
Positioning a Paediatric Compounded Non-Sterile Product Electronic Repository (pCNPeRx) within the Health Information Technology Infrastructure


Abstract
:1. Introduction

{kind=link}
{kind=link}
{kind=link}
| 2017 Pharmacy HIT Goals | Key Strategies Related to Pharmacy Paediatrics |
|---|---|
| Goal 1: Ensure that HIT supports pharmacists in health care service delivery | Develop white papers describing the appropriate flow of critical electronic information among health care providers, including pharmacists, that protects patient privacy while providing medical information needed for decision making for optimal therapy. |
| Goal 2: Achieve integration of clinical data with electronic prescription | Engage and participate in standards-setting organizations, task forces, and work groups to improve electronic exchanges related to e-prescribing. |
| Goal 4: Ensure that HIT infrastructure includes and supports MTM services | Work with organizations defining the pharmacist’s MTM role in HIT, such as pharmacy associations, PSTAC, MTM intermediaries, and NCPDP, to ensure that MTM principles and guidelines defined by pharmacists are incorporated into the national HIT infrastructure. |
| Goal 5: Integrate pharmacist-delivered immunizations into EHR | Enhance the ability of pharmacists to electronically document, share, and evaluate patient immunization therapy. |
| Goal 6: Achieve recognition of pharmacists as meaningful users of EHR quality measures | Ensure that pharmacists are involved in the determination and adoption of the meaningful use of the EHR quality measures pertaining to medications and medication-related activities |
| Goal 9: Achieve integration of pharmacies and pharmacists into health information exchanges | Work with policymakers, including state Medicaid agencies, ONC, CMS, HHS, and other members of the health care industry, to promote the importance of pharmacist participation in HIEs |
2. National Electronic Health Information Infrastructure (HIT)

3. Pharmacy-Related HIT across the Continuum of Care for Paediatric Patients
3.1. Initiation and Generation of eRx from the Provider
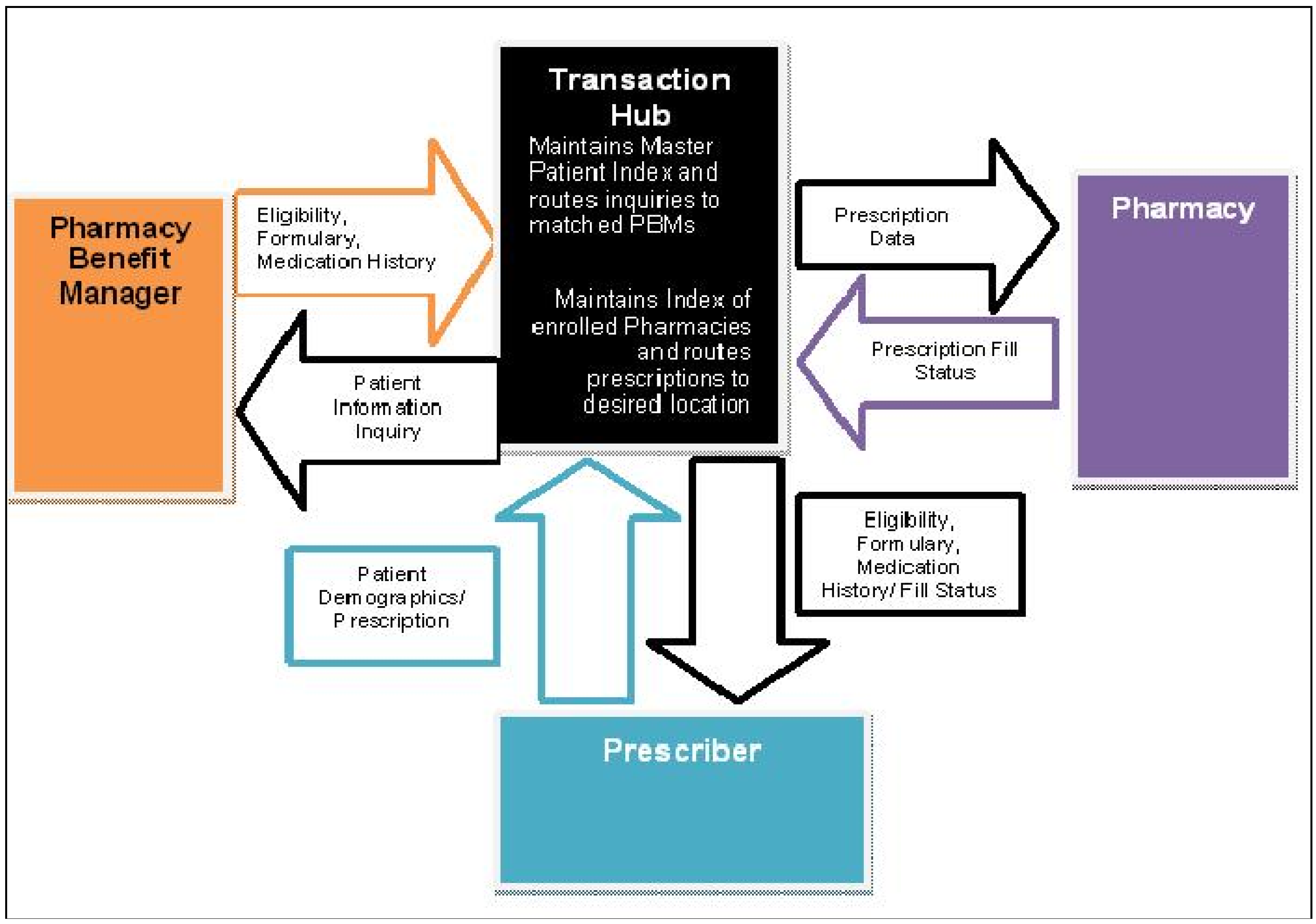
3.2. Transmission from Provider to Intermediary
3.3. Emulation at the Intermediary

3.4. Order Fulfillment at Community Pharmacy, Sub-Acute Hospital, Home Care Pharmacy, or Pharmacy Benefit Manager (PBM)
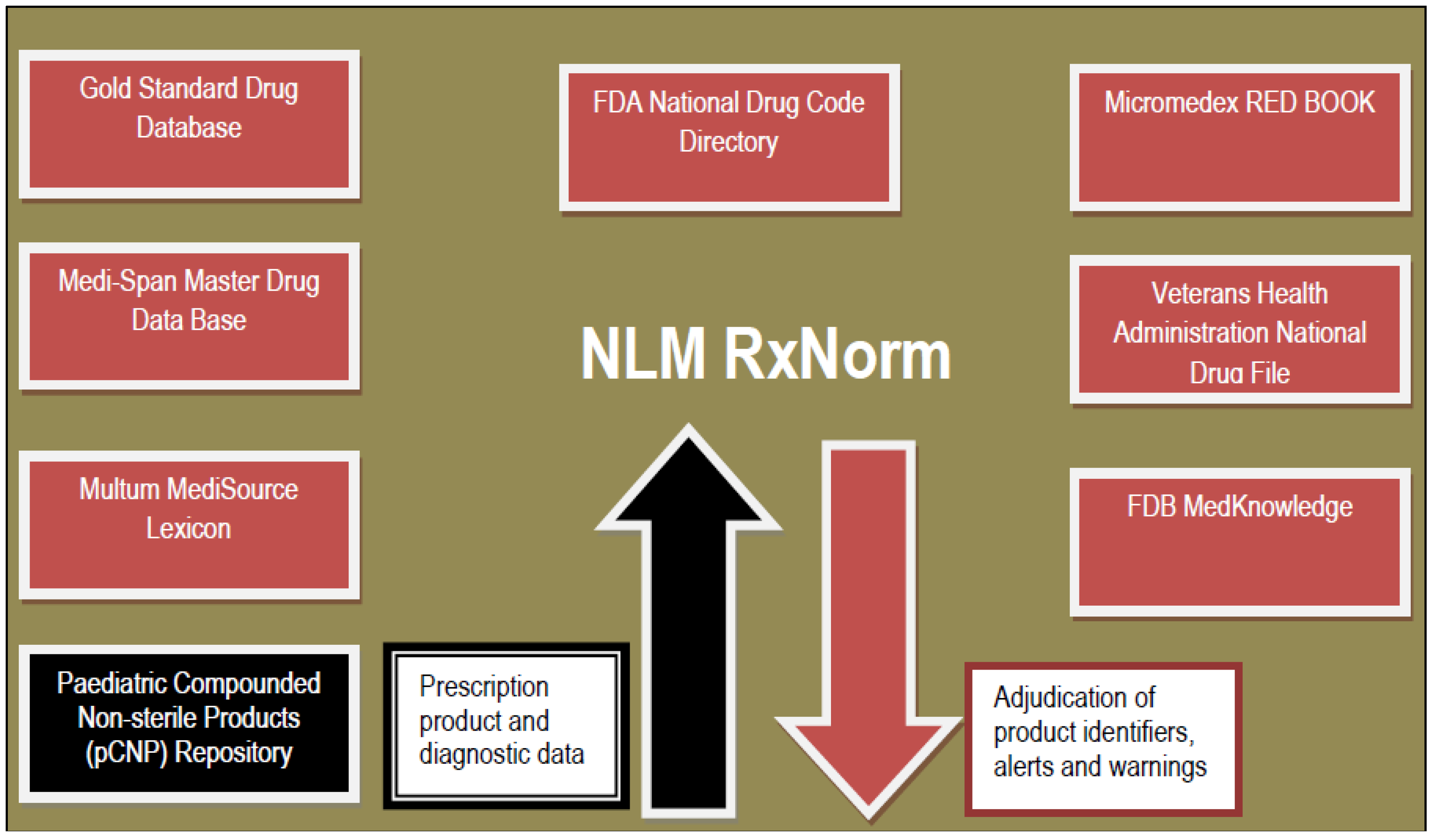
4. Where in the Infrastructure could a pCNP Repository Be Inserted?
- Ease of integration into RxNorm-formatted drug coding structures;
- Ease of maintenance and updating for new and modified extemporaneous pCNP formulations;
- Ability to emulate compatible and complete eRx transmission from initiation to fulfillment;
- Ability to facilitate bi-directional integration of clinical use data related to a minimum data set of patient assessment factors such as indication or purpose, dose-response relationships, and outcomes;
- Capability to create medication lists that would aid medication reconciliation across the continuum of care; and
- Ease of third-party adjudication for pCNP preparation and dispensing.

5. Conclusions
Conflicts of Interest
References
- Chai, G.; Governale, L.; McMahon, A.W.; Trinidad, J.P.; Staffa, J.; Murphy, D. Trends of outpatient prescription drug utilization in US children, 2002–2010. Pediatrics 2012, 130, 23–31. [Google Scholar] [CrossRef] [PubMed]
- United States Pharmacopeial Convention. <795> Pharmaceutical Compounding—Non-Sterile Preparations. In United States Pharmacopeia 38-National Formulary 33; Committee of Revision, Ed.; The United States Pharmacopeial Convention, Inc.: Rockville, MD, USA, 2015. [Google Scholar]
- Parrish, R.H., II; Cernak, I. Creating a distinct medicines-use system for children: The time is now. Pharmacy 2015, 3, 72–78. [Google Scholar]
- Benavides, S.; Madzhidova, S.; Hernandez, A.; Le, T.; Palma, S.M.; Stephen, S. Establishment of pediatric medication therapy management: A proposed model. Pharmacy 2015, 3. in press. [Google Scholar]
- Pharmacy Health Information Technology Collaborative. Roadmap for Pharmacy Health Information Technology Integration in U.S. Health Care: 2014 to 2017 Update. Available online: http://www.pharmacyhit.org/pdfs/RoadmapUpdate_2015.pdf (accessed on 16 September 2015).
- National Institute of Standards and Technology. Focused Program Competition 97–03. Information Infrastructure for Healthcare. Available online: http://www.atp.nist.gov/press/iih9703.htm (accessed on 16 September 2015).
- The Office of the National Coordinator for Health Information Technology. Adoption of Electronic Health Record Systems among U.S. Non-Federal Acute Care Hospitals: 2008–2014; Data Brief No. 23. Available online: http://www.healthit.gov/sites/default/files/data-brief/2014HospitalAdoptionDataBrief.pdf (accessed on 16 September 2015).
- The Office of the National Coordinator for Health Information Technology. Connecting Health and Care for the Nation: A Shared Nationwide Interoperability Roadmap; Draft version 1.0; pp. 135–137. Available online: http://www.healthit.gov/sites/default/files/nationwide-interoperability-roadmap-draft-version 1.0.pdf (accessed on 16 September 2015).
- Health Resources and Services Administration. Health IT Adoption Toolkit. Available online: http://www.hrsa.gov/healthit/toolbox/HealthITAdoptiontoolbox (accessed on 9 December 2015).
- Benavides, S.; Huynh, D.; Morgan, J.; Briars, L. Approach to the pediatric prescription in a community pharmacy. J. Pediatr. Pharmacol. Ther. 2011, 16, 298–307. [Google Scholar] [PubMed]
- Parrish, R.H., II; Benavides, S.; Malak, J.T.; Potts, A.L.; Guirguis, M.; Hagemann, T. Optimizing effectiveness in electronic prescriptions for pediatric outpatients: A call for responsive action. Pharmacy 2014, 2, 260–269. [Google Scholar]
- Bhatt-Mehta, V.; MacArthur, R.B.; Löbenberg, R.; Cies, J.J.; Cernak, I.; Parrish, R.H., II. An algorithm that identifies compounded non-sterile products that can be formulated on a commercial scale or imported to promote safer medication use in children. Pharmacy 2015, 3, 284–294. [Google Scholar] [CrossRef]
- Ventola, C.L. Mobile devices and apps for healthcare professionals: Uses and benefits. P&T 2014, 39, 356–364. [Google Scholar]
- Agarwal, R.; Angst, C.M.; DesRoches, C.M.; Fischer, M.A. Technological viewpoints (frames) about electronic prescribing in physician practices. J. Am. Med. Inform. Assoc. 2010, 17, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Stultz, J.S.; Nahata, M.C. Appropriateness of commercially available and partially customized medication dosing alerts among pediatric patients. J. Am. Med. Inform. Assoc. 2014, 21, e35–e42. [Google Scholar] [CrossRef] [PubMed]
- Pederson, C.A.; Schneider, P.J.; Scheckelhoff, D.J. ASHP national survey of pharmacy practice in hospital settings: Prescribing and transcribing-2013. Am. J. Health Syst. Pharm. 2014, 71, 924–942. [Google Scholar] [CrossRef] [PubMed]
- Gracy, D.; Weisman, J.; Grant, R.; Pruitt, J.; Brito, A. Content Barriers to Pediatric Uptake of Electronic Health Records. In Advances in Pediatrics; Kappy, M.S., Barness, L.A., Barton, L.L., Berkowitz, C.D., Gilbert-Barness, E., Ziegler, M., Eds.; Volume 59, Elsevier Health Sciences: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Slight, S.P.; Berner, E.S.; Galanter, W.; Huff, S.; Lambert, B.L.; Lannon, C.; Lehmann, C.U.; McCourt, B.J.; McNamara, M.; Menachemi, N.; et al. Meaningful use of electronic health records: Experiences from the field and future opportunities. JMIR Med. Inform. 2015, 3, e30. Available online: http://medinform.jmir.org/2015/3/e30/ (accessed on 16 September 2015). [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caruso, M.C.; Gittleman, M.A.; Widecan, M.L.; Luria, J.W. Pediatric emergency department discharge prescriptions requiring pharmacy clarification. Pediatr Emerg. Care 2015, 31, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Palchuk, M.B.; Fang, E.A.; Cygielnik, J.M.; Lebreche, M.; Shubina, M.; Ramelson, H.Z.; Hamann, C.; Broverman, C.; Einbinder, J.S.; Turchin, A. An unintended consequence of electronic prescriptions: Prevalence and impact of internal discrepancies. J. Am. Med. Inform. Assoc. 2010, 17, 472–476. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Mahoney, L.M.; Shakurova, A.; Goss, F.; Chang, F.Y.; Bates, D.W.; Rocha, R.A. How many medication orders are entered through free-text in EHRs?—A study on hypoglycemic agents. AMIA Annu. Symp. Proc. 2012, 2012, 1079–1088. [Google Scholar] [PubMed]
- Dhavle, A.; Rupp, M.T. Towards creating the perfect electronic prescription. J. Am. Med. Inform. Assoc. 2014, 22, e7–e12. [Google Scholar] [CrossRef] [PubMed]
- NextGen Healthcare; (Marketing Department, Philadelphia, PA, USA). Personal communication, 20 October 2015.
- National Council of Prescription Drug Programs. NCPDP Electronic Prescribing Standards. September 2014. Available online: http://www.ncpdp.org/NCPDP/media/pdf/NCPDPEprescribing101.pdf (accessed on 23 September 2015).
- The Office of the National Coordinator for Health IT. 2016 Interoperability Standards Advisory (draft). 22 September 2015. Available online: http://www.healthit.gov/sites/default/files/2016_InteroperabilityStandardsAdvisoryFINAL.pdf (accessed on 23 September 2015). [Google Scholar]
- Bodenreider, O.; Rodriguez, L.M. Analyzing U.S. prescription lists with RxNorm and the ATC/DDD index. AMIA Annu. Symp. Proc. 2014, 2014, 297–306. [Google Scholar] [PubMed]
- Bell, D.S.; O’Neill, S.M.; Reynolds, K.A.; Schoeff, D. Evaluation of RxNorm in Ambulatory Electronic Prescribing; Rand Corporation: Santa Monica, CA, USA, 2011; Available online: http://www.rand.org/content/dam/rand/pubs/technical_reports/2011/RAND_TR941.pdf (accessed on 23 September 2015).
- United States Pharmacopeial Convention, Inc. 2015 USP Compounding Compendium; United States Pharmacopeial Convention: Rockville, MD, USA, 2015. [Google Scholar]
- U.S. National Library of Medicine; Unified Medical Language System (UMLS). RxNorm Technical Documentation. Available online: https://www.nlm.nih.gov/research/umls/rxnorm/docs/2012/rxnorm_doco_full_2012-3.html (accessed on 23 September 2015).
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parrish, II, R.H. Positioning a Paediatric Compounded Non-Sterile Product Electronic Repository (pCNPeRx) within the Health Information Technology Infrastructure. Pharmacy 2016, 4, 2. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy4010002
Parrish, II RH. Positioning a Paediatric Compounded Non-Sterile Product Electronic Repository (pCNPeRx) within the Health Information Technology Infrastructure. Pharmacy. 2016; 4(1):2. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy4010002
Chicago/Turabian StyleParrish, II, Richard H. 2016. "Positioning a Paediatric Compounded Non-Sterile Product Electronic Repository (pCNPeRx) within the Health Information Technology Infrastructure" Pharmacy 4, no. 1: 2. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy4010002