Evaluation of a Mobile Phone Image-Based Dietary Assessment Method in Adults with Type 2 Diabetes


Abstract
:1. Introduction
2. Experimental Section
2.1. Subjects and Study Design
2.2. Total Energy Expenditure (TEE)
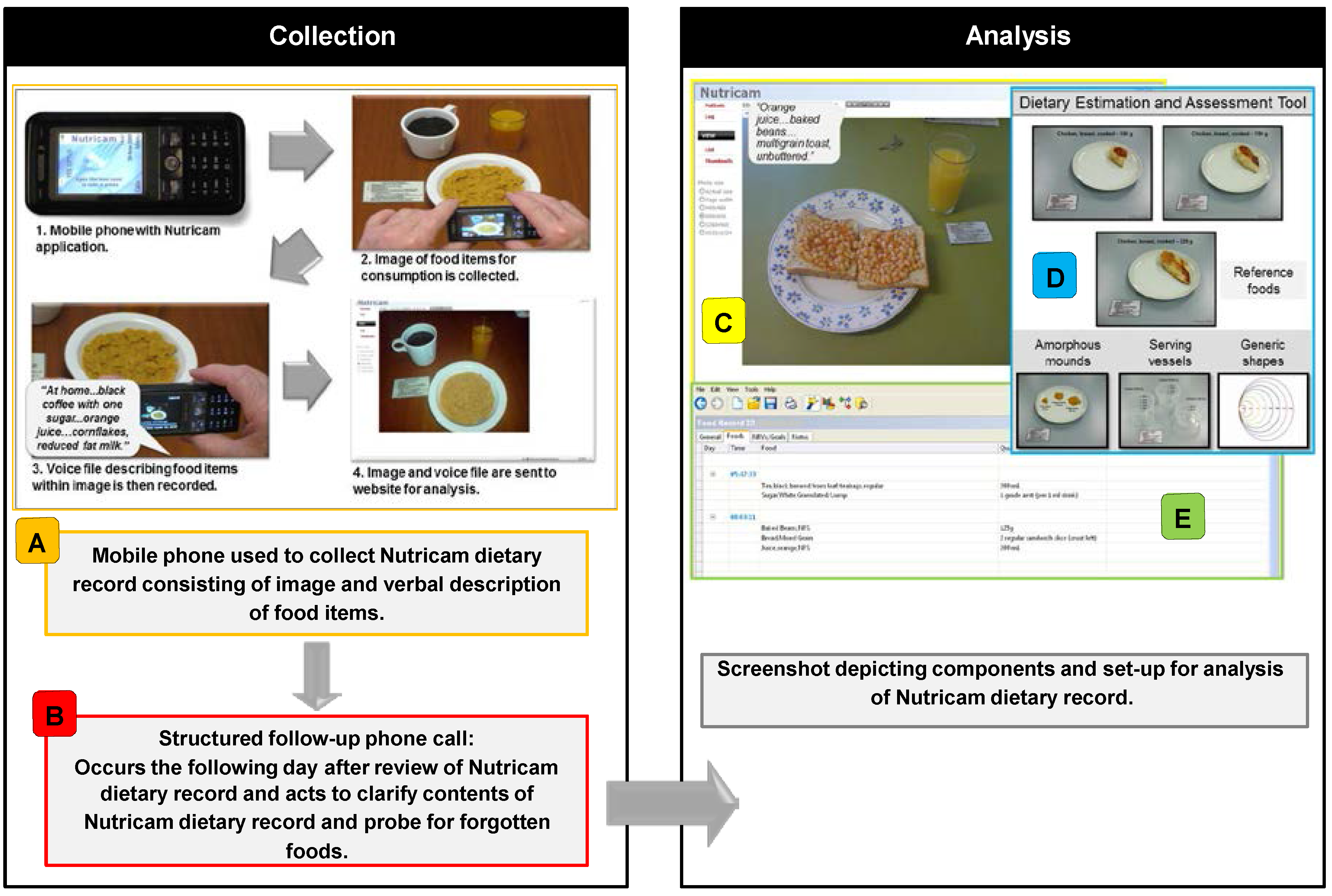
2.3. Nutricam Dietary Assessment Method (NuDAM)

2.4. Weighed Food Record (WFR)
2.5. Nutrient Analysis from the NuDAM and WFR
2.6. Statistical Analysis
3. Results
3.1. Criterion and Relative Validity
3.2. Inter-Rater Reliability
3.3. Usability, Acceptability and Changes to Eating Behaviours

{kind=link}
| Mean(± SD) Intake as Assessed by Each Dietitian † | ICC (95% CI) between Dietitians | Overall ‡ | |||||
|---|---|---|---|---|---|---|---|
| D1 | D2 | D3 | Mean ( ± SD) Intake § | Correlation ^ between Methods | |||
| Energy (MJ/day) | NuDAM | 8.2 ± 1.7 | 9.0 ± 2.3 * | 9.1 ± 2.0 * | 0.88 (0.58–0.98) *** | 8.8 ± 2.0 | 0.57 |
| WFR | 8.5 ± 1.6 | 8.9 ± 2.0 | 8.9 ± 1.8 | 0.92 (0.80–0.98) *** | 8.8 ± 1.8 | ||
| Protein (g/day) | NuDAM | 89.3 ± 20.2 | 99.0 ± 31.4 | 98.1 ± 23.1 * | 0.79 (0.53–0.94) *** | 95.5 ± 23.7 | 0.78 ** |
| WFR | 89.1 ± 26.8 | 91.9 ± 28.2 | 91.5 ± 24.9 | 0.97 (0.92–0.99) *** | 90.8 ± 26.4 | ||
| Fat (g/day) | NuDAM | 75.6 ± 18.3 | 87.0 ± 25.4 * | 86.6 ± 20.1 | 0.77 (0.45–0.93) *** | 83.1 ± 20.3 | 0.24 |
| WFR | 79.5 ± 16.8 | 85.4 ± 27.4 | 80.9 ± 24.2 | 0.82 (0.59–0.95) *** | 81.9 ± 21.8 | ||
| CHO (g/day) | NuDAM | 194.9 ± 52.8 | 212.0 ± 52.7 * | 215.3 ± 60.8 | 0.91 (0.71–0.98) *** | 207.4 ± 54.4 | 0.63 * |
| WFR | 206.3 ± 53.8 | 207.2 ± 54.9 | 211.9 ± 57.8 | 0.92 (0.79–0.98) *** | 208.5 ± 53.9 | ||
| Alcohol (g/day) #,¶ | NuDAM | 15.0 ± 29.4 | 13.6 ± 28.0 | 14.4 ± 29.5 | 0.99 (0.98–0.99) *** | 14.3 ± 28.9 | 0.85 ** |
| WFR | 16.1 ± 23.4 | 17.4 ± 30.2 | 16.5 ± 28.4 | 0.99 (0.98–0.99) *** | 16.7 ± 28.3 | ||
| Questions (as Presented): | Count | |||
|---|---|---|---|---|
| Usability and Acceptability ^ | Strongly Agree | Agree | Neutral | Disagree |
| Overall, I found the Nutricam mobile phone easy to use: | 7 | 2 | 1 | 0 |
| Overall, I found weighing my foods and drinks easy: | 0 | 3 | 4 | 3 |
| NuDAM only: | ||||
| I found taking photographs of food and drink items easy *: | 5 | 5 | 0 | 0 |
| I found recording the voice file easy *: | 5 | 5 | 0 | 0 |
| I found that the Prompt Card was useful for remembering how to use Nutricam: | 5 | 1 | 4 | 0 |
| When prompted during the call: I found it easy to clarify the details of the food and/or drink items that I had eaten during the previous day: | 8 | 1 | 1 | 0 |
| I found it easy to remember if there were any food and/or drink items I had not recorded using the Nutricam mobile phone the previous day: | 7 | 3 | 0 | 0 |
| I found it easy to remember the description of the food and/or drink items I had not recorded using the Nutricam mobile phone the previous day: | 6 | 4 | 0 | 0 |
| I found it easy to remember the quantities of the food and/or drink items I had not recorded using the Nutricam mobile phone the previous day: | 6 | 3 | 1 | 0 |
| Overall, I found that the length of the calls I received were appropriate: | 5 | 4 | 1 | 0 |
| Change to eating behaviours | No | Yes | ||
| Was there any difference in how you used the Nutricam mobile phone to record your diet when you were alone compared to when you were with other people or in public? | 4 | 6 | ||
| Was there any difference in how you recorded your diet using the weighed record method when you were alone, compared to when you were with other people or in public? | 2 | 8 | ||
| Did you record all food and drink items that you consumed during the test period using the Nutricam mobile phone? | 5 | 5 | ||
| Did you record all food and drink items that you consumed during the test period using the weighed record method? | 4 | 6 | ||
| Where there any foods and/or drinks that you usually eat, but did not eat during the Nutricam test period? | 9 | 1 | ||
| Where there any foods and/or drinks that you usually eat, but did not eat during the weighed record method test period? | 6 | 4 | ||
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care 2014, 37, S14–S80. [Google Scholar]
- Nelson, M.; Bingham, S.A. Assessment of food consumption and nutrient intake. In Design Concepts in Nutrional Epidemiology; Margetts, B., Nelson, M., Eds.; Oxford University Press: New York, NY, USA, 1997. [Google Scholar]
- Mela, D.J.; Aaron, J.I. Honest but invalid: What subjects say about recording their food intake. J. Am. Diet. Assoc. 1997, 97, 791–793. [Google Scholar] [CrossRef]
- Rebro, S.M.; Patterson, R.E.; Kristal, A.R.; Cheney, C.L. The effect of keeping food records on eating patterns. J. Am. Diet. Assoc. 1998, 98, 1163–1165. [Google Scholar] [CrossRef]
- Vuckovic, N.; Ritenbaugh, C.; Taren, D.L.; Tobar, M. A qualitative study of participants’ experiences with dietary assessment. J. Am. Diet. Assoc. 2000, 100, 1023–1028. [Google Scholar] [CrossRef]
- Daugherty, L.B.; Schap, E.T.; Ettienne-Gittens, R.; Zhu, M.F.; Bosch, M.; Delp, J.E.; Ebert, S.D.; Kerr, A.D.; Boushey, J.C. Novel technologies for assessing dietary intake: Evaluating the usability of a mobile telephone food record among adults and adolescents. J. Med. Internet Res. 2012, 14, e58. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.K.; Correa, J.B.; Han, H.; Allen, H.R.; Rood, J.C.; Champagne, C.M.; Gunturk, B.K.; Bray, G.A. Validity of the remote food photography method (RFPM) for estimating energy and nutrient intake in near real-time. Obesity 2012, 20, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Rollo, M.E.; Ash, S.; Lyons-Wall, P.; Russell, A. Trial of a mobile phone method for recording dietary intake in adults with type 2 diabetes: Evaluation and implications for future applications. J. Telemed. Telecare 2011, 17, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Kikunaga, S.; Tin, T.; Ishibashi, G.; Wang, D.H.; Kira, S. The application of a handheld personal digital assistant with camera and mobile phone card (Wellnavi) to the general population in a dietary survey. J. Nutr. Sci. Vitaminol. (Tokyo) 2007, 53, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.H.; Kogashiwa, M.; Kira, S. Development of a new instrument for evaluating individuals’ dietary intakes. J. Am. Diet. Assoc. 2006, 106, 1588–1593. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.H.; Kogashiwa, M.; Ohta, S.; Kira, S. Validity and reliability of a dietary assessment method: The application of a digital camera with a mobile phone card attachment. J. Nutr. Sci. Vitaminol. (Tokyo) 2002, 48, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Bird, G.; Elwood, P.C. The dietary intakes of subjects estimated from photographs compared with a weighed record. Hum. Nutr. Appl. Nutr. 1983, 37, 470–473. [Google Scholar] [PubMed]
- Lassen, A.D.; Poulsen, S.; Ernst, L.; Andersen, K.K.; Biltoft-Jensen, A.; Tetens, I. Evaluation of a digital method to assess evening meal intake in a free-living adult population. Food Nutr. Res 2010, 54. [Google Scholar] [CrossRef]
- Martin, C.K.; Han, H.M.; Coulon, S.M.; Allen, H.R.; Champagne, C.M.; Anton, S.D. A novel method to remotely measure food intake of free-living individuals in real time: The remote food photography method. Br. J. Nutr. 2009, 101, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Gleason, P.M.; Harris, J.; Sheean, P.M.; Boushey, C.J.; Bruemmer, B. Publishing nutrition research: Validity, reliability, and diagnostic test assessment in nutrition-related research. J. Am. Diet. Assoc. 2010, 110, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Black, A.E.; Prentice, A.M.; Goldberg, G.R.; Jebb, S.A.; Bingham, S.A.; Livingstone, M.B.; Coward, W.A. Measurements of total energy expenditure provide insights into the validity of dietary measurements of energy intake. J. Am. Diet. Assoc. 1993, 93, 572–579. [Google Scholar] [CrossRef]
- Livingstone, M.B.E.; Black, A.E. Markers of the validity of reported energy intake. J. Nutr. 2003, 133, 895S–920S. [Google Scholar] [PubMed]
- Nelson, M. The validation of dietary assessment. In Design Concepts in Nutritional Epidemiology, 2nd ed.; Margetts, B.M., Nelson, M., Eds.; Oxford University Press: New York, NY, USA, 1997. [Google Scholar]
- Van Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P.B. The dutch eating behavior questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behaviours. Int. J. Eat. Disord. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Schoeller, D.A. Hydrometry. In Human Body Composition; Roche, A.F., Ed.; Human Kinetics: Champaign, IL, USA, 1996. [Google Scholar]
- Racette, S.B.; Schoeller, D.A.; Luke, A.H.; Shay, K.; Hnilicka, J.; Kushner, R.F. Relative dilution spaces of 2h- and 18O-labeled water in humans. Am. J. Physiol. 1994, 267, E585–E590. [Google Scholar] [PubMed]
- Weir, J.B. New methods for calculating metabolic rate with special reference to protein metabolism. J. Physiol. 1949, 109, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Australia New Zealand Food Authority. AUSNUT 1999—Australian Food and Nutrient Database 1999; Australia New Zealand Food Authority: Canberra, Australia, 1999.
- McBride, J. Was it a slice, a slab or a sliver? Agric. Res. 2001, 3, 4–7. [Google Scholar]
- Nelson, M.; Atkinson, M.; Darbyshire, S. Food photography II: Use of food photographs for estimating portion size and the nutrient content of meals. Br. J. Nutr. 1996, 76, 31–49. [Google Scholar] [CrossRef] [PubMed]
- Black, A.E.; Cole, T.J. Biased over- or under-reporting is characteristic of individuals whether over time or by different assessment methods. J. Am. Diet. Assoc. 2001, 101, 70–80. [Google Scholar] [CrossRef]
- Goran, M.I.; Poehlman, E.T. Total energy expenditure and energy requirements in healthy elderly persons. Metabolism 1992, 41, 744–753. [Google Scholar] [CrossRef]
- Johnson, R.K.; Goran, M.I.; Poehlman, E.T. Correlates of over-and underreporting of energy intake in healthy older men and women. Am. J. Clin. Nutr. 1994, 59, 1286–1290. [Google Scholar] [PubMed]
- Tomoyasu, N.J.; Toth, M.J.; Poehlman, E.T. Misreporting of total energy intake in older men and women. J. Am. Geriatr. Soc. 1999, 47, 710–715. [Google Scholar] [CrossRef] [PubMed]
- Sallé, A.; Ryan, M.; Ritz, P. Underreporting of food intake in obese diabetic and nondiabetic patients. Diabetes Care 2006, 29, 2726–2727. [Google Scholar] [CrossRef] [PubMed]
- Van Strien, T. Success and failure in the measurement of restraint: Notes and data. Int. J. Eat. Disord. 1999, 25, 441–449. [Google Scholar] [CrossRef]
- Rennie, K.L.; Siervo, M.; Jebb, S.A. Can self-reported dieting and dietary restraint identify underreporters of energy intake in dietary surveys? J. Am. Diet. Assoc. 2006, 106, 1667–1672. [Google Scholar] [CrossRef] [PubMed]
- Poppitt, S.D.; Swann, D.; Black, A.E.; Prentice, A.M. Assessment of selective under-reporting of food intake by both obese and non-obese women in a metabolic facility. Int. J. Obes. Relat. Metab. Disord. 1998, 22, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Goris, A.H.; Westerterp-Plantenga, M.S.; Westerterp, K.R. Undereating and underrecording of habitual food intake in obese men: Selective underreporting of fat intake. Am. J. Clin. Nutr. 2000, 71, 130–134. [Google Scholar] [PubMed]
- Gemming, L.; Doherty, A.; Kelly, P.; Utter, J.; Ni Mhurchu, C. Feasibility of a sensecam-assisted 24-h recall to reduce under-reporting of energy intake. Eur. J. Clin. Nutr. 2013, 67, 1095–1099. [Google Scholar] [CrossRef] [PubMed]
- Jia, W.; Chen, H.C.; Yue, Y.; Li, Z.; Fernstrom, J.; Bai, Y.; Li, C.; Sun, M. Accuracy of food portion size estimation from digital pictures acquired by a chest-worn camera. Public Health Nutr. 2014, 17, 1671–1681. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.D.; Chae, J.; Schap, T.E.; Kerr, D.A.; Delp, E.J.; Ebert, D.S.; Boushey, C.J. Comparison of known food weights with image-based portion-size automated estimation and adolescents’ self-reported portion size. J. Diabetes Sci. Technol. 2012, 6, 428–434. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rollo, M.E.; Ash, S.; Lyons-Wall, P.; Russell, A.W. Evaluation of a Mobile Phone Image-Based Dietary Assessment Method in Adults with Type 2 Diabetes. Nutrients 2015, 7, 4897-4910. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7064897
Rollo ME, Ash S, Lyons-Wall P, Russell AW. Evaluation of a Mobile Phone Image-Based Dietary Assessment Method in Adults with Type 2 Diabetes. Nutrients. 2015; 7(6):4897-4910. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7064897
Chicago/Turabian StyleRollo, Megan E., Susan Ash, Philippa Lyons-Wall, and Anthony W. Russell. 2015. "Evaluation of a Mobile Phone Image-Based Dietary Assessment Method in Adults with Type 2 Diabetes" Nutrients 7, no. 6: 4897-4910. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7064897