Errors in Implant Positioning Due to Lack of Planning: A Clinical Case Report of New Prosthetic Materials and Solutions

 ,
, 
Abstract
:1. Introduction
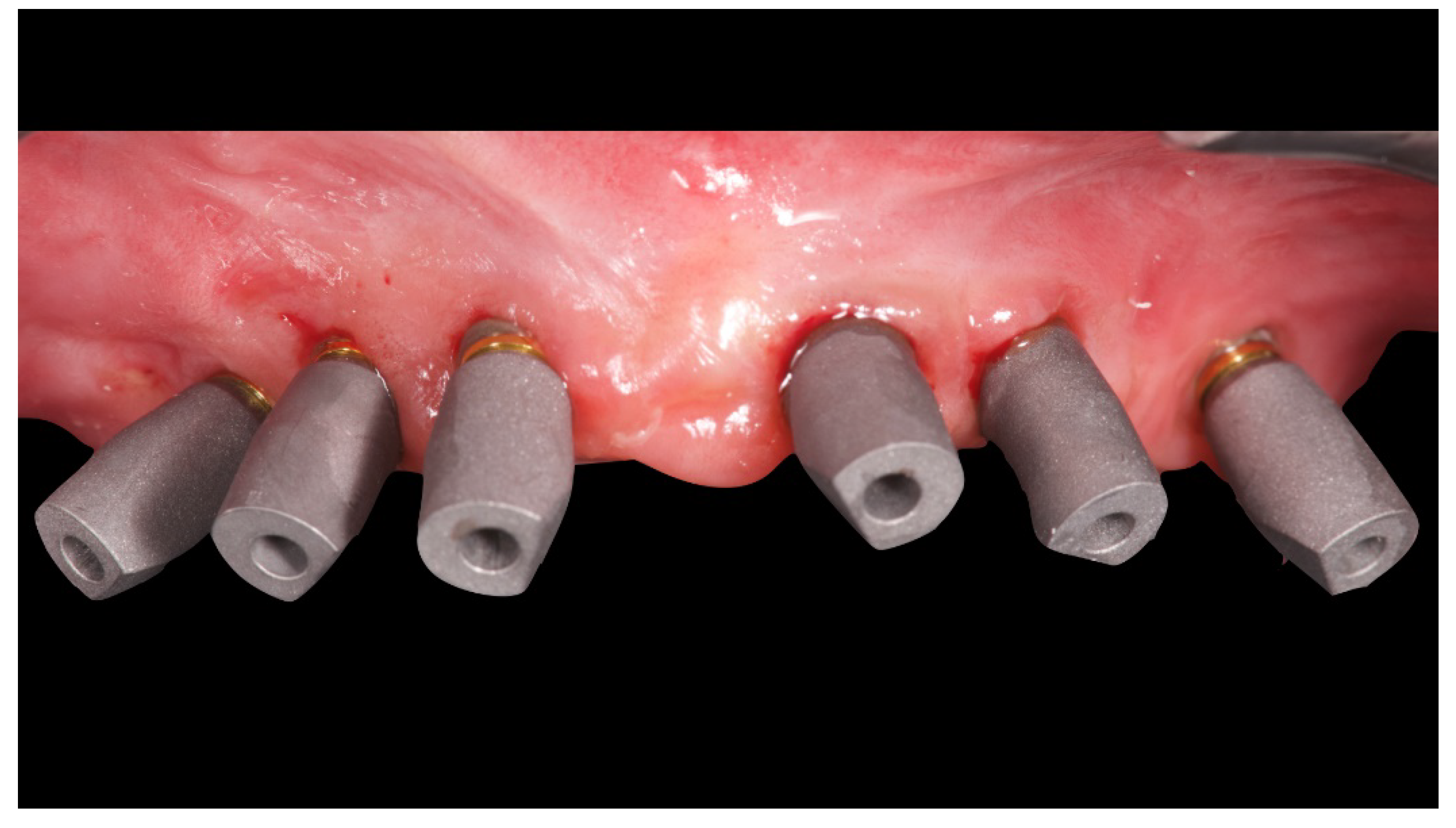
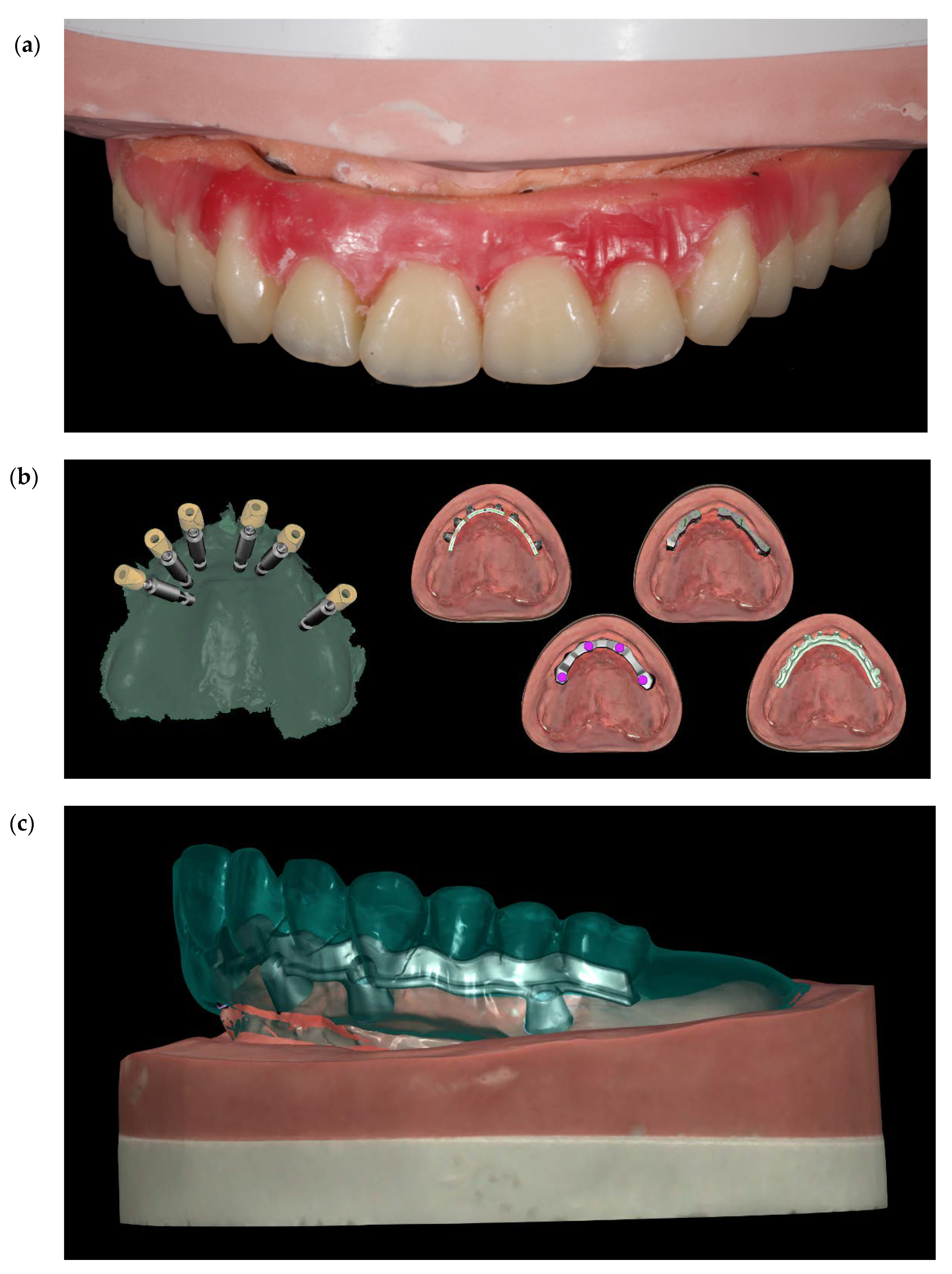
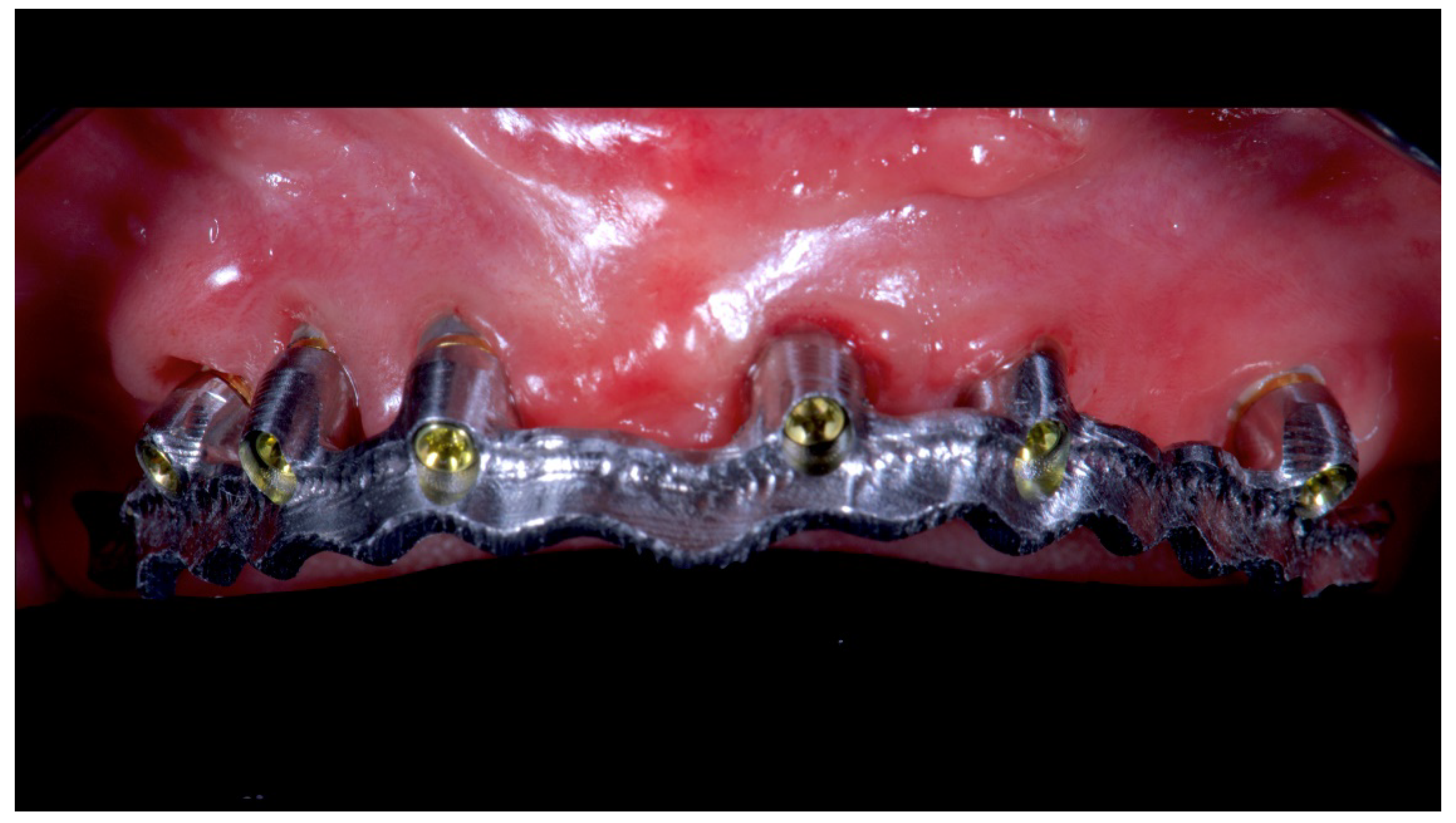
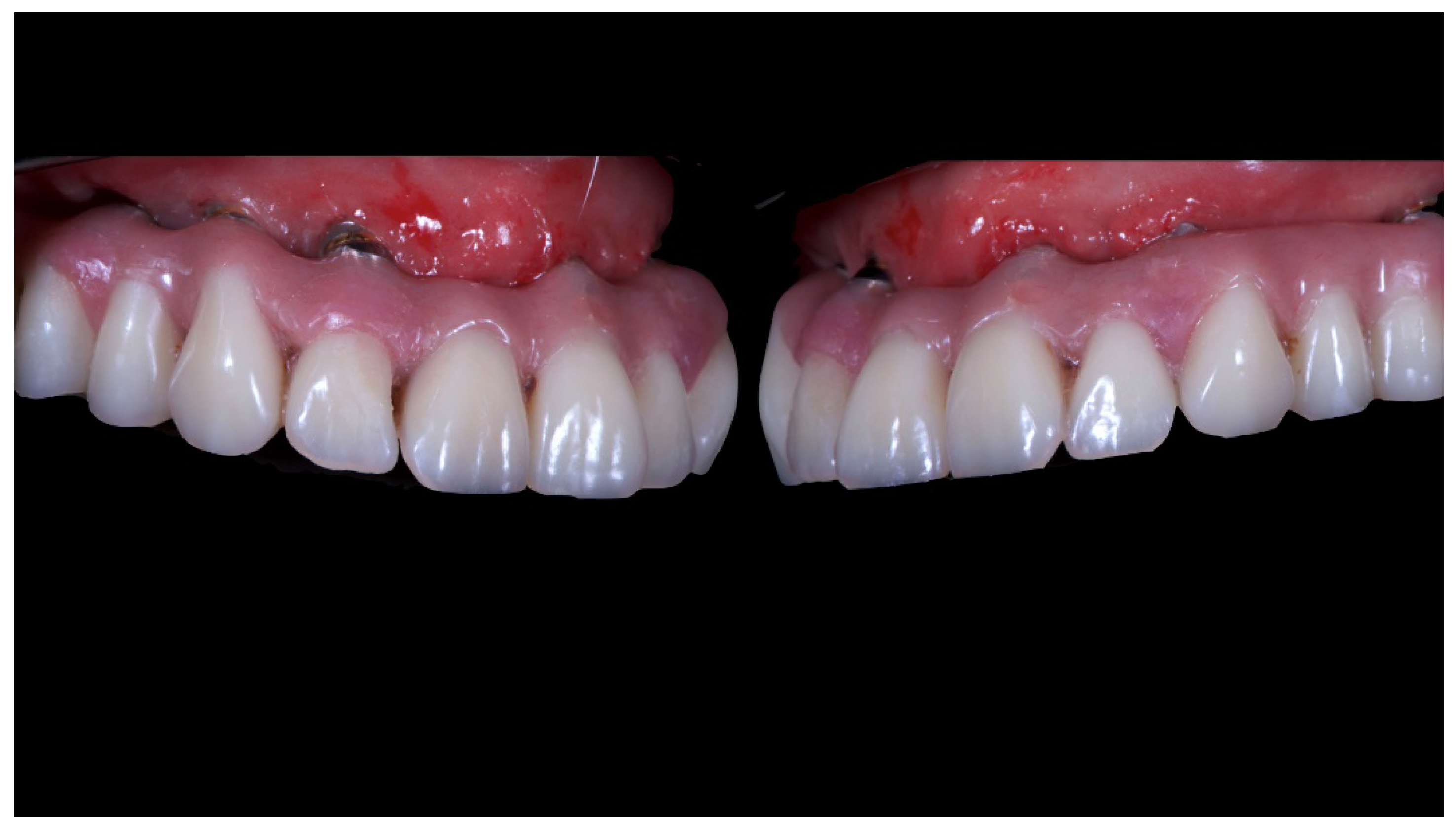
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Merli, M. Implant Therapy Vol. 1: Diagnosis and Surgical Therapy: The Integrated Treatment Plan, 1st ed.; Quintessence Publishing: Milan, Italy, 2012. [Google Scholar]
- Jiang, X.; Yao, Y.; Tang, W.; Han, D.; Zhang, L.; Zhao, K.; Wang, S.; Meng, Y. Design of dental implants at materials level: An overview. J. Biomed. Mater. Res. A 2020. [Google Scholar] [CrossRef] [PubMed]
- Kiatkroekkrai, P.; Takolpuckdee, C.; Subbalekha, K.; Mattheos, N.; Pimkhaokham, A. Accuracy of implant position when placed using static computer-assisted implant surgical guides manufactured with two different optical scanning techniques: A randomized clinical trial. Int. J. Oral Maxillofac. Surg. 2020, 49, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Zitzmann, N.U.; Margolin, M.D.; Filippi, A.; Weiger, R.; Krastl, G. Patient assessment and diagnosis in implant treatment. Aust. Dent. J. 2008, 53, S3–10. [Google Scholar] [CrossRef] [PubMed]
- Schneider, D.; Sancho-Puchades, M.; Mir-Marí, J.; Mühlemann, S.; Jung, R.; Hämmerle, C. A randomized controlled clinical trial comparing conventional and computer-assisted implant planning and placement in partially edentulous patients. Part 4: Accuracy of implant placement. Int. J. Periodontics Restor. Dent. 2019, 39, e111–e122. [Google Scholar] [CrossRef] [PubMed]
- Farley, N.E.; Kennedy, K.; McGlumphy, E.A.; Clelland, N.L. Split-mouth comparison of the accuracy of computer-generated and conven- tional surgical guides. Int. J. Oral Maxillofac. Implant. 2013, 28, 563–572. [Google Scholar] [CrossRef]
- Jung, R.E.; Schneider, D.; Ganeles, J.; Wismeijer, D.; Zwahlen, M.; Hammerle, C.H.; Tahmaseb, A. Computer technology applications in surgi-cal implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2009, 24, 92–109. [Google Scholar]
- Schneider, D.; Marquardt, P.; Zwahlen, M.; Jung, R.E. A systematic review on the accuracy and the clinical outcome of computer-guided template-based implant dentistry. Clin. Oral Implant. Res. 2009, 20, 73–86. [Google Scholar] [CrossRef] [Green Version]
- Tahmaseb, A.; Wismeijer, D.; Coucke, W.; Derksen, W. Computer technology applications in surgi-cal implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 25–42. [Google Scholar] [CrossRef] [Green Version]
- Tallarico, M.; Esposito, M.; Xhanari, E.; Caneva, M.; Meloni, S.M. Computer-guided vs freehand placement of immediately loaded dental implants: 5-year post-loading results of a randomised controlled trial. Eur. J. Oral Implant. 2018, 25, 1–11. [Google Scholar]
- Tallarico, M.; Meloni, S. Retrospective analysis on survival rate, template-related complications, and prevalence of peri-implantitis of 694 anodized implants placed using computer-guided surgery: Results between 1 and 10 years of follow-up. Int. J. Oral Maxillofac. Implant. 2017, 32, 1162–1171. [Google Scholar] [CrossRef]
- Tallarico, M.; Meloni, S.M.; Canullo, L.; Xhanari, E.; Polizzi, G. Guided surgery for single-implant placement: A critical review. J. Oral Sci. Rehabil. 2016, 2, 8–14. [Google Scholar]
- Tallarico, M.; Martinolli, M.; Kim, Y.-J.; Cocchi, F.; Meloni, S.M.; Alushi, A.; Xhanari, E. Accuracy of computer-assisted template-based implant placement using two different surgical templates designed with or without metallic sleeves: A randomized controlled trial. Dent. J. 2019, 7, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tallarico, M.; Kim, Y.-J.; Cocchi, F.; Martinolli, M.; Meloni, S.M. Accuracy of newly developed sleeve-designed templates for insertion of dental implants: A prospective multicenters clinical trial. Clin. Implant Dent. Relat. Res. 2018, 11, 203–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tallarico, M.; Caneva, M.; Baldini, N.; Gatti, F.; Duvina, M.; Billi, M.; Iannello, G.; Piacentini, G.; Meloni, S.M.; Cicciù, M. Patient-centered rehabilitation of single, partial, and complete edentulism with cemented-or screw-retained fixed dental prosthesis: The first osstem advanced dental implant research and education center consensus conference 2017. Eur. J. Dent. 2018, 12, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, A.; Tallarico, M.; Mangani, F.; Barlattani, A. Different implant impression techniques for edentulous patients treated with CAD/CAM complete-arch prostheses: a randomised controlled trial reporting data at 3 year post-loading. Eur. J. Oral Implant. 2013, 6, 325–340. [Google Scholar]
- Abduo, J.; Bennani, V.; Waddell, N.; Lyons, K.; Swain, M. Assessing the fit of implant fixed prostheses: A critical review. Int. J. Oral Maxillofac. Implant. 2010, 25, 506–515. [Google Scholar]
- Eisenmann, E.; Mokabberi, A.; Walter, M.H.; Freesmeyer, W.B. Improving the fit of implant-supported superstructures using the spark erosion technique. Int. J. Oral Maxillofac. Implant. 2004, 19, 810–818. [Google Scholar]
- Scrascia, R.; Fiorillo, L.; Gaita, V.; Secondo, L.; Nicita, F.; Cervino, G. Implant-supported prosthesis for edentulous patient rehabilitation from temporary prosthesis to definitive with a new protocol: A single case report. Prosthesis 2020, 1, 10–24. [Google Scholar]
- Avrampou, M.; Mericske-Stern, R.; Blatz, M.B.; Katsoulis, J. Virtual implant planning in the edentulous maxilla: Criteria for decision-making of prosthesis design. Clin. Oral Implant. Res. 2013, 24, 152–159. [Google Scholar] [CrossRef]
- Garber, D.A. The esthetic dental implant: letting restoration be the guide. J. Am. Dent. Assoc. 1995, 126, 319–325. [Google Scholar] [CrossRef]
- Meloni, S.M.; Tallarico, M.; Pisano, M.; Xhanari, E.; Canullo, L. Immediate loading of fixed complete denture prosthesis supported by 4–8 implants placed using guided surgery: A 5-year prospective study on 66 patients with 356 implants. Clin. Implant Dent. Relat. Res. 2016, 37, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Ganz, S.D. Presurgical planning with ct-derived fabrication of surgical guides. J. Oral Maxillofac. Surg. 2005, 63, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, A.; Tallarico, M.; Moy, P.K. Immediate loading with a novel implant featured by variable-threaded geometry, internal conical connection and platform shifting: Three-year results from a prospective cohort study. Eur. J. Oral. Implant. 2015, 8, 51–63. [Google Scholar]
- Tallarico, M.; Vaccarella, A.; Marzi, G.C.; Alviani, A.; Campana, V. A prospective case-control clinical trial comparing 1-and 2-stage Nobel Biocare TiUnite implants: Resonance frequency analysis assessed by Osstell Mentor during integration. Quintessence Int. 2011, 42, 635–644. [Google Scholar] [PubMed]
- Meloni, S.M.; Jovanovic, S.A.; Urban, I.; Baldoni, E.; Pisano, M.; Tallarico, M. Horizontal ridge augmentation using GBR with a native collagen membrane and 1:1 ratio of particulate xenograft and autologous bone: A 3-year after final loading prospective clinical study. Clin. Implant Dent. Relat. Res. 2019, 12, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, G.; Lo Giudice, R.; Matarese, G.; Giudice, G.L.; Isola, G.; Cicciù, M.; Palaia, G.; Romeo, U. Evaluation of magnification systems in restorative dentistry. An In-Vitro study. Dent. Cadmos 2015, 83, 296–305. [Google Scholar] [CrossRef]
- Cicciù, M.; Risitano, G.; Lo Giudice, G.; Bramanti, E.E. Periodontal health and caries prevalence evaluation in patients affected by parkinson’s disease. Parkinson Disease 2012, 2012, 541908. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Spagnuolo, G.; Bramanti, E.; Laino, L.; Lauritano, F.; Cicciù, M. Interface between MTA and dental bonding agents: Scanning electron microscope evaluation. J. Int. Soc. Prev. Community Dent. 2017, 7, 64–68. [Google Scholar]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Benefits | Risks |
|---|---|
| Minamally invasive approach | Peri-implantitis |
| Low cost for patient | Technical problems |
| reliability |
| Benefits | Risks |
|---|---|
| Accurate implant position | Needs for GBR |
| No surface exposure | Failure of the New Implants |
| Surgical complications | |
| Higher cost |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tallarico, M.; Scrascia, R.; Annucci, M.; Meloni, S.M.; Lumbau, A.I.; Koshovari, A.; Xhanari, E.; Martinolli, M. Errors in Implant Positioning Due to Lack of Planning: A Clinical Case Report of New Prosthetic Materials and Solutions. Materials 2020, 13, 1883. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13081883
Tallarico M, Scrascia R, Annucci M, Meloni SM, Lumbau AI, Koshovari A, Xhanari E, Martinolli M. Errors in Implant Positioning Due to Lack of Planning: A Clinical Case Report of New Prosthetic Materials and Solutions. Materials. 2020; 13(8):1883. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13081883
Chicago/Turabian StyleTallarico, Marco, Roberto Scrascia, Marco Annucci, Silvio Mario Meloni, Aurea Immacolata Lumbau, Alba Koshovari, Erta Xhanari, and Matteo Martinolli. 2020. "Errors in Implant Positioning Due to Lack of Planning: A Clinical Case Report of New Prosthetic Materials and Solutions" Materials 13, no. 8: 1883. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13081883