What Is Known About the Nutritional Intake of Women during Pregnancy Following Bariatric Surgery? A Scoping Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
- identifying the research question
- identifying relevant studies
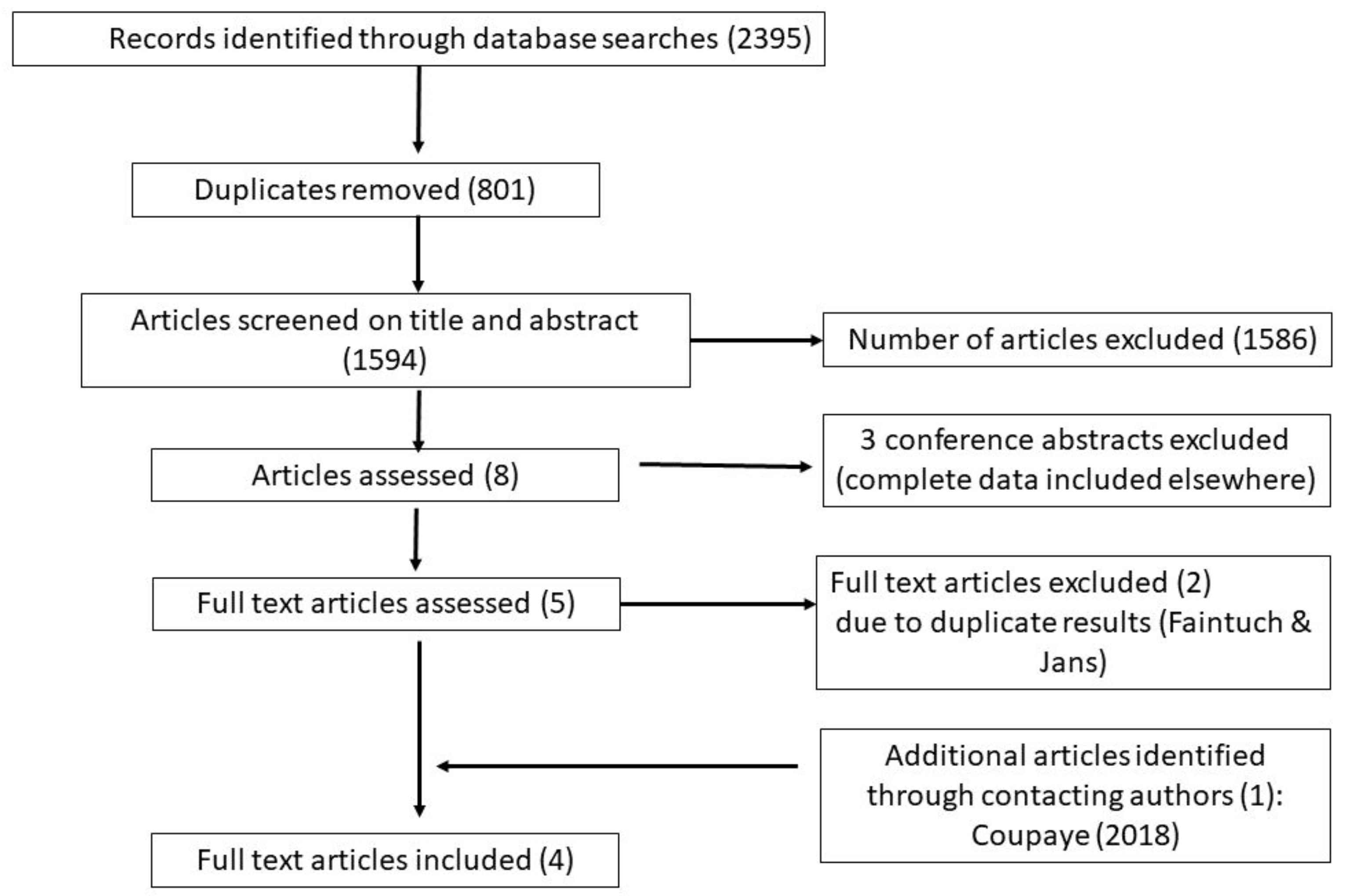
- study selection
- charting the data
- collating, summarising and reporting the results.
2.2. Identifying the Research Question
2.3. Search Strategy
2.4. Charting and Summarising the Data
3. Results
3.1. Study Characteristics
3.2. Dietary Assessment Methodology of Included Studies
3.3. Macronutrient and Micronutrient Intakes
3.4. Group Comparisons
3.5. Links between Nutritional Intake and Other Outcomes
4. Discussion
Strengths and Limitations of Methodology
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Stephenson, J.; Heslehurst, N.; Hall, J.; Schoenaker, D.A.J.M.; Hutchinson, J.; Cade, J.E.; Poston, L.; Barrett, G.; Crozier, S.R.; Barker, M.; et al. Before the beginning: Nutrition and lifestyle in the preconception period and its importance for future health. Lancet 2018, 391, 1830–1841. [Google Scholar] [CrossRef]
- Brewer, C.J.; Balen, A.H. The adverse effects of obesity on conception and implantation. Reproduction 2010, 140, 347–364. [Google Scholar] [CrossRef] [Green Version]
- Marchi, J.; Berg, M.; Dencker, A.; Olander, E.K.; Begley, C. Risks associated with obesity in pregnancy, for the mother and baby: A systematic review of reviews. Obes. Rev. 2015, 16, 621–638. [Google Scholar] [CrossRef]
- Santos, S.; Voerman, E.; Amiano, P.; Barros, H.; Beilin, L.J.; Bergström, A.; Charles, M.A.; Chatzi, L.; Chevrier, C.; Chrousos, G.P.; et al. Impact of maternal body mass index and gestational weight gain on pregnancy complications: An individual participant data meta-analysis of European, North American and Australian cohorts. BJOG 2019, 126, 984–995. [Google Scholar] [CrossRef]
- Devlieger, R.; Benhalima, K.; Damm, P.; Van Assche, A.; Mathieu, C.; Mahmood, T.; Dunne, F.; Bogaerts, A. Maternal obesity in Europe: Where do we stand and how to move forward? A scientific paper commissioned by the European Board and College of Obstetrics and Gynaecology (EBCOG). Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 201, 203–208. [Google Scholar] [CrossRef]
- Hales, C.M.; Fryar, C.D.; Carroll, M.D.; Freedman, D.S.; Ogden, C.L. Trends in Obesity and Severe Obesity Prevalence in US Youth and Adults by Sex and Age, 2007–2008 to 2015–2016. JAMA 2018, 319, 1723–1725. [Google Scholar] [CrossRef]
- Sullivan, E.A.; Dickinson, J.E.; Vaughan, G.A.; Peek, M.J.; Ellwood, D.; Caroline, S.E.; Knight, M.; Mclintock, C.; Wang, A.; Pollock, W.; et al. Maternal super-obesity and perinatal outcomes in Australia: A national population-based cohort study. BMC Pregnancy Childbirth 2015, 15, 322. [Google Scholar] [CrossRef]
- OOnubi, J.; Marais, D.; Aucott, L.; Okonofua, F.; Poobalan, A.S. Maternal obesity in Africa: A systematic review and meta-analysis. J. Public Health (Oxf.) 2016, 38, e218–e231. [Google Scholar] [CrossRef]
- Sjostrom, L.; Lindroos, A.K.; Peltonen, M.; Torgerson, J.; Bouchard, C.; Carlsson, B.; Dahlgren, S.; Larsson, B.; Narbro, K.; Sjöström, C.D.; et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N. Engl. J. Med. 2004, 351, 2683–2693. [Google Scholar] [CrossRef]
- Colquitt, J.L.; Pickett, K.; Loveman, E.; Frampton, G.K. Surgery for weight loss in adults. Cochrane Database Syst. Rev. 2014, CD003641. [Google Scholar] [CrossRef]
- Johnson, E.E.; Simpson, A.N.; Harvey, J.B.; Lockett, M.A.; Byrne, K.T.; Simpson, K.N. Trends in bariatric surgery, 2002–2012: Do changes parallel the obesity trend? Surg. Obes. Relat. Dis. 2016, 12, 398–404. [Google Scholar] [CrossRef]
- Fuchs, H.F.; Broderick, R.C.; Harnsberger, C.R.; Chang, D.C.; Sandler, B.J.; Jacobsen, G.R.; Horgan, S. Benefits of bariatric surgery do not reach obese men. J. Laparoendosc Adv. Surg. Tech. A 2015, 25, 196–201. [Google Scholar] [CrossRef]
- NBSR. The United Kingdom National Bariatric Surgery Registry. Second Registry Report. National Bariatric Surgery Registry 2014. Available online: http://www.bomss.org.uk/wpcontent/uploads/2014/04/Extract_from_the_NBSR_2014_report.pdf (accessed on 16 April 2019).
- Edison, E.; Whyte, M.; van Vlymen, J.; Jones, S.; Gatenby, P.; de Lusignan, S.; Shawe, J. Bariatric Surgery in Obese Women of Reproductive Age Improves Conditions That Underlie Fertility and Pregnancy Outcomes: Retrospective Cohort Study of UK National Bariatric Surgery Registry (NBSR). Obes. Surg. 2016, 26, 283–2842. [Google Scholar] [CrossRef]
- Gosman, G.G.; King, W.C.; Schrope, B.; Steffen, K.J.; Strain, G.W.; Courcoulas, A.P.; Flum, D.R.; Pender, J.R.; Simhan, H.N. Reproductive health of women electing bariatric surgery. Fertil. Steril. 2010, 94, 1426–1431. [Google Scholar] [CrossRef] [Green Version]
- Boerlage, T.C.C.; Westerink, F.; van de Laar, A.; Hutten, B.A.; Brandjes, D.P.M.; Gerdes, V.E.A. Gastrointestinal symptoms before and after laparoscopic Roux-en-Y gastric bypass: A longitudinal assessment. Surg. Obes. Relat. Dis. 2019, 15, 871–877. [Google Scholar] [CrossRef]
- Mala, T.; Hogestol, I. Abdominal Pain After Roux-En-Y Gastric Bypass for Morbid Obesity. Scand. J. Surg. 2018, 107, 277–284. [Google Scholar] [CrossRef] [Green Version]
- Shoar, S.; Naderan, M.; Shoar, N.; Modukuru, V.R.; Mahmoodzadeh, H. Alteration Pattern of Taste Perception After Bariatric Surgery: A Systematic Review of Four Taste Domains. Obes. Surg. 2019, 29, 1542–1550. [Google Scholar] [CrossRef]
- Nicoletti, C.F.; de Oliveira, B.A.; Barbin, R.; Marchini, J.S.; Junior, W.S.; Nonino, C.B. Red meat intolerance in patients submitted to gastric bypass: A 4-year follow-up study. Surg. Obes. Relat. Dis. 2015, 11, 842–846. [Google Scholar] [CrossRef]
- Opozda, M.; Chur-Hansen, A.; Wittert, G. Changes in problematic and disordered eating after gastric bypass, adjustable gastric banding and vertical sleeve gastrectomy: A systematic review of pre-post studies. Obes. Rev. 2016, 17, 770–792. [Google Scholar] [CrossRef]
- O’Kane, M.; Parretti, H.M.; Hughes, C.A.; Sharma, M.; Woodcock, S.; Puplampu, T.; Blakemore, A.I.; Clare, K.; MacMillan, I.; Joyce, J.; et al. Guidelines for the follow-up of patients undergoing bariatric surgery. Clin. Obes. 2016, 6, 210–224. [Google Scholar] [CrossRef]
- Einarson, T.R.; Piwko, C.; Koren, G. Quantifying the global rates of nausea and vomiting of pregnancy: A meta analysis. J. Popul. Ther. Clin. Pharmacol. 2013, 20, e171–e183. [Google Scholar]
- Crozier, S.R.; Inskip, H.M.; Godfrey, K.M.; Cooper, C.; Robinson, S.M. Nausea and vomiting in early pregnancy: Effects on food intake and diet quality. Matern. Child. Nutr. 2017, 13, e12389. [Google Scholar] [CrossRef]
- Busetto, L.; Dicker, D.; Azran, C.; Batterham, R.L.; Farpour-Lambert, N.; Fried, M.; Hjelmesæth, J.; Kinzl, J.; Leitner, D.R.; Makaronidis, J.M.; et al. Obesity Management Task Force of the European Association for the Study of Obesity Released Practical Recommendations for the Post-Bariatric Surgery Medical Management. Obes. Surg. 2018, 28, 2117–2121. [Google Scholar] [CrossRef]
- Harreiter, J.; Schindler, K.; Bancher-Todesca, D.; Gobl, C.; Langer, F.; Prager, G.; Gessel, A.; Leutner, M.; Ludvik, B.; Luger, A.; et al. Management of Pregnant Women after Bariatric Surgery. J. Obes. 2018, 2018, 4587064. [Google Scholar] [CrossRef]
- SACN. Update on Folic Acid. Scientific Advisory Committee on Nutrition London 2017. Available online: https://www.gov.uk/government/publications/folic-acid-updated-sacn-recommendations (accessed on 16 April 2019).
- NICE. Maternal and child nutrition NICE Public Health Guidance (PH11). National Institute for Clinical Excellence 2008. Available online: https://www.nice.org.uk/guidance/ph11 (accessed on 16 April 2019).
- Yi, X.Y.; Li, Q.F.; Zhang, J.; Wang, Z.H. A meta-analysis of maternal and fetal outcomes of pregnancy after bariatric surgery. Int. J. Gynaecol. Obstet. 2015, 130, 3–9. [Google Scholar] [CrossRef]
- Johansson, K.; Sven Cnattingius, M.D.; Ingmar, N.; Nathalie, R.; Ylva Trolle, L.; Fredrik, G.; Olof, S.; Martin, N. Outcomes of pregnancy after bariatric surgery. N. Engl. J. Med. 2015, 372, 814–824. [Google Scholar] [CrossRef]
- Maggard, M.A.; Yermilov, I.; Li, Z.; Maglione, M.; Newberry, S.; Suttorp, M.; Hilton, L.; Santry, H.P.; Morton, J.M.; Livingston, E.H.; et al. Pregnancy and fertility following bariatric surgery: A systematic review. JAMA 2008, 300, 2286–2296. [Google Scholar] [CrossRef]
- Adams, T.D.; Hammoud, A.O.; Davidson, L.E.; Laferrère, B.; Fraser, A.; Stanford, J.B.; Hashibe, M.; Greenwood, J.L.; Kim, J.; Taylor, D. Maternal and neonatal outcomes for pregnancies before and after gastric bypass surgery. Int. J. Obes. (Lond.) 2015, 39, 686–694. [Google Scholar] [CrossRef] [Green Version]
- Galazis, N.; Docheva, N.; Simillis, C.; Nicolaides, K.H. Maternal and neonatal outcomes in women undergoing bariatric surgery: A systematic review and meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 181, 45–53. [Google Scholar] [CrossRef]
- Jans, G.; Matthys, C.; Bogaerts, A.; Lannoo, M.; Verhaeghe, J.; Van der Schueren, B.; Devlieger, R. Maternal micronutrient deficiencies and related adverse neonatal outcomes after bariatric surgery: A systematic review. Adv. Nutr. 2015, 6, 420–429. [Google Scholar] [CrossRef]
- Rottenstreich, A.; Elazary, R.; Goldenshluger, A.; Pikarsky, A.J.; Elchalal, U.; Ben-Porat, T. Maternal nutritional status and related pregnancy outcomes following bariatric surgery: A systematic review. Surg. Obes. Relat. Dis. 2019, 15, 324–332. [Google Scholar] [CrossRef]
- JBI. The Joanna Briggs Institute Reviewers’ Manual 2015 Methodology for JBI Scoping Reviews. The Joanna Briggs Institute 2015. Available online: http://joannabriggs.org/assets/docs/sumari/Reviewers-Manual_Methodology-for-JBI-Scoping-Reviews_2015_v2.pdf (accessed on 9 April 2019).
- Arskey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–23. [Google Scholar]
- Jans, G.; Mattheus, A.; Galjaard, S.; Bogaerts, A.; Vansant, G.; Devlieger, R. Systematic follow-up of pregnancies after bariatric surgery: A prospective controlled study. In 60th Annual Scientific Meeting of the Society for Gynecologic Investigation; Reproductive Sciences: Weston, FL, USA, 2013; Volume 20, p. 329A. [Google Scholar]
- Jans, G.; Guelinckx, I.; Matthys, C.; van der Schueren, B.; Vansant, G.; Devlieger, R. Close monitoring and coaching of pregnancies after bariatric surgery results in better outcomes: A prospective, controlled study. Presented at the 61st Annual Scientific Meeting of the Society for Gynecologic Investigation, Florence, Italy, 21–23 March 2014. [Google Scholar]
- Guelinckx, I.; Vansant, G.; Devlieger, R. A prospective study analyzing the fat-soluble vitamins and dietary habits during 1st pregnancy trimester of women with bariatric surgery. In 58th Annual Scientific Meeting of the Society for Gynecologic Investigation; Reproductive Sciences: Weston, FL, USA, 2011; p. 165A. [Google Scholar]
- Faintuch, J.; Dias, M.C.; de Souza Fazio, E.; de Oliveira, F.C.; Nomura, R.M.; Zugaib, M.; Cecconello, I. Pregnancy nutritional indices and birth weight after Roux-en-Y gastric bypass. Obes. Surg. 2009, 19, 583–589. [Google Scholar] [CrossRef]
- Jans, G.; Devlieger, R.; De Preter, V.; Ameye, L.; Roelens, K.; Lannoo, M.; Van der Schueren, B.; Verhaeghe, J.; Matthys, C. Bariatric Surgery Does Not Appear to Affect Women’s Breast-Milk Composition. J. Nutr. 2018, 148, 1096–1102. [Google Scholar] [CrossRef]
- Dias, M.C.; Ede, S.F.; de Oliveira, F.C.; Nomura, R.M.; Faintuch, J.; Zugaib, M. Body weight changes and outcome of pregnancy after gastroplasty for morbid obesity. Clin. Nutr. 2009, 28, 169–172. [Google Scholar] [CrossRef]
- Jans, G.; Matthys, C.; Bogaerts, A.; Ameye, L.; Delaere, F.; Roelens, K.; Loccufier, A.; Logghe, H.; De Becker, B.; Verhaeghe, J.; et al. Depression and Anxiety: Lack of Associations with an Inadequate Diet in a Sample of Pregnant Women with a History of Bariatric Surgery-a Multicenter Prospective Controlled Cohort Study. Obes. Surg. 2018, 28, 1629–1635. [Google Scholar] [CrossRef]
- Coupaye, M.; Legardeur, H.; Sami, O.; Calabrese, D.; Mandelbrot, L.; Ledoux, S. Impact of Roux-en-Y gastric bypass and sleeve gastrectomy on fetal growth and relationship with maternal nutritional status. Surg. Obes. Relat. Dis. 2018, 14, 1488–1494. [Google Scholar] [CrossRef]
- Guelinckx, I.; Devlieger, R.; Donceel, P.; Bel, S.; Pauwels, S.; Bogaerts, A.; Thijs, I.; Schurmans, K.; Deschilder, P.; Vansant, G. Lifestyle after bariatric surgery: A multicenter, prospective cohort study in pregnant women. Obes. Surg. 2012, 22, 1456–1464. [Google Scholar] [CrossRef]
- Nutritional Recommendations for the Belgian Population; Scientific Advisory report on Public Health Policy HGR: Brussels, Belgium, 2016; Nr 9285.
- Mechanick, J.I.; Youdim, A.; Jones, D.B.; Garvey, W.T.; Hurley, D.L.; McMahon, M.; Heinber, L.J.; Kushner, R.; Adam, T.D.; Shikora, S.; et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient--2013 update: Cosponsored by American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery. Obesity (Silver Spring) 2013, 21, S1–S27. [Google Scholar]
- NICE. Clinical Guideline 189—Obesity: Identification, Assessment and Management of Overweight and Obesity in Children, Young People and Adults. National Institute for Health and Care Excellence, London 2014. Available online: https://www.nice.org.uk/guidance/cg189 (accessed on 16 April 2019).
- Shawe, J. Pregnancy after bariatric surgery: European consensus guidelines. Obes. Rev. 2019, in press. [Google Scholar] [CrossRef]
- ACOG practice bulletin no. 105: Bariatric surgery and pregnancy. Obstet. Gynecol. 2009, 113, 1405–1413.
- RCOG. Bariatric Surgery in Improving Reproductive Health, The Role of (Scientific Impact Paper No. 17). Royal College of Obstetricians and Gynaecologists 2015. Available online: https://www.rcog.org.uk/en/guidelines-research-services/guidelines/sip17/ (accessed on 16 April 2019).
- Mengesha, B.; Griffin, L.; Nagle, A.; Kiley, J. Assessment of contraceptive needs in women undergoing bariatric surgery. Contraception 2016, 94, 74–77. [Google Scholar] [CrossRef]
- O’Kane, P.J.; Aasheim, M.; Barth, E.; Batterham, J.; Welbourn, R.R. British Obesity and Metabolic Surgery Society (BOMSS). Guidelines on Peri-Operative and Postoperative Biochemical Monitoring and Micronutrient Replacement for Patients Undergoing Bariatric Surgery; BOMSS: London, UK, 2014. [Google Scholar]
- Hillier, S.E.; Olander, E.K. Women’s dietary changes before and during pregnancy: A systematic review. Midwifery 2017, 49, 19–31. [Google Scholar] [CrossRef]
- Hill, A.J.; Cairnduff, V.; McCance, D.R. Nutritional and clinical associations of food cravings in pregnancy. J. Hum. Nutr. Diet. 2016, 29, 281–289. [Google Scholar] [CrossRef]
- Wilson, R.L.; Grieger, J.A.; Bianco-Miotto, T.; Roberts, C.T. Association between Maternal Zinc Status, Dietary Zinc Intake and Pregnancy Complications: A Systematic Review. Nutrients 2016, 8, 10. [Google Scholar] [CrossRef]
- Bath, S.C. The effect of iodine deficiency during pregnancy on child development. Proc. Nutr. Soc. 2019, 78, 150–160. [Google Scholar] [CrossRef]
- Middleton, P.; Gomersall, J.C.; Gould, J.F.; Shepherd, E.; Olsen, S.F.; Makrides, M. Omega-3 fatty acid addition during pregnancy. Cochrane Database Syst. Rev. 2018, 11, Cd003402. [Google Scholar] [CrossRef]
- Faria, S.L.; Faria, O.P.; de Gouvea, H.R.; Amato, A.A. Supplementation Adherence and Outcomes Among Pregnant Women After Bariatric Surgery. Obes. Surg. 2019, 29, 178–182. [Google Scholar] [CrossRef]
- Jans, G.; Matthys, C.; Bel, S.; Ameye, L.; Lannoo, M.; Van der Schueren, B.; Dillemans, B.; Lemmens, L.; Saey, J.P.; van Nieuwenhove, Y.; et al. AURORA: Bariatric surgery registration in women of reproductive age—A multicenter prospective cohort study. BMC Pregnancy Childbirth 2016, 16, 195. [Google Scholar] [CrossRef]
- Cade, J.E.; Warthon-Medina, M.; Albar, S.; Alwan, N.A.; Ness, A.; Roe, M.; Wark, P.A.; Greathead, K.; Burley, V.J.; Finglas, P.; et al. DIET@NET: Best Practice Guidelines for dietary assessment in health research. BMC Med. 2017, 15, 202. [Google Scholar] [CrossRef]
- Dodsworth, A.; Warren-Forward, H.; Baines, S. A systematic review of dietary intake after laparoscopic adjustable gastric banding. J. Hum. Nutr. Diet. 2011, 24, 327–341. [Google Scholar] [CrossRef]
- Janmohammadi, P.; Sajadi, F.; Alizadeh, S.; Daneshzad, E. Comparison of Energy and Food Intake Between Gastric Bypass and Sleeve Gastrectomy: A Meta-analysis and Systematic Review. Obes. Surg. 2019, 29, 1040–1048. [Google Scholar] [CrossRef]
- Peters, M.D.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based. Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Authors, Year | Study Population | Location | Participants (N) | Mean/Median Age * (Years) | Pre-Pregnancy BMI (kg/m2) | Time Interval Surgery to Conception (Months) | Method |
|---|---|---|---|---|---|---|---|
| Dias et al. (2009) [42] | Women who conceived between 0–5 years after having RYGB surgery | Brazil | 14 | 31.8 ± 6.5 | Not stated | 24.2 ± 21.6 | Retrospective medical note review |
| Guelinckx et al. (2012) [45] | Pregnant women with a history of bariatric surgery | Belgium | 49: 18 LAGB 31 RYGB | 31 (25–36) (LAGB group) 30 (18–38) (RYGB group) | 31 (22–44) (LAGB group) 25 (22–39) (RYGB group) | 44 (4–108) (LAGB group) 22 (2–96) (RYGB group) | Prospective study: 7 day food diary collected in first and second trimester (weeks 7–12 and week 20) |
| Jans et al. (2018) [43] | Pregnant women with a history of bariatric surgery | Belgium | 54: 45 RYGB 2 SG 2 LAGB 2 Scoparino procedure 3 not specified | 29.4 ± 4.3 | 28.1 ± 5.1 | 45.6 ± 29.9 | Prospective study: 3 day food record measured in first and third trimester (15 weeks and 32 weeks) |
| Coupaye et al. [44] (2018) | Pregnant women who had bariatric surgery and at least 1 nutritional evaluation | France | 85 with dietary data: 55 RYGB 30 SG | 33.4 ± 4.7 (RYGB group) 31.1 ± 4.8 (SG group) | 31.2 ± 5.0 (RYGB group) 31.6 ± 6.8 (SG group) | 31 ± 22 (RYGB group) 24 ± 18 (SG group) | Prospective: 4 day food diary |
| Authors | Control Group | Method of Dietary Monitoring | Dietary Outcome Measures | Results | Conclusions/Recommendations |
|---|---|---|---|---|---|
| Dias et al. (2009) [42] | No | Unclear–“energy and protein ingestion transcribed from patient’s chart” (Trimester 2 and 3). |
| Trimester 2 mean daily intake: Energy: 1789 ± 659 kcal Protein: 61.7 ± 19.8 g Trimester 3 mean daily intake: Energy: 1881 ± 835 kcal Protein: 62.8 ± 19.2 g |
|
| Guelinckx et al. (2012) [45] | No | 7 day food diary (Trimester 1 and 2) |
| Trimester 1 mean daily intake LAGB participants: Energy: 1971 ± 430 kcal Protein as % energy: 15.1 ± 1.5 Total fat as % energy: 35.3 ± 4.7 Saturated fat as % energy: 13.0 ± 2.6 Carbohydrate as % energy: 49.8 ± 5.4 Fibre: 19.5 ± 5.4 g Calcium: 822 ± 273 mg Iron: 11 ± 2 mg RYGB participants: Energy: 1786 ± 283 kcal Protein as % energy: 15.8 ± 2.1 Total fat as % energy: 35.9 ± 3.3 Saturated fat as % energy: 14.2 ± 2.3 Carbohydrate as % energy: 48.5 ± 3.9 Fibre: 17.5 ± 5.3 g Calcium: 702 ± 228 mg Iron: 9 ± 2 mg Trimester 2 mean daily intake LAGB participants: Energy: 1978 ± 472 kcal Protein as % energy: 15.5 ± 2.2 Carbohydrate as % energy: 49.4 ± 4.4 Total fat as % energy: 14.2 ± 2.3 Saturated fat as % energy: 13.6 ± 2.4 Fibre: 17.7 ± 5.8 g Calcium: 806 ± 384 mg Iron: 10 ± 2 mg RYGB participants: Energy: 1895 ± 542 kcal Protein as % energy: 15.1 ± 2.4 Total fat as % energy: 35.1 ± 4.0 Saturated fat as % energy: 14.2 ± 1.9 Carbohydrate as % energy: 49.9 ± 4.4 Fibre: 18.2 ± 3.5 g Calcium: 764 ± 370 mg Iron: 10 ± 30 mg |
|
| Jans et al. (2018) [43] | Yes 25 pregnant women with obesity | 3 day food record (Trimester 1 and 3) |
| Trimester 1 mean daily intake: Energy: 1452.46 ± 415.99 kcal Total fat: 56.21 ± 19.65 g Saturated fat: 23.39 ± 8.81 g MUFA: 17.73 ± 7.00 g PUFA: 8.80 ± 3.75 g n3 fatty acids: 0.78 (0.12–2.06) * g n6 fatty acids: 5.42 (1.38–15.25) * g Folate: 177.25 (42.01–419.62) * mcg Vitamin B12: 2.94 (0.59–8.54) * mcg Trimester 3 mean daily intake: Energy: 1514.47 ± 503.69 kcal Total fat: 56.8 ± 20.50 g Saturated fat: 24.25 ± 9.33 g MUFA: 17.86 ± 7.39 g PUFA: 8.35 (2.86–24.34) * g n3 fatty acids: 0.64 (0.12–2.28) * g n6 fatty acids: 5.18 (1.16–19.76) * g Folate: 171.75 ± 68.04 mcg Vitamin B12: 2.92 ±1.29 mcg |
|
| Coupaye (2018) [44] | No | 4 day self-reported food diary (Trimester 2) |
| Mean daily intake: RYGB participants: Energy intake: 1385 ± 400 kcal Protein intake: 59.1 ± 20.9 g Carbohydrate: 164 ± 49 g Fat: 54.8 ± 19.1 g SG participants: Energy: 1222 ± 425 kcal Protein: 46.7 ± 14.5 g Carbohydrate: 152 ± 59 g Fat: 47.3 ± 20.3 g |
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maslin, K.; James, A.; Brown, A.; Bogaerts, A.; Shawe, J. What Is Known About the Nutritional Intake of Women during Pregnancy Following Bariatric Surgery? A Scoping Review. Nutrients 2019, 11, 2116. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092116
Maslin K, James A, Brown A, Bogaerts A, Shawe J. What Is Known About the Nutritional Intake of Women during Pregnancy Following Bariatric Surgery? A Scoping Review. Nutrients. 2019; 11(9):2116. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092116
Chicago/Turabian StyleMaslin, Kate, Alison James, Anne Brown, Annick Bogaerts, and Jill Shawe. 2019. "What Is Known About the Nutritional Intake of Women during Pregnancy Following Bariatric Surgery? A Scoping Review" Nutrients 11, no. 9: 2116. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092116