A Dairy Product to Reconstitute Enriched with Bioactive Nutrients Stops Bone Loss in High-Risk Menopausal Women without Pharmacological Treatment

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Study Design
2.3. Experimental and Placebo Products
2.4. Methods
2.4.1. Diet
2.4.2. Anthropometric, Body Composition and Bone Mass Variables
2.4.3. Physical Activity
2.5. Biochemical Parameters
2.6. Adverse Events
2.7. Statistical Analysis
3. Results
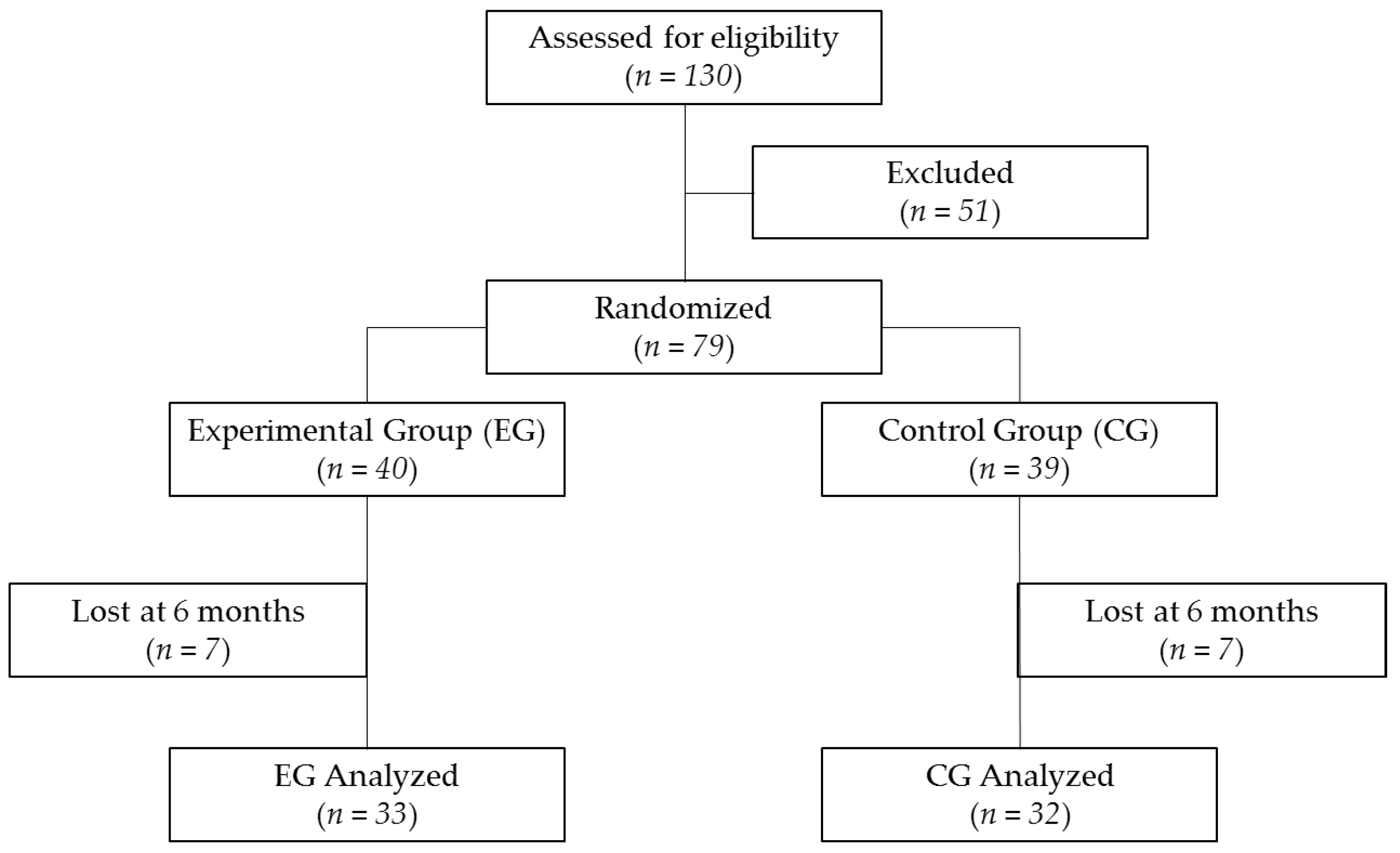
3.1. Recruitment and Study Population
3.2. Baseline Characteristic, Physical Activity and Blood Pressure Variables
3.3. Adverse Events
3.4. Dietetic Intake Variable
3.5. Anthropometric, Bone Body Composition Variables
3.6. Biochemical Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Institutes of Health. NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy, March 7–29, 2000: Highlights of the Conference. South. Med. J. 2001, 94, 569–573. [Google Scholar]
- Pouresmaeili, F.; Dehghan, B.K.; Kamarehei, M.; Goh, Y.M. A comprehensive overview on osteoporosis and its risk factors. Ther. Clin. Risk Manag. 2018, 14, 2029–2049. [Google Scholar] [CrossRef] [Green Version]
- Alibasic, E.; Ljuca, F.; Brkic, S.; Fazlic, M.; Husic, D. Secondary Prevention of Osteoporosis through Assessment of Individual and Multiple Risk Factors. Mater. Socio Medica 2020, 32, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Herrera, A.; Mateo, J.; Gil-Albarova, J.; Lobo-Escolar, A.; Artigas, J.M.; López-Prats, F.; Mesa, M.; Ibarz, E.; Gracia, L. Prevalence of osteoporotic vertebral fracture in Spanish women over age 45. Maturitas 2015, 80, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Borgström, F.; Karlsson, L.; Ortsäter, G.; Norton, N.; Halbout, P.; Cooper, C.; Lorentzon, M.; McCloskey, E.V.; Harvey, N.C.; Javaid, M.K.; et al. Fragility fractures in Europe: Burden, management and opportunities. Arch. Osteoporos. 2020, 15, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ensrud, K.E.; Kats, A.M.; Boyd, C.M.; Diem, S.J.; Schousboe, J.T.; Taylor, B.C.; Bauer, D.C.; Stone, K.L.; Langsetmo, L.; Study of Osteoporotic Fractures (SOF) Research Group; et al. Association of Disease Definition, Comorbidity Burden, and Prognosis With Hip Fracture Probability Among Late-Life Women. JAMA Intern. Med. 2019, 179, 1095–1103. [Google Scholar] [CrossRef]
- Hannafon, F.; Cadogan, M.P. Recognition and treatment of postmenopausal osteoporosis. J. Gerontol. Nurs. 2014, 40, 10–14. [Google Scholar] [CrossRef]
- Kanis, J.A.; Harvey, N.C.; Cooper, C.; Johansson, H.; Odén, A.; McCloskey, E.V.; Advisory Board of the National Osteoporosis Guideline Group. A systematic review of intervention thresholds based on FRAX: A report prepared for the National Osteoporosis Guideline Group and the International Osteoporosis Foundation. Arch. Osteoporos. 2016, 11, 25. [Google Scholar] [CrossRef] [Green Version]
- Link, T.M.; Heilmeier, U. Bone Quality—Beyond Bone Mineral Density. Semin. Musculoskelet. Radiol. 2016, 20, 269–278. [Google Scholar] [CrossRef]
- Binns, N.; Howlett, J. Functional foods in Europe: International Developments in Science and Health Claims: Summary report of an International Symposium held 9–11 May 2007, Portomaso, Malta. Eur. J. Nutr. 2009, 48. [Google Scholar] [CrossRef]
- Sikand, G.; Kris-Etherton, P.; Boulos, N.M. Impact of Functional Foods on Prevention of Cardiovascular Disease and Diabetes. Curr. Cardiol. Rep. 2015, 17, 39. [Google Scholar] [CrossRef] [PubMed]
- Puri, K.S.; Suresh, K.R.; Gogtay, N.J.; Thatte, U.M. Declaration of Helsinki, 2008: Implications for stakeholders in research. J. Postgrad. Med. 2009, 55, 131–134. [Google Scholar] [CrossRef] [PubMed]
- WHO/FAO. Methodology of Nutritional Surveillance. Report of a Joint FAO/UNICEF/WHO Expert Committee; The World Health Organization Technical Report Series; WHO/FAO: Geneva, Switzerland, 1976. [Google Scholar]
- Hagströmer, M.; Oja, P.; Sjöström, M. The International Physical Activity Questionnaire (IPAQ): A study of concurrent and construct validity. Public Health Nutr. 2006, 9, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Hoeck, H.C.; Li, P.; Qvist, P. Changes in 15-Hydroxyvitamin D3 to oral treatment with vitamin D3 in postmenopausal females with osteoporosis. Osteoporos. Int. 2009, 20, 1329–1335. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, B.A.; Harrison, S.L.; Fink, H.A.; Lane, N.E. Study of Osteoporosis Fractures Research Group. Incident fracture is associated with a period of accelerated loss of hip BMD: The Study of Osteoporosis Factures. Osteoporos. Int. 2018, 29, 2201–2209. [Google Scholar] [CrossRef]
- Cicero, A.F.; Fogacci, F.; Bove, M.; Giovannini, M.; Borghi, C. Impact of a short-term synbiotic supplementation on metabolic syndrome and systemic inflammation in elderly patients: A randomized placebo-controlled clinical trial. Eur. J. Nutr. 2020. [Google Scholar] [CrossRef]
- Yilmaz, V.; Umay, E.; Gundogdu, I.; Cakcı, F.A. Effect of Primary Hypertension on Treatment Outcomes of Patients with Postmenopausal Osteoporosis: A 5 Year Follow up Retrospective Study. High Blood Press. Cardiovasc. Prev. 2019, 26, 61–67. [Google Scholar] [CrossRef]
- Rhee, M.Y.; Jeong, Y.J. Sodium Intake, Blood Pressure and Cardiovascular Disease. Korean Circ. J. 2020, 50, 555–571. [Google Scholar] [CrossRef]
- McGrane, M.M.; Essery, E.; Obbagy, J.; Lyon, J.; Macneil, P.; Spahn, J.; Van Horn, L. Dairy Consumption, Blood Pressure, and Risk of Hypertension: An Evidence-Based Review of Recent Literature. Curr. Cardiovasc. Risk Rep. 2011, 5, 287–298. [Google Scholar] [CrossRef] [Green Version]
- Park, K.M.; Cifelli, C.J. Dairy and blood pressure: A fresh look at the evidence. Nutr. Rev. 2013, 71, 149–157. [Google Scholar] [CrossRef]
- McClure, S.T.; Rebholz, C.M.; Medabalimi, S.; Hu, E.A.; Xu, Z.; Selvin, E.; Appel, L.J. Dietary phosphorus intake and blood pressure in adults: A systematic review of randomized trials and prospective observational studies. Am. J. Clin. Nutr. 2019, 109, 1264–1272. [Google Scholar] [CrossRef] [PubMed]
- Fekete, Á.A.; Giromini, C.; Chatzidiakou, Y.; Givens, D.I.; Lovegrove, J.A. Whey protein lowers blood pressure and improves endothelial function and lipid biomarkers in adults with prehypertension and mild hypertension: Results from the chronic Whey2Go randomized controlled trial. Am. J. Clin. Nutr. 2016, 104, 1534–1544. [Google Scholar] [CrossRef]
- Fekete, Á.A.; Givens, D.I.; Lovegrove, J.A. Casein-derived lactotripeptides reduce systolic and diastolic blood pressure in a meta-analysis of randomised clinical trials. Nutrients 2015, 7, 659–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Billington, E.O.; Bristow, S.M.; Gamble, G.D.; de Kwant, J.A.; Stewart, A.; Mihov, B.V.; Horne, A.M.; Reid, I.R. Acute effects of calcium supplements on blood pressure: Randomized, crossover trial in postmenopausal women. Osteoporos. Int. 2017, 28, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Bolland, M.J.; Barber, P.A.; Doughty, R.N.; Mason, B.; Horne, A.; Ames, R.; Gamble, G.D.; Grey, A.; Reid, I.R. Vascular events in healthy older women receiving calcium supplementation: Randomized controlled trial. BMJ 2008, 336, 263–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pentti, K.; Tuppurainen, M.T.; Honkanen, R.; Sandini, L.; Kröger, H.; Alhava, E.; Saarikoski, S. Use of calcium supplements and the risk of coronary heart disease in 52–62-year-old women: The Kuopio Osteoporosis Risk Factor and Prevention Study. Maturitas 2009, 63, 73–78. [Google Scholar] [CrossRef]
- Li, S.; Na, L.; Li, Y.; Gong, L.; Yuan, F.; Niu, Y.; Zhao, Y.; Sun, C. Long-term calcium supplementation may have adverse effects on serum cholesterol and carotid intima-media thickness in postmenopausal women: A double-blind, randomized, placebo-controlled trial. Am. J. Clin. Nutr. 2013, 98, 1353–1359. [Google Scholar] [CrossRef] [Green Version]
- Cesareo, R.; Iozzino, M.; D’onofrio, L.; Terrinoni, I.; Maddaloni, E.; Casini, A.; Campagna, G.; Santonati, A.; Palermo, A. Effectiveness and safety of calcium and vitamin D treatment for postmenopausal osteoporosis. Minerva Endocrinol. 2015, 40, 231–237. [Google Scholar]
- Chrysant, S.G.; Chrysant, G.S. Controversy regarding the association of high calcium intake and increased risk for cardiovascular disease. J. Clin. Hypertens. 2014, 16, 545–550. [Google Scholar] [CrossRef]
- Weaver, C.M.; Alexander, D.D.; Boushey, C.J.; Dawson-Hughes, B.; Lappe, J.M.; LeBoff, M.S.; Liu, S.; Looker, A.C.; Wallace, T.C.; Wang, D.D. Calcium plus vitamin D supplementation and risk of fractures: An updated meta-analysis from the National Osteoporosis Foundation. Osteoporos. Int. 2016, 27, 367–376. [Google Scholar] [CrossRef] [Green Version]
- Ralston, R.A.; Lee, J.H.; Truby, H.; Palermo, C.E.; Walker, K.Z. A Systematic Review and Meta-Analysis of Elevated Blood Pressure and Consumption of Dairy Foods. J. Hum. Hypertens. 2012, 26, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhavadharini, B.; Dehghan, M.; Mente, A.; Rangarajan, S.; Sheridan, P.; Mohan, V.; Iqbal, R.; Gupta, R.; Lear, S.; Wentzel-Viljoen, E.; et al. Association of dairy consumption with metabolic syndrome, hypertension and diabetes in 147 812 individuals from 21 countries. BMJ Open Diabetes Res. Care 2020, 8, e00026. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.T.; Moore, C.E.; Radcliffe, J.D. Consumption of Calcium-Fortified Cereal Bars to Improve Dietary Calcium Intake of Healthy Women: Randomized Controlled Feasibility Study. PLoS ONE 2015, 10, e0125207. [Google Scholar] [CrossRef] [PubMed]
- González Sánchez, M.E.; Rivera Torres, A.; Morán Fagúndez, L.J. Nutritional trial to evaluate calcium intake in postmenopausic women on a diet of fermented milk enriched in calcium and vitamin D (Densia®). Nutr. Hosp. 2012, 27, 537–541. [Google Scholar] [CrossRef]
- Black, L.J.; Seamans, K.M.; Cashman, K.D.; Kiely, M. An Updated Systematic Review and Meta-Analysis of the Efficacy of Vitamin D Food Fortification. J. Nutr. 2012, 142, 1102–1108. [Google Scholar] [CrossRef] [Green Version]
- Silva, T.R.; Franz, R.; Maturana, M.A.; Spritzer, P.M. Associations between body composition and lifestyle factors with bone mineral density according to time since menopause in women from Southern Brazil: A cross-sectional study. BMC Endocr. Disord. 2015, 15, 71. [Google Scholar] [CrossRef] [Green Version]
- Morrison, S.A.; Petri, R.M.; Hunter, H.L.; Raju, D.; Gower, B. Comparison of the Lunar Prodigy and iDXA Dual-Energy X-ray Absorptiometers for Assessing Total and Regional Body Composition. J. Clin. Densitom. 2016, 19, 290–297. [Google Scholar] [CrossRef] [Green Version]
- Batur, P.; Rice, S.; Barrios, P.; Sikon, A. Osteoporosis Management. J. Womens Health 2017, 26, 918–921. [Google Scholar] [CrossRef]
- Sahni, S.; Mangano, K.M.; Kiel, D.P.; Tucker, K.L.; Hannan, M.T. Dairy Intake Is Protective against Bone Loss in Older Vitamin D Supplement Users: The Framingham Study. J. Nutr. 2017, 147, 645–652. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Xiao, Y.; Xie, B.; Zhang, Q.; Ma, X.; Li, N.; Liu, M.; Zhang, Q. Effect of Milk Powder Supplementation with Different Calcium Contents on Bone Mineral Density of Postmenopausal Women in Northern China: A Randomized Controlled Double-Blind Trial. Calcif. Tissue Int. 2016, 98, 60–66. [Google Scholar] [CrossRef]
- Gui, J.-C.; Brašić, J.R.; Liu, X.-D.; Gong, G.-Y.; Zhang, G.-M.; Liu, C.-J.; Gao, G.-Q. Bone Mineral Density in Postmenopausal Chinese Women Treated with Calcium Fortification in Soymilk and Cow’s Milk. Osteoporos. Int. 2012, 23, 1563–1570. [Google Scholar] [CrossRef] [PubMed]
- Kruger, M.C.; Chan, Y.M.; Lau, L.T.; Lau, C.C.; Chin, Y.S.; Kuhn-Sherlock, B.; Todd, J.M.; Schollum, L.M. Calcium and vitamin D fortified milk reduces bone turnover and improves bone density in postmenopausal women over 1 year. Eur. J. Nutr. 2018, 57, 2785–2794. [Google Scholar] [CrossRef] [PubMed]
- Kruger, M.C.; von Hurst, P.R.; Booth, C.L.; Kuhn-Sherlock, B.; Todd, J.M.; Schollum, L.M. Postprandial metabolic responses of serum calcium, parathyroid hormone and C-telopeptide of type I collagen to three doses of calcium delivered in milk. J. Nutr. Sci. 2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jafarnejad, S.; Djafarian, K.; Fazeli, M.R.; Yekaninejad, M.S.; Rostamian, A.; Keshavarz, S.A. Effects of a Multispecies Probiotic Supplement on Bone Health in Osteopenic Postmenopausal Women: A Randomized, Double-blind, Controlled Trial. J. Am. Coll. Nutr. 2017, 36, 497–506. [Google Scholar] [CrossRef]
- Rizzoli, R.; Biver, E. Effects of Fermented Milk Products on Bone. Calcif. Tissue Int. 2018, 102, 489–500. [Google Scholar] [CrossRef]
- Biver, E.; Durosier-Izart, C.; Merminod, F.; Chevalley, T.; van Rietbergen, B.; Ferrari, S.L.; Rizzoli, R. Fermented dairy products consumption is associated with attenuated cortical bone loss independently of total calcium, protein, and energy intakes in healthy postmenopausal women. Osteoporos. Int. 2018, 29, 1771–1782. [Google Scholar] [CrossRef]
- Rizzoli, R.; Biver, E. Are Probiotics the New Calcium and Vitamin D for Bone Health? Curr. Osteoporos. Rep. 2020, 18, 273–284. [Google Scholar] [CrossRef]
- Kruger, M.C.; Ha, P.C.; Todd, J.M.; Kuhn-Sherlock, B.; Schollum, L.M.; Ma, J.; Qin, G.; Lau, E. High-calcium, vitamin D fortified milk is effective in improving bone turnover markers and vitamin D status in healthy postmenopausal Chinese women. Eur. J. Clin. Nutr. 2012, 66, 856–861. [Google Scholar] [CrossRef] [Green Version]
- Iuliano, S.; Hill, T.R. Dairy foods and bone health throughout the lifespan: A critical appraisal of the evidence. Br. J. Nutr. 2019, 121, 763–772. [Google Scholar] [CrossRef] [Green Version]
- Manios, Y.; Moschonis, G.; Mavrogianni, C.; van den Heuvel, E.; Singh-Povel, C.M.; Kiely, M.; Cashman, K.D. Reduced-fat Gouda-type cheese enriched with vitamin D3 effectively prevents vitamin D deficiency during winter months in postmenopausal women in Greece. Eur. J. Nutr. 2017, 56, 2367–2377. [Google Scholar] [CrossRef]
- Kaushik, R.; Sachdeva, B.; Arora, S.; Kapila, S.; Wadhwa, B.K. Bioavailability of vitamin D₂ and calcium from fortified milk. Food Chem. 2014, 147, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Takahata, M. Bone Cell Biology Assessed by Microscopic Approach. The effect of parathyroid hormone and teriparatide on bone. Clin. Calcium 2015, 25, 1529–1535. [Google Scholar]
- Jamal, S.A.; Miller, P.D. Secondary and tertiary hyperparathyroidism. J. Clin. Densitom. 2013, 16, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Bonjour, J.-P.; Benoit, V.; Payen, F.; Kraenzlin, M. Consumption of Yogurts Fortified in Vitamin D and Calcium Reduces Serum Parathyroid Hormone and Markers of Bone Resorption: A Double-Blind Randomized Controlled Trial in Institutionalized Elderly Women. J. Clin. Endocrinol. Metab. 2013, 98, 2915–2921. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Zhao, M.; Xu, Z. The effects of differing resistance training modes on the preservation of bone mineral density in postmenopausal women: A meta-analysis. Osteoporos. Int. 2015, 26, 1605–1618. [Google Scholar] [CrossRef] [PubMed]
- Kelley, G.A.; Kelley, K.S.; Kohrt, W.M. Effects of ground and joint reaction force exercise on lumbar spine and femoral neck bone mineral density in postmenopausal women: A meta-analysis of randomized controlled trials. BMC Musculoskelet. Disord. 2012, 13, 177. [Google Scholar] [CrossRef] [Green Version]
- Whiting, S.J.; Kohrt, W.M.; Warren, M.P.; Kraenzlin, M.I.; Bonjour, J.P. Food fortification for bone health in adulthood: A scoping review. Eur. J. Clin. Nutr. 2016, 70, 1099–1105. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| EG | CG | |
|---|---|---|
| Energy (kcal) | 126 | 123 |
| Lipid (g) | 2.06 | 2.06 |
| saturated (g) | 1.8 | 1.8 |
| Carbohydrates (g) | 23 | 23 |
| sugars (g) | 18 | 18 |
| Protein (g) | 1.8 | 1.8 |
| Calcium (mg) | 501 | 227 |
| Vitamin D3 (μg) | 6 | 0.015 |
| Vitamin K (μg) | 80 | - |
| Vitamin C (mg) | 100 | - |
| Zinc Gluconate (mg) | 10.39 | - |
| Dicitrate of Trimagnesium (mg) | 250.5 | - |
| L-Leucin (g) | 1 | - |
| Lactobacillus plantarum 3547 (ufc) | 1 × 1010 | - |
| CG | EG | ||||||
|---|---|---|---|---|---|---|---|
| Week 0 | Week 24 | Change | Week 0 | Week 24 | Change | ||
| Fasting plasma glucose | mg/dL | 92.13 ± 7.43 | 96.13 ± 8.3 * | 4.00 ± 6.74 | 90.76 ± 7.96 | 94.91 ± 8.77 * | 4.15 ± 8.78 |
| Plasma insulin | µU/mL | 8.78 ± 5.38 | 9.88 ± 8.11 | 1.10 ± 6.38 | 8.50 ± 4.82 | 9.42 ± 4.23 | 0.91 ± 3.79 |
| Total cholesterol | mg/dL | 217.26 ± 29.69 | 210.59 ± 24.95 * | −6.69 ± 23.3 | 211.18 ± 35.41 | 204.88 ± 35.41 * | −6.30 ± 22.09 |
| LDL-cholesterol | mg/dL | 137.09 ± 27.33 | 128.56 ± 23.00 * | −8.53 ± 18.5 | 131.03 ± 29.87 | 123.91 ± 26.93 * | −7.12 ± 19.91 |
| HDL-cholesterol | mg/dL | 63.19 ± 14.71 | 62.16 ± 12.54 | −1.03 ± 10.3 | 61.91 ± 14.16 | 61.71 ± 13.63 | −0.12 ± 5.73 |
| Triglycerides | mg/dL | 84.84 ± 31.12 | 87.09 ± 46.26 | 2.25 ± 31.85 | 91.76 ± 43.68 | 94.30 ± 39.44 | 2.54 ± 27.99 |
| Creatinine | mg/dL | 0.64 ± 0.10 | 0.65 ± 0.12 | 0.01 ± 0.02 | 0.64 ± 0.09 | 0.65 ± 0.08 | 0.01 ± 0.01 |
| Urate | mg/dL | 4.32 ± 1.17 | 4.37 ± 1.13 | 0.05 ± 0.92 | 4.13 ± 0.82 | 4.18 ± 0.98 | 0.05 ± 0.58 |
| Aspartate transaminase | UI/L | 22.81 ± 7.00 | 22.47 ± 6.34 | −0.34 ± 5.26 | 24.33 ± 8.24 | 24.52 ± 11.24 | 0.18 ± 5.97 |
| Alanine transaminase | UI/L | 23.13 ± 10.45 | 23.13 ± 11.86 | 0.00 ± 5.35 | 24.12 ± 10.74 | 22.70 ± 11.94 | −1.42 ± 8.12 |
| Alkaline phosphatase | UI/L | 87.75 ± 23.26 | 88.05 ± 23.64 | 0.30 ± 11.43 | 81.42 ± 19.53 | 81.75 ± 17.69 | 0.33 ± 10.6 |
| Bilirubin | mg/dL | 0.53 ± 0.16 | 0.57 ± 0.15 | 0.04 ± 0.21 | 0.55 ± 0.22 | 0.59 ± 0.19 | 0.04 ± 0.21 |
| CG | EG | ||||||
|---|---|---|---|---|---|---|---|
| Week 0 | Week 24 | Change | Week 0 | Week 24 | Change | ||
| Energy | (kcal) | 2025.24 ± 238.45 | 1829.4 ± 355.5 ** | −195.76 ± 359.9 | 2036.14 ± 244.83 | 1818.7 ± 304.1 ** | −217.39 ± 306.7 |
| Carbohydrates | (%) | 36.13 ± 6.15 | 33.35 ± 6.38 ** | −2.78 ± 6.16 | 36.46 ± 5.94 | 32.89 ± 7.24 ** | −3.57 ± 6.38 |
| Proteins | (%) | 16.94 ± 3.00 | 17.78 ± 3.05 | 0.84 ± 2.31 | 18.15 ± 2.53 | 17.89 ± 3.08 | −0.27 ± 3.42 |
| Lipid | (%) | 46.93 ± 3.61 | 48.87 ± 3.52 * | 1.94 ± 3.32 | 45.39 ± 4.46 | 48.22 ± 8.25 * | 2.83 ± 2.29 |
| SFA | (%) | 14.97 ± 3.32 | 15.39 ± 2.21 | 0.42 ± 1.08 | 14.57 ± 2.48 | 15.26 ± 2.57 | 0.69 ± 2.27 |
| MFA | (%) | 26.26 ± 4.10 | 27.70 ± 4.60 * | 1.44 ± 5.79 | 24.89 ± 4.50 | 27.54 ± 5.68 * | 2.65 ± 5.51 |
| PFA | (%) | 5.70 ± 1.90 | 5.78 ± 1.35 | 1.08 ± 2.30 | 5.93 ± 2.23 | 6.42 ± 2.64 | 0.49 ± 2.61 |
| Total Cholesterol | (mg/day) | 324.38 ± 70.62 | 291.48 ± 92.94 * | −32.90 ± 90.93 | 339.46 ± 92.16 | 289.43 ± 80.80 * | −50.03 ± 19.02 |
| Fibre | (g/day) | 22.30 ± 7.62 | 26.01 ± 5.17 * | 3.71 ± 13.71 | 21.42 ± 5.69 | 29.73 ± 5.51 * | 8.31 ± 36.52 |
| Calcium | (mg/day) | 759.24 ± 13.74 | 794.52 ± 18.62 | 35.28 ± 27.21 | 776.39 ± 29.67 | 959.75 ± 266.2 * | 183.36 ± 334.0 # |
| Vitamin D | (µg/day) | 12.99 ± 2.34 | 13.39 ± 2.59 | 0.40 ± 3.31 | 13.35 ± 2.61 | 16.10 ± 2.93 * | 2.75 ± 3.19 # |
| CG | EG | ||||||
|---|---|---|---|---|---|---|---|
| Week 0 | Week 24 | Change | Week 0 | Week 24 | Change | ||
| Weight | (kg) | 66.71 ± 12.32 | 66.21 ± 12.10 | −0.49 ± 2.93 | 67.22 ± 10.13 | 66.61 ± 9.41 | −0.61 ± 3.52 |
| BMI | (kg/m2) | 26.47 ± 4.11 | 26.39 ± 4.20 | −0.08 ± 1.13 | 26.34 ± 3.19 | 26.2 ± 3.20 | −0.14 ± 1.53 |
| Waist circ. | (cm) | 88.89 ± 11.54 | 88.7 ± 12.22 | 0.19 ± 7.02 | 89.01 ± 11.42 | 88.54 ± 11.81 | −0.47 ± 5.82 |
| BMD | (kg/cm2) | 1.05 ± 0.10 | 1.04 ± 0.10 ** | −0.01 ± 0.01 | 1.04 ± 0.11 | 1.04 ± 0.11 | 0.00 ± 0.00 # |
| T-Score | −0.28 ± 1.04 | −0.36 ± 0.10 ** | −0.08 ± 0.13 | −0.40 ± 1.04 | −0.40 ± 1.04 | 0.00 ± 0.00 # | |
| Z-Score | 0.36 ± 0.94 | 0.37 ± 0.90 | 0.02 ± 0.22 | 0.20 ± 1.04 | 0.23 ± 1.03 | 0.03 ± 12 | |
| BM | (kg) | 2.09 ± 3.12 | 2.08 ± 0.30 * | −0.01 ± 0.03 | 2.07 ± 0.26 | 2.08 ± 0.26 * | 0.01 ± 0.03 # |
| FM | (kg) | 27.32 ± 9.30 | 27.24 ± 8.84 | −0.08 ± 0.02 | 27.52 ± 7.53 | 27.78 ± 7.57 | 0.26 ± 1.13 |
| LM | (kg) | 36.61 ± 3.76 | 36.23 ± 3.98 | −0.38 ± 0.22 | 37.69 ± 3.59 | 37.53 ± 3.61 | −0.17 ± 0.86 |
| FFM | (kg) | 38.71 ± 3.98 | 38.31 ± 4.17 | −0.40 ± 0.19 | 39.76 ± 3.72 | 39.59 ± 3.75 | −0.17 ± 0.86 |
| CG | EG | ||||||
|---|---|---|---|---|---|---|---|
| Week 0 | Week 24 | Change | Week 0 | Week 24 | Change | ||
| P1NP | ng/mL | 59.37 ± 13.70 | 55.16 ± 17.15 | −4.21 ± 15.62 | 58.17 ± 13.26 | 71.36 ± 5.50 ** | 13.19 ± 25.17 # |
| CTx | ng/mL | 0.49 ± 0.20 | 0.53 ± 0.23 | 0.04 ± 0.14 | 0.50 ± 0.19 | 0.46 ± 0.16 | −0.05 ± 0.19 # |
| Calcium | mg/dL | 9.65 ± 0.29 | 9.62 ± 0.26 | −0.03 ± 0.33 | 9.54 ± 0.35 | 9.57 ± 0.30 | 0.03 ± 0.38 |
| Phosphorus | mg/dL | 3.63 ± 0.52 | 3.68 ± 0.39 | 0.05 ± 0.46 | 3.69 ± 0.46 | 3.77 ± 0.34 | 0.08 ± 0.41 |
| Vitamin D | ng/mL | 17.97 ± 9.70 | 19.89 ± 5.13 | 1.93 ± 6.60 | 19.24 ± 7.07 | 23.73 ± 15.6 * | 4.49 ± 13.94 # |
| Calcitonin | pg/mL | 2.09 ± 0.40 | 2.07 ± 0.31 | −0.02 ± 0.28 | 2.12 ± 0.43 | 2.13 ± 0.01 | 0.01 ± 0.43 |
| PTH | pg/mL | 83.19 ± 26.63 | 100.47 ± 14.2 * | 17.28 ± 12.46 | 85.89 ± 24.35 | 82.12 ± 21.06 | −3.77 ± 23.29 # |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morato-Martínez, M.; López-Plaza, B.; Santurino, C.; Palma-Milla, S.; Gómez-Candela, C. A Dairy Product to Reconstitute Enriched with Bioactive Nutrients Stops Bone Loss in High-Risk Menopausal Women without Pharmacological Treatment. Nutrients 2020, 12, 2203. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082203
Morato-Martínez M, López-Plaza B, Santurino C, Palma-Milla S, Gómez-Candela C. A Dairy Product to Reconstitute Enriched with Bioactive Nutrients Stops Bone Loss in High-Risk Menopausal Women without Pharmacological Treatment. Nutrients. 2020; 12(8):2203. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082203
Chicago/Turabian StyleMorato-Martínez, Marina, Bricia López-Plaza, Cristina Santurino, Samara Palma-Milla, and Carmen Gómez-Candela. 2020. "A Dairy Product to Reconstitute Enriched with Bioactive Nutrients Stops Bone Loss in High-Risk Menopausal Women without Pharmacological Treatment" Nutrients 12, no. 8: 2203. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082203