 61, e01043–e01117. [Google Scholar] [CrossRef]
- Sader, H.S.; Farrell, D.J.; Flamm, R.K.; Jones, R.N. Activity of ceftaroline and comparator agents tested against Staphylococcus aureus from patients with bloodstream infections in US medical centres (2009–13). J. Antimicrob. Chemother. 2015, 70, 2053–2056. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Published Year | Study Design | Study Site | No (Male Ratio, %) of Patients | Mean Age of Patients | Dose Regimen | |||
|---|---|---|---|---|---|---|---|---|
| Ceftaroline | Comparator | Ceftaroline | Comparator | Ceftaroline | Comparator | |||
| Talbot et al., 2007 [18] | Multicenter, randomized, observe-blinded (2:1) | 15 clinical sites in USA, South America, South Africa, Russia | 67 (55.2) | 33 (59.4) | 41.6 | 44.0 | 600 mg q12h | Vancomycin 1 g q12h ± aztreonam 1 g q8h |
| Corey et al., 2010 [16] | Multicenter, randomized, double-blind (1:1) | 55 sites in 10 countries | 351 (62.7) | 347 (62.8) | 47.2 | 49.2 | 600 mg q12h | Vancomycin 1 g q12h + aztreonam 1 g q12h |
| Wilcox et al., 2010 [19] | Multicenter, randomized, double-blind (1:1) | 56 sites in 12 countries | 348 (65.5) | 346 (59.5) | 47.8 | 47.5 | 600 mg q12h | Vancomycin 1 g q12h + aztreonam 1 g q12h |
| Dryden et al., 2016 [17] | Multicenter, randomized, double-blind (2:1) | 111 sites in 28 countries | 506 (61.3) | 255 (58.0) | 52.6 | 53.6 | 600 mg q8h | Vancomycin 15 mg/kg q12h + aztreonam 1 g q8h |
| Claeys et al., 2019 [15] | Multicenter, randomized, double-blind (1:1) | 3 sites in USA | 54 (NA) | 54 (NA) | 54.8 | 48.1 | ± metronidazole * | Vancomycin ± ceftriaxone ± metronidazole or ampicillin/sulbactam * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lan, S.-H.; Chang, S.-P.; Lai, C.-C.; Lu, L.-C.; Chao, C.-M. Ceftaroline Efficacy and Safety in Treatment of Complicated Skin and Soft Tissue Infection: A Systemic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2019, 8, 776. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8060776
Lan S-H, Chang S-P, Lai C-C, Lu L-C, Chao C-M. Ceftaroline Efficacy and Safety in Treatment of Complicated Skin and Soft Tissue Infection: A Systemic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2019; 8(6):776. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8060776
Chicago/Turabian StyleLan, Shao-Huan, Shen-Peng Chang, Chih-Cheng Lai, Li-Chin Lu, and Chien-Ming Chao. 2019. "Ceftaroline Efficacy and Safety in Treatment of Complicated Skin and Soft Tissue Infection: A Systemic Review and Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 8, no. 6: 776. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8060776