Dietary Selenium Intake and Subclinical Hypothyroidism: A Cross-Sectional Analysis of the ELSA-Brasil Study

 , , and
, , and
Abstract
:1. Introduction
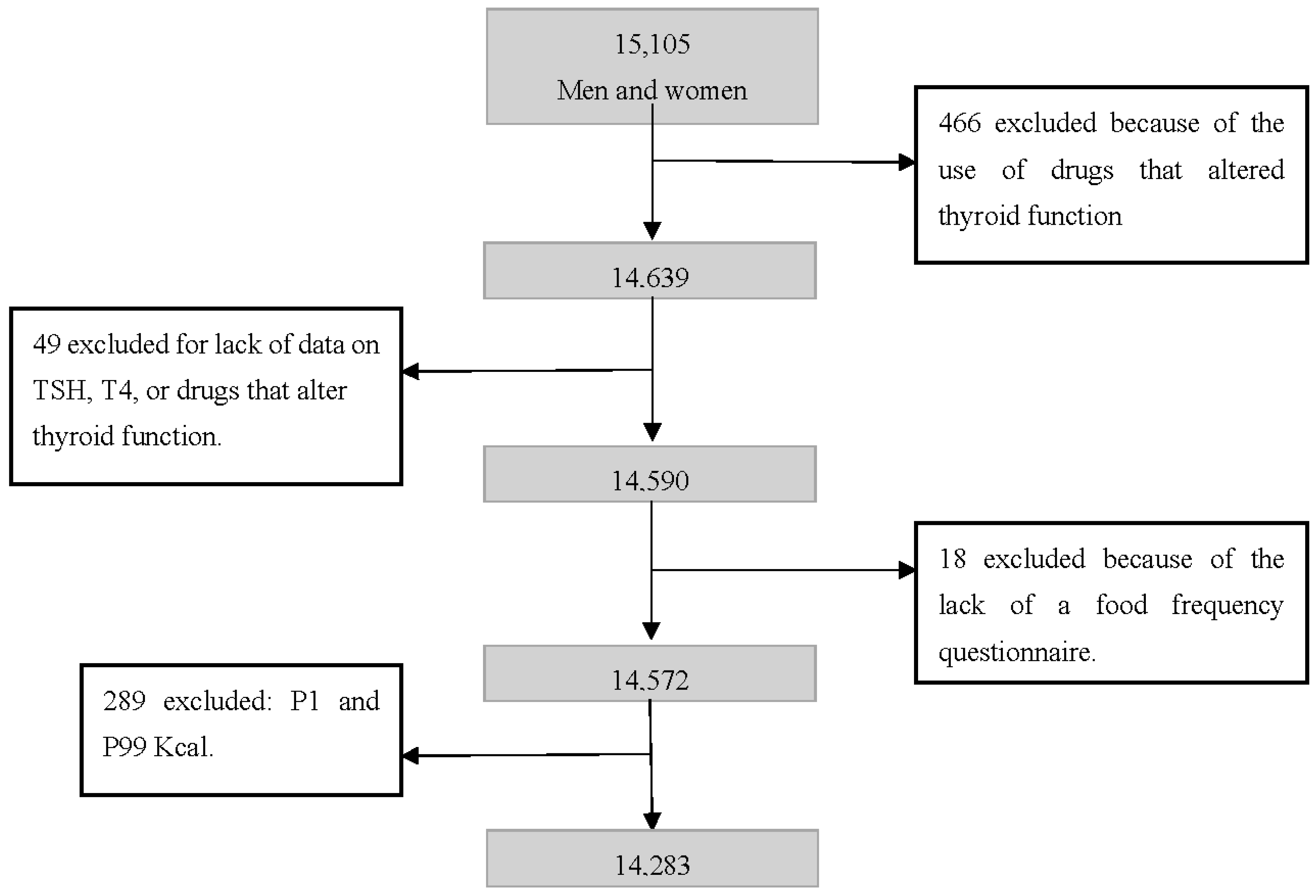
2. Materials and Methods
2.1. Ethical Aspects
2.2. Diet
2.3. Subclinical Hypothyroidism
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ichiki, T. Thyroid hormone and vascular remodeling. J. Atheroscler. Thromb. 2016, 23, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Bensenor, I.M.; Olmos, R.D.; Lotufo, P.A. Hypothyroidism in the elderly: Diagnosis and management. Clin. Interv. Aging 2012, 7, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Vinceti, M.; Filippini, T.; Del Giovane, C.; Dennert, G.; Zwahlen, M.; Brinkman, M.; Zeegers, M.P.; Horneber, M.; D’Amico, R.; Crespi, C.M. Selenium for preventing cancer. Cochrane Database Syst. Rev. 2018, 1, CD005195. [Google Scholar] [CrossRef] [PubMed]
- Fatourechi, V. Subclinical hypothyroidism: An update for primary care physicians. Mayo Clin. Proc. 2009, 84, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Bensenor, I.M.; Goulart, A.C.; Lotufo, P.A.; Menezes, P.R.; Scazufca, M. Prevalence of thyroid disorders among older people: Results from the São Paulo Ageing and Health Study. Cad. Saúde Pública 2011, 27, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Olmos, R.D.; Figueiredo, R.C.; Aquino, E.M.; Lotufo, P.A.; Bensenor, I.M. Gender, race and socioeconomic influence on diagnosis and treatment of thyroid disorders in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Braz. J. Med. Biol. Res. 2015, 48, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Sichieri, R.; Baima, J.; Marante, T.; de Vasconcellos, M.T.; Moura, A.S.; Vaisman, M. Low prevalence of hypothyroidism among black and Mulatto people in a population-based study of Brazilian women. Clin. Endocrinol. 2007, 66, 803–807. [Google Scholar] [CrossRef] [PubMed]
- Ventura, M.; Melo, M.; Carrilho, F. Selenium and thyroid disease: From pathophysiology to treatment. Int. J. Endocrinol. 2017, 2017, 1297658. [Google Scholar] [CrossRef] [PubMed]
- Schomburg, L. Selenium, selenoproteins and the thyroid gland: Interactions in health and disease. Nat. Rev. Endocrinol. 2011, 8, 160–171. [Google Scholar] [CrossRef] [PubMed]
- O’Kane, S.M.; Mulhern, M.S.; Pourshahidi, L.K.; Strain, J.J.; Yeates, A.J. Micronutrients, iodine status and concentrations of thyroid hormones: A systematic review. Nutr. Rev. 2018, 76, 418–431. [Google Scholar] [CrossRef] [PubMed]
- Behne, D.; Hilmert, H.; Scheid, S.; Gessner, H.; Elger, W. Evidence for specific selenium target tissues and new biologically important selenoproteins. Biochim. Biophys. Acta 1988, 966, 12–21. [Google Scholar] [CrossRef]
- Fairweather-Tait, S.J.; Bao, Y.; Broadley, M.R.; Collings, R.; Ford, D.; Hesketh, J.E.; Hurst, R. Selenium in human health and disease. Antioxid. Redox Signal. 2011, 14, 1337–1383. [Google Scholar] [CrossRef] [PubMed]
- Schomburg, L.; Riese, C.; Michaelis, M.; Griebert, E.; Klein, M.O.; Sapin, R.; Schweizer, U.; Köhrle, J. Synthesis and metabolism of thyroid hormones is preferentially maintained in selenium-deficient transgenic mice. Endocrinology 2006, 147, 1306–1313. [Google Scholar] [CrossRef] [PubMed]
- Parshukova, O.; Potolitsyna, N.; Shadrina, V.; Chernykh, A.; Bojko, E. Features of selenium metabolism in humans living under the conditions of North European Russia. Int. Arch. Occup. Environ. Health 2014, 87, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Rayman, M.P.; Lv, H.; Schomburg, L.; Gao, C.; Chen, P.; Zhuang, G.; Zhang, Z.; Peng, X.; Li, H.; et al. Low population selenium status is associated with increased prevalence of thyroid disease. J. Clin. Endocrinol. Metab. 2015, 100, 4037–4047. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, J.E. Selenium World Atlas; Selenium-Tellurium Development Association: Grimbergen, Belgium, 2002. [Google Scholar]
- Combs, G.F. Selenium in global food systems. Br. J. Nutr. 2001, 85, 517–547. [Google Scholar] [CrossRef] [PubMed]
- Donadio, J.L.; Guerra-Shinohara, E.M.; Rogero, M.M.; Cozzolino, S.M. Influence of Gender and SNPs in GPX1 Gene on Biomarkers of Selenium Status in Healthy Brazilians. Nutrients 2016, 8, 81. [Google Scholar] [CrossRef] [PubMed]
- Favaro, D.I.; Hui, M.L.; Cozzolino, S.M.; Maihara, V.A.; Armelin, M.J.; Vasconcellos, M.B.; Yuyama, L.K.; Boaventura, G.T.; Tramonte, V.L. Determination of various nutrients and toxic elements in different brazilian regional diets by neutron activation analysis. J. Trace Elem. Med. Biol. 1997, 11, 129–136. [Google Scholar] [CrossRef]
- Combs, G.F. Biomarkers of selenium status. Nutrients 2015, 7, 2209–2236. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, K.S.; Gomes, J.C.; Bellato, C.R.; Jordão, C.P. Concentrações de selênio em alimentos consumidos no Brasil. Rev. Panam. Salud Publica 2002, 11, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Kvicala, J.; Zamrazil, V. Effect of iodine and selenium upon thyroid function. Cent. Eur. J. Public Health 2003, 11, 107–113. [Google Scholar] [PubMed]
- Combs, G.F.; Midthune, D.N.; Patterson, K.Y.; Canfield, W.K.; Hill, A.D.; Levander, O.A.; Taylor, P.R.; Moler, J.E.; Patterson, B.H. Effects of selenomethionine supplementation on selenium status and thyroid hormone concentrations in healthy adults. Am. J. Clin. Nutr. 2009, 89, 1808–1814. [Google Scholar] [CrossRef] [PubMed]
- Thomson, C.D.; Campbell, J.M.; Miller, J.; Skeaff, S.A.; Livingstone, V. Selenium and iodine supplementation: Effect on thyroid function of older New Zealanders. Am. J. Clin. Nutr. 2009, 90, 1038–1046. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Reyes, R.; Mathieu, F.; Boelaert, M.; Begaux, F.; Suetens, C.; Rivera, M.T.; Nève, J.; Perlmutter, N.; Vanderpas, J. Selenium and iodine supplementation of rural Tibetan children affected by Kashin-Beck osteoarthropathy. Am. J. Clin. Nutr. 2003, 78, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Angstwurm, M.W.; Schopohl, J.; Gaertner, R. Selenium substitution has no direct effect on thyroid hormone metabolism in critically ill patients. Eur. J. Endocrinol. 2004, 151, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Aquino, E.M.L.; Vasconcellos-Silva, P.R.; Coeli, C.M.; Araújo, M.J.; Santos, S.M.; De Figueiredo, R.C.; Duncan, B.B. Aspectos éticos em estudos longitudinais: O caso do ELSA-Brasil. Rev. Saúde Pública 2013, 47, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Bensenor, I.M.; Griep, R.H.; Pinto, K.A.; de Faria, C.P.; Felisbino-Mendes, M.; Caetano, E.I.; Albuquerque, L.S.; Schmidt, M.I. Rotinas de organização de exames e entrevistas no centro de investigação ELSA-Brasil. Rev. Saúde Pública 2013, 47, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Chor, D.; Alves, M.G.M.; Giatti, L.; Cade, N.V.; Nunes, M.A.; Molina, M.C.B.; Bensenor, I.M.; Aquino, E.M.L.; Passos, V.; Santos, S.M.; et al. Questionário do ELSA-Brasil: Desafios na elaboração de instrumento multidimensional. Rev. Saúde Pública 2013, 47, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Molina, M.C.B.; Bensenor, I.M.; Cardoso, L.O.; Velazquez-Melendez, G.; Drehmer, M.; Pereira, T.S.S.; Faria, C.P.; Melere, C.; Manato, L.; Gomes, A.L.C.; et al. Reprodutibilidade e validade relativa do Questionário de Frequência Alimentar do ELSA-Brasil. Cad. Saúde Pública 2013, 29, 379–389. [Google Scholar] [CrossRef]
- Fedeli, L.G.; Vidigal, P.G.; Leite, C.M.; Castilhos, C.D.; Pimentel, R.A.; Maniero, V.C.; Mill, J.G.; Lotufo, P.A.; Pereira, A.C.; Bensenor, I.M. Logistics of collection and transportation of biological samples and the organization of the centrallaboratory in the ELSA-Brasil. Rev. Saude Publica 2013, 47, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Willet, W. Nutritional Epidemiology; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation; WHO Technical Report Series 894; World Health Organization: Geneva, Switzerland, 2000; Available online: http://www.who.int/iris/handle/10665/42330 (accessed on 10 April 2018).
- Mezzomo, T.R.; Nadal, J. Efeito dos nutrientes e substâncias alimentares na função tireoidiana e no hipotireoidismo. Demetra 2016, 11, 427–443. [Google Scholar] [CrossRef]
- McLean, R.M. Measuring population sodium intake: A review of methods. Nutrients 2014, 6, 4651–4662. [Google Scholar] [CrossRef] [PubMed]
- Chanoine, J.P.; Safran, M.; Farwell, A.P.; Tranter, P.; Ekenbarger, D.M.; Dubord, S.; Alex, S.; Arthur, J.R.; Beckett, G.J.; Braverman, L.E.; et al. Selenium deficiency and type II 5′-deiodinase regulation in the euthyroid and hypothyroid rat: Evidence of a direct effect of thyroxine. Endocrinology 1992, 131, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Kralik, A.; Eder, K.; Kirchgessner, M. Influence of zinc and selenium deficiency on parameters relating to thyroid hormone metabolism. Horm. Metab. Res. 1996, 28, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Beckett, G.J.; MacDougall, D.A.; Nicol, F.; Arthur, J.R. Inhibition of type I and type II iodothyronine deiodinase activity in rat liver, kidney and brain produced by selenium deficiency. Biochem. J. 1989, 259, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Köhrle, J.; Jakob, F.; Contempre, B.; Dumont, J.E. Selenium, the thyroid and the endocrine system. Endocr. Rev. 2005, 26, 944–984. [Google Scholar] [CrossRef] [PubMed]
- Thomson, C.D.; McLachlan, S.K.; Grant, A.M.; Peterson, E.; Lillico, A.J. The effect of selenium on thyroid status in a population with marginal selenium and iodine status. Br. J. Nutr. 2005, 94, 962–968. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, J.; Kahana, M.J. Neural representations of individual stimuli in humans revealed by gamma-band ECoG activity. J. Neurosci. 2009, 29, 10203–10214. [Google Scholar] [CrossRef] [PubMed]
- Van Zuuren, E.J.; Albusta, A.Y.; Fedorowicz, Z.; Carter, B.; Pijl, H. Selenium supplementation for Hashimoto’s thyroiditis. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed]
- Eskes, S.A.; Endert, E.; Fliers, E.; Birnie, E.; Hollenbach, B.; Schomburg, L.; Köhrle, J.; Wiersinga, W.M. Selenite supplementation in euthyroid subjects with thyroid peroxidase antibodies. Clin. Endocrinol. 2014, 80, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Kahaly, G.J.; Riedl, M.; König, J.; Diana, T.; Schomburg, L. Double-Blind, Placebo-Controlled, Randomized Trial of Selenium in Graves Hyperthyroidism. J. Clin. Endocrinol. Metab. 2017, 102, 4333–4341. [Google Scholar] [CrossRef] [PubMed]
- Winther, K.H.; Bonnema, S.J.; Cold, F.; Debrabant, B.; Nybo, M.; Cold, S.; Hegedus, L. Does selenium supplementation affect thyroid function? Results from a randomized, controlled, double-blinded trial in a Danish population. Eur. J. Endocrinol. 2015, 172, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.; Pop, V.J.; Bath, S.C.; Vader, H.L.; Redman, C.W.; Rayman, M.P. Effect of low-dose selenium on thyroid autoimmunity and thyroid function in UK pregnant women with mild-to-moderate iodine deficiency. Eur. J. Nutr. 2016, 55, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Contempre, B.; Dumont, J.E.; Ngo, B.; Thilly, C.H.; Diplock, A.T.; Vanderpas, J. Effect of selenium supplementation in hypothyroid subjects of an iodine and selenium deficient area: The possible danger of indiscriminate supplementation of iodine-deficient subjects with selenium. J. Clin. Endocrinol. Metab. 1991, 73, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P.; Thompson, A.J.; Bekaert, B.; Catterick, J.; Galassino, R.; Hall, E.; Warren-Perry, M.; Beckett, G.J. Randomized controlled trial of the effect of selenium supplementation on thyroid function in the elderly in the United Kingdom. Am. J. Clin. Nutr. 2008, 87, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, W.C.; Keim, N.L.; Diane Richter, B.; Gustafson, M.B.; Gale, B.; Mackey, B.R.; Bonnel, E.L. High-selenium yeast supplementation in free-living North American men: No effect on thyroid hormone metabolism or body composition. J. Trace Elem. Med. Biol. 2008, 22, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Pirola, I.; Gandossi, E.; Agosti, B.; Delbarba, A.; Cappelli, C. Selenium supplementation could restore euthyroidism in subclinical hypothyroid patients with autoimmune thyroiditis. Endokrynol. Pol. 2016, 67, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Negro, R.; Attanasio, R.; Grimaldi, F.; Morcocci, C.; Guglielmi, R.; Papine, E. A 2016 Italian survey about the clinical use of selenium in thyroid disease. Eur. Thyroid J. 2016, 5, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium and Carotenoids; National Academy Press: Washington, DC, USA, 2000; Available online: http://books.nap.edu/catalog/9810.html (accessed on 16 April 2018).
- Thompson, F.E.; Kirkpatrick, S.I.; Subar, A.F.; Reedy, J.; Schap, T.E.; Wilson, M.M.; Krebs-Smith, S.M. The national cancer institute’s dietary assessment primer: A resource for diet research. J. Acad. Nutr. Diet. 2015, 115, 1986–1995. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total | Selenium Intake * | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| First Tertile (0–187 mg) | Second Tertile (188–232 mg) | Third Tertile (233–1087 mg) | p Value ** | ||||||
| N | % | N | % | N | % | N | % | ||
| Sex | <0.001 | ||||||||
| Male | 6518 | 45.6 | 2519 | 53.0 | 1979 | 41.6 | 2020 | 42.4 | |
| Female | 7765 | 54.4 | 2242 | 47.0 | 2782 | 58.4 | 2741 | 57.6 | |
| Self-declared race | <0.001 | ||||||||
| Caucasian | 7418 | 52.5 | 2045 | 43.4 | 2540 | 53.9 | 2833 | 60.3 | |
| Black and Mixed | 6204 | 43.9 | 203 | 53.1 | 190 | 42.3 | 111 | 36.4 | |
| Others | 497 | 3.6 | 161 | 3.5 | 179 | 3.8 | 157 | 3.3 | |
| Age | <0.001 | ||||||||
| 35–59 years | 11,271 | 78.9 | 3892 | 80.5 | 3831 | 80.5 | 3548 | 74.5 | |
| ≥60 years | 3012 | 21.1 | 869 | 18.6 | 930 | 19.5 | 1213 | 25.5 | |
| Per capita income | <0.001 | ||||||||
| First tertile (USD 14.85–520.51) | 5175 | 36.1 | 2498 | 52.7 | 1665 | 35.1 | 1012 | 21.3 | |
| Second tertile (USD 529.87–1059.74) | 4992 | 34.9 | 1476 | 31.1 | 1739 | 36.6 | 1707 | 36.0 | |
| Third tertile (USD 1115.32–4238.97) | 4135 | 29.0 | 768 | 16.2 | 1342 | 28.3 | 2025 | 42.7 | |
| Current smoking | <0.001 | ||||||||
| No | 12,446 | 87.1 | 3979 | 83.6 | 4182 | 87.9 | 4285 | 90.0 | |
| Yes | 1836 | 12.9 | 782 | 16.4 | 578 | 12.1 | 476 | 10.0 | |
| Current alcohol use | <0.001 | ||||||||
| No | 4302 | 30.1 | 1675 | 35.2 | 1434 | 30.1 | 1193 | 25.1 | |
| Yes | 9978 | 69.9 | 3085 | 64.8 | 3325 | 69.9 | 3568 | 74.9 | |
| Physical activity during leisure | <0.001 | ||||||||
| Low | 10,796 | 76.7 | 3865 | 82.6 | 3621 | 77.3 | 3310 | 70.3 | |
| Moderate | 1986 | 14.1 | 499 | 10.7 | 683 | 14.6 | 804 | 17.2 | |
| Vigorous | 1287 | 9.2 | 315 | 6.7 | 379 | 8.1 | 593 | 12.5 | |
| Change in diet | <0.001 | ||||||||
| No | 9903 | 69.4 | 3517 | 73.9 | 3247 | 68.3 | 3139 | 66.0 | |
| Yes | 4366 | 30.6 | 1243 | 26.1 | 1507 | 31.7 | 1616 | 34.0 | |
| Use of dietary supplements | <0.001 | ||||||||
| No | 10,887 | 77.3 | 3940 | 84.2 | 3639 | 77.5 | 3308 | 70.5 | |
| Regularly | 1823 | 12.9 | 391 | 8.3 | 579 | 12.3 | 853 | 18.0 | |
| Not regularly | 1381 | 9.8 | 353 | 7.5 | 480 | 10.2 | 548 | 11.5 | |
| Nutritional status | <0.001 | ||||||||
| Low weight | 129 | 0.9 | 57 | 1.2 | 34 | 0.7 | 38 | 0.8 | |
| Eutrophic | 5175 | 36.2 | 1672 | 35.1 | 1662 | 34.9 | 1841 | 38.7 | |
| Overweight | 5740 | 40.2 | 1898 | 39.9 | 1940 | 40.8 | 1902 | 40.0 | |
| Obese | 3234 | 22.7 | 1,32 | 23.8 | 1124 | 23.6 | 978 | 20.5 | |
| Hypertension | <0.001 | ||||||||
| No | 9930 | 69.5 | 3047 | 64.0 | 3120 | 65.5 | 3163 | 66.4 | |
| Yes | 4951 | 34.7 | 1714 | 36.0 | 1640 | 34.5 | 1597 | 33.6 | |
| Diabetes | <0.001 | ||||||||
| No | 11,558 | 80.9 | 3797 | 79.8 | 3886 | 81.6 | 3875 | 81.4 | |
| Yes | 2724 | 19.1 | 963 | 20.2 | 875 | 18.4 | 886 | 18.6 | |
| Dyslipidemia | <0.001 | ||||||||
| No | 6007 | 42.4 | 2225 | 47.0 | 1926 | 40.8 | 1856 | 39.4 | |
| Yes | 8169 | 57.6 | 2510 | 53.0 | 2799 | 59.2 | 2860 | 60.6 | |
| Thyroid function | <0.001 | ||||||||
| Subclinical hypothyroidism | 770 | 5.4 | 276 | 5.8 | 252 | 5.3 | 242 | 5.1 | |
| Clinical hypothyroidism | 1061 | 7.4 | 256 | 5.4 | 383 | 8.0 | 422 | 8.9 | |
| Euthyroid | 12,171 | 85.3 | 4146 | 87.1 | 4022 | 84.5 | 4003 | 84.1 | |
| Subclinical hyperthyroidism | 186 | 1.3 | 57 | 1.2 | 70 | 1.5 | 59 | 1.2 | |
| Clinical hyperthyroidism | 95 | 0.6 | 26 | 0.5 | 34 | 0.7 | 35 | 0.7 | |
| Total | Selenium Intake * | R *** | |||||||
|---|---|---|---|---|---|---|---|---|---|
| First Tertile (0–187 mg) | Second Tertile (188–232 mg) | Third Tertile (233–1087 mg) | p Value ** | ||||||
| N | N | % | N | % | N | % | |||
| Energy (average) | <0.001 | _ | |||||||
| First tertile (1900 kcal) | 4761 | 1049 | 22.0 | 2202 | 46.2 | 1510 | 31.7 | ||
| Second tertile (2735 kcal) | 4761 | 1599 | 33.6 | 1529 | 32.1 | 1633 | 34.3 | ||
| Third tertile (4166 kcal) | 4761 | 2113 | 44.4 | 1030 | 21.6 | 1618 | 34.0 | ||
| Zinc * (average) | <0.001 | 0.16 | |||||||
| First tertile (13 mg) | 4761 | 2562 | 53.8 | 1226 | 25.7 | 973 | 20.4 | ||
| Second tertile (16 mg) | 4761 | 1278 | 26.8 | 1833 | 38.5 | 1650 | 34.7 | ||
| Third tertile (21 mg) | 4761 | 921 | 19.3 | 1702 | 35.8 | 2138 | 44.9 | ||
| Vitamin A * (average) | <0.001 | 0.11 | |||||||
| First tertile (71 mg) | 4761 | 1887 | 39.6 | 1614 | 33.9 | 1260 | 26.5 | ||
| Second tertile (125 mg) | 4761 | 1443 | 30.3 | 1714 | 36.0 | 1604 | 33.7 | ||
| Third tertile (220 mg) | 4761 | 1431 | 30.1 | 1433 | 30.7 | 1897 | 40.6 | ||
| Total fat * (average) | <0.001 | 0.33 | |||||||
| First tertile (74 g) | 4761 | 2335 | 49.0 | 1418 | 29.8 | 1008 | 21.2 | ||
| Second tertile (93 g) | 4761 | 1399 | 29.4 | 1815 | 38.1 | 1547 | 31.6 | ||
| Third tertile (112 g) | 4761 | 1027 | 21.6 | 1528 | 32.1 | 2206 | 47.2 | ||
| Saturated fat * (average) | <0.001 | 0.13 | |||||||
| First tertile (22 g) | 4761 | 2107 | 44.3 | 1354 | 28.4 | 1300 | 27.8 | ||
| Second tertile (30 g) | 4761 | 1315 | 28.1 | 1825 | 39.1 | 1621 | 34.7 | ||
| Third tertile (41 g) | 4761 | 1339 | 28.7 | 1582 | 33.9 | 1840 | 39.0 | ||
| Urinary sodium (average) | <0.001 | −0.08 | |||||||
| First tertile (6 g/day) | 4665 | 1345 | 28.8 | 1537 | 33.0 | 1773 | 38.1 | ||
| Second tertile (10 g/day) | 4667 | 1528 | 32.8 | 1563 | 33.6 | 1576 | 33.9 | ||
| Third tertile (19 g/day) | 4642 | 1782 | 38.4 | 1557 | 33.4 | 1303 | 28.0 | ||
| Model 1 a | Model 2 b | Model 3 c | Model 4 d | Model 5 e | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | ||||||
| Selenium ** | |||||||||||||||
| First tertile (0–187 mg) | 1 | _ | _ | 1 | _ | _ | 1 | _ | _ | 1 | _ | _ | 1 | _ | _ |
| Second tertile (188–232 mg) | 0.89 | 0.74 | 1.08 | 0.85 | 0.71 | 1.03 | 0.81 | 0.67 | 0.98 | 0.80 | 0.66 | 0.97 | 0.79 | 0.65 | 0.96 |
| Third tertile (233–1087 mg) | 0.90 | 0.75 | 1.08 | 0.86 | 0.70 | 1.05 | 0.74 | 0.60 | 0.92 | 0.73 | 0.59 | 0.91 | 0.72 | 0.58 | 0.90 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrade, G.R.G.; Gorgulho, B.; Lotufo, P.A.; Bensenor, I.M.; Marchioni, D.M. Dietary Selenium Intake and Subclinical Hypothyroidism: A Cross-Sectional Analysis of the ELSA-Brasil Study. Nutrients 2018, 10, 693. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10060693
Andrade GRG, Gorgulho B, Lotufo PA, Bensenor IM, Marchioni DM. Dietary Selenium Intake and Subclinical Hypothyroidism: A Cross-Sectional Analysis of the ELSA-Brasil Study. Nutrients. 2018; 10(6):693. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10060693
Chicago/Turabian StyleAndrade, Gustavo R. G., Bartira Gorgulho, Paulo A. Lotufo, Isabela M. Bensenor, and Dirce M. Marchioni. 2018. "Dietary Selenium Intake and Subclinical Hypothyroidism: A Cross-Sectional Analysis of the ELSA-Brasil Study" Nutrients 10, no. 6: 693. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10060693