Clinical Effectiveness of Bulk-Fill and Conventional Resin Composite Restorations: Systematic Review and Meta-Analysis

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Study Quality Assessment
2.4. Assessment of the Risk of Bias of the Studies
2.5. Analysis of Results
3. Results
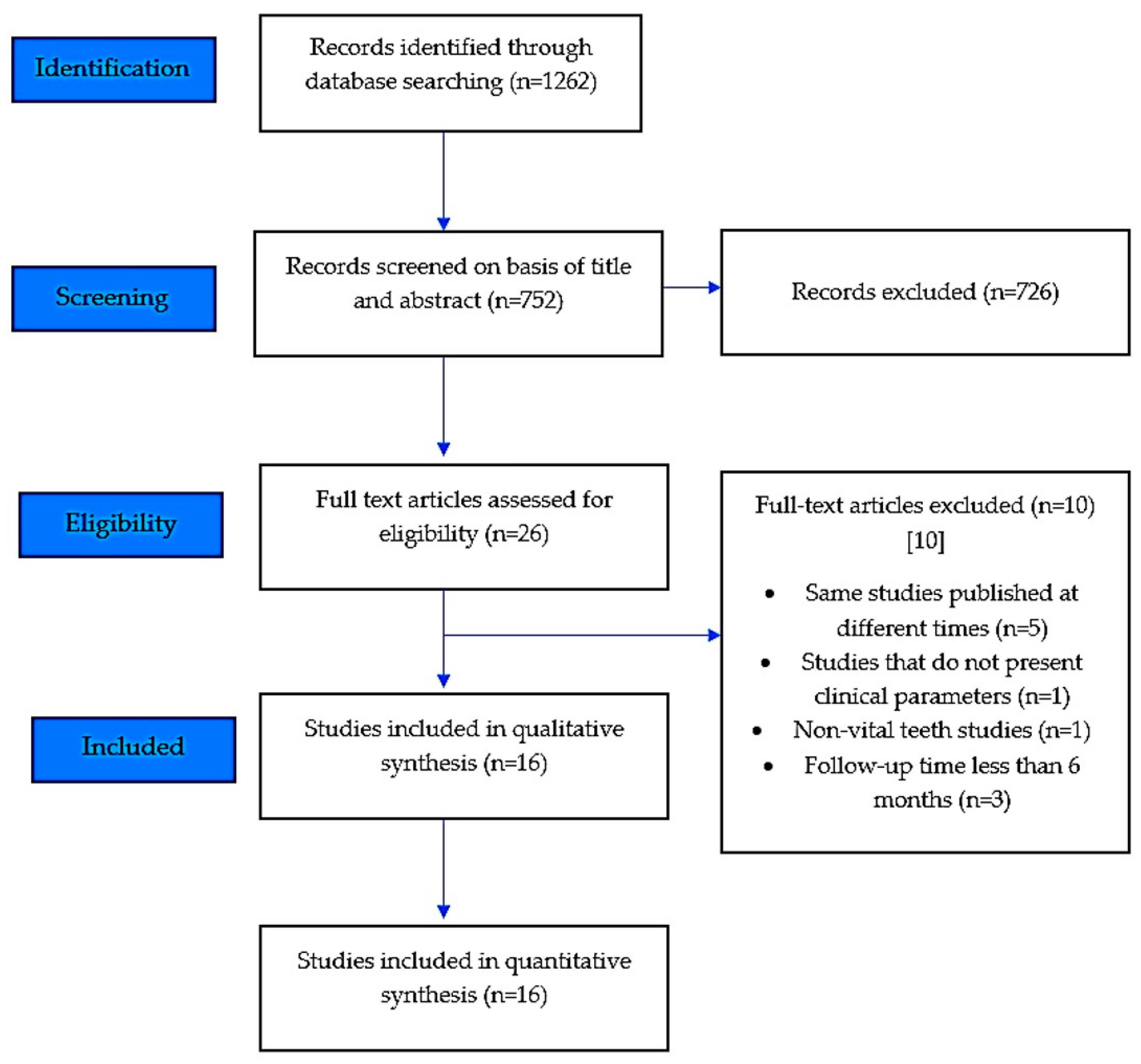
3.1. Selection of Studies
3.2. Characteristics of the Studies
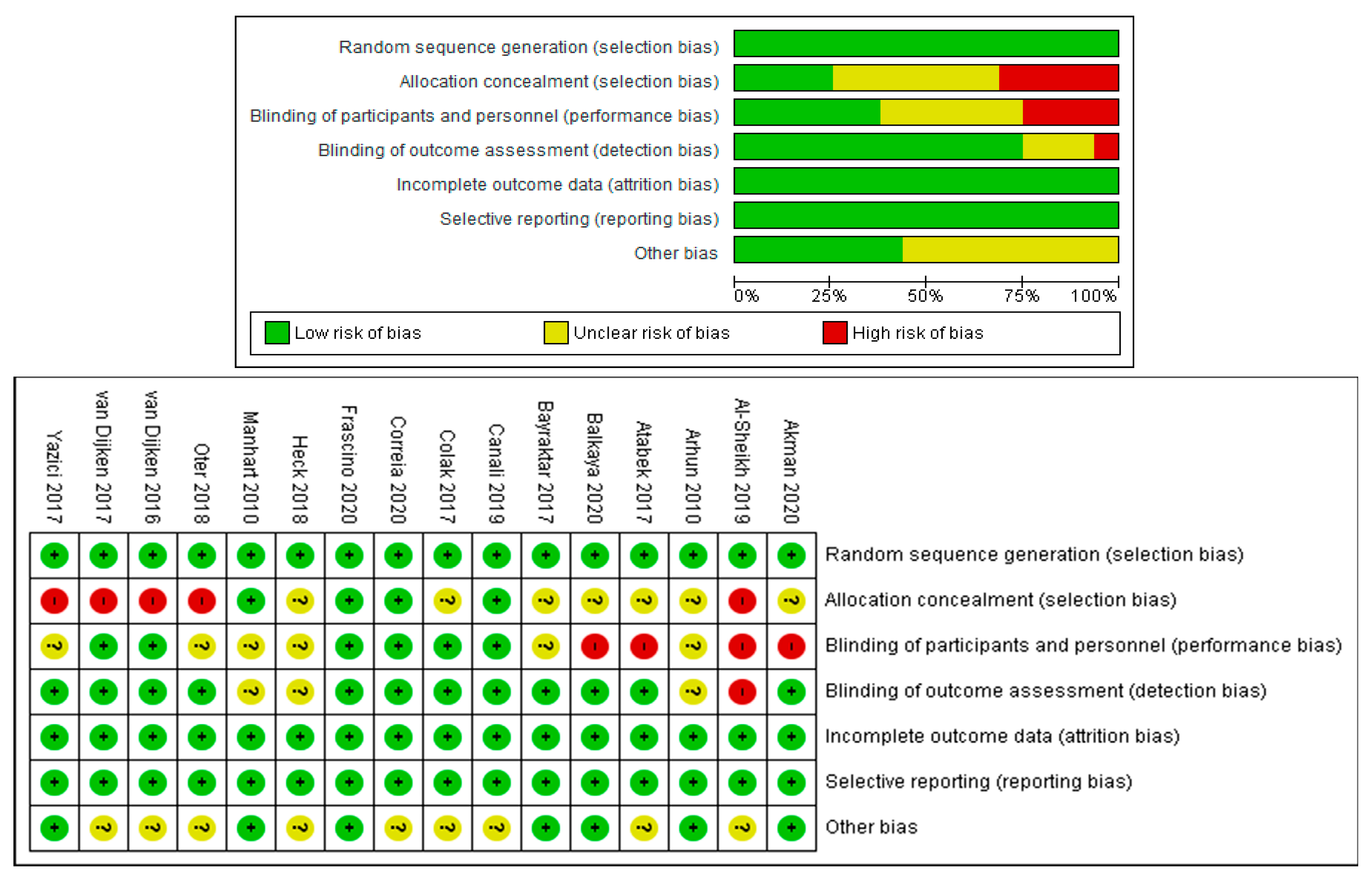
3.3. Analysis of Risk of Bias of the Studies
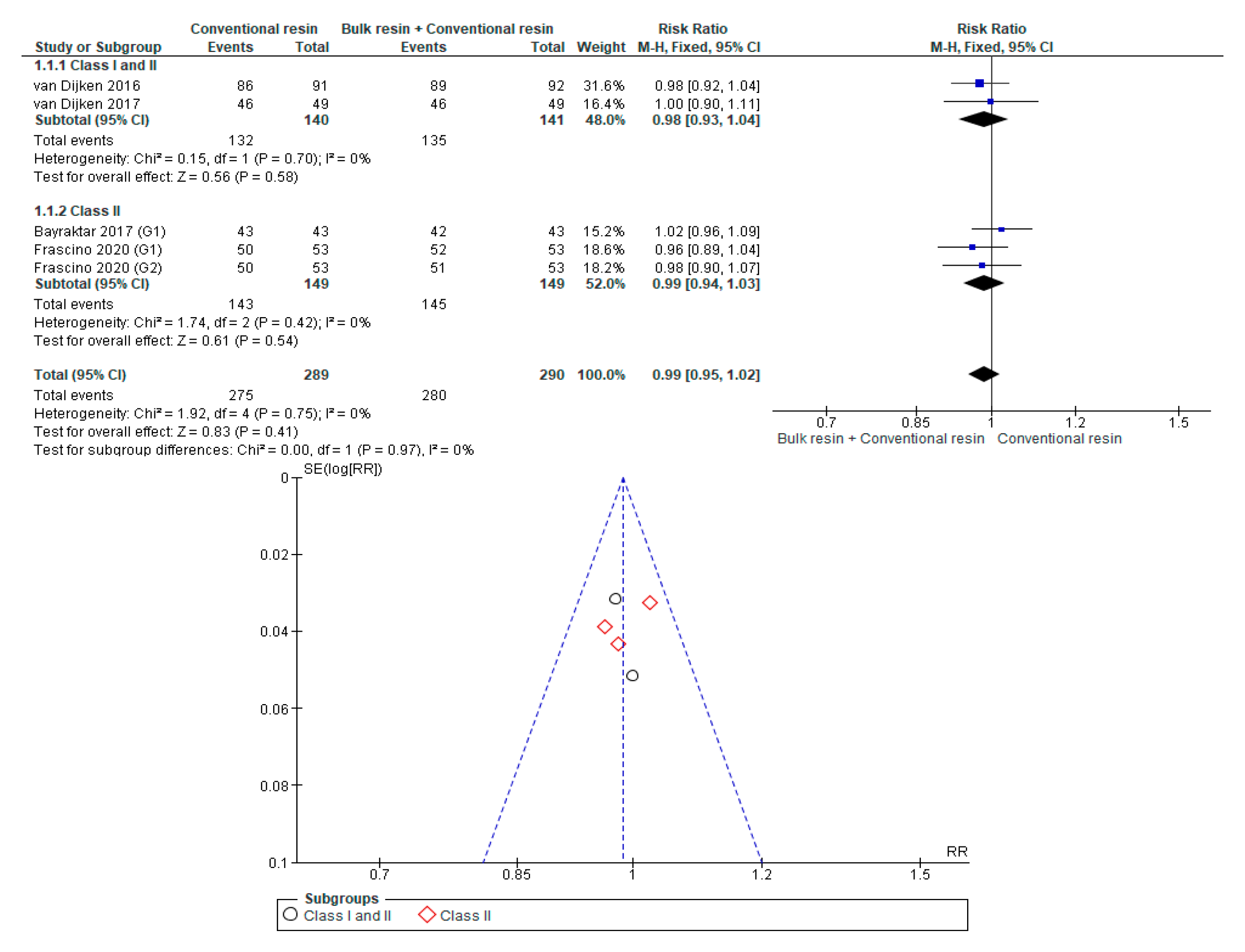
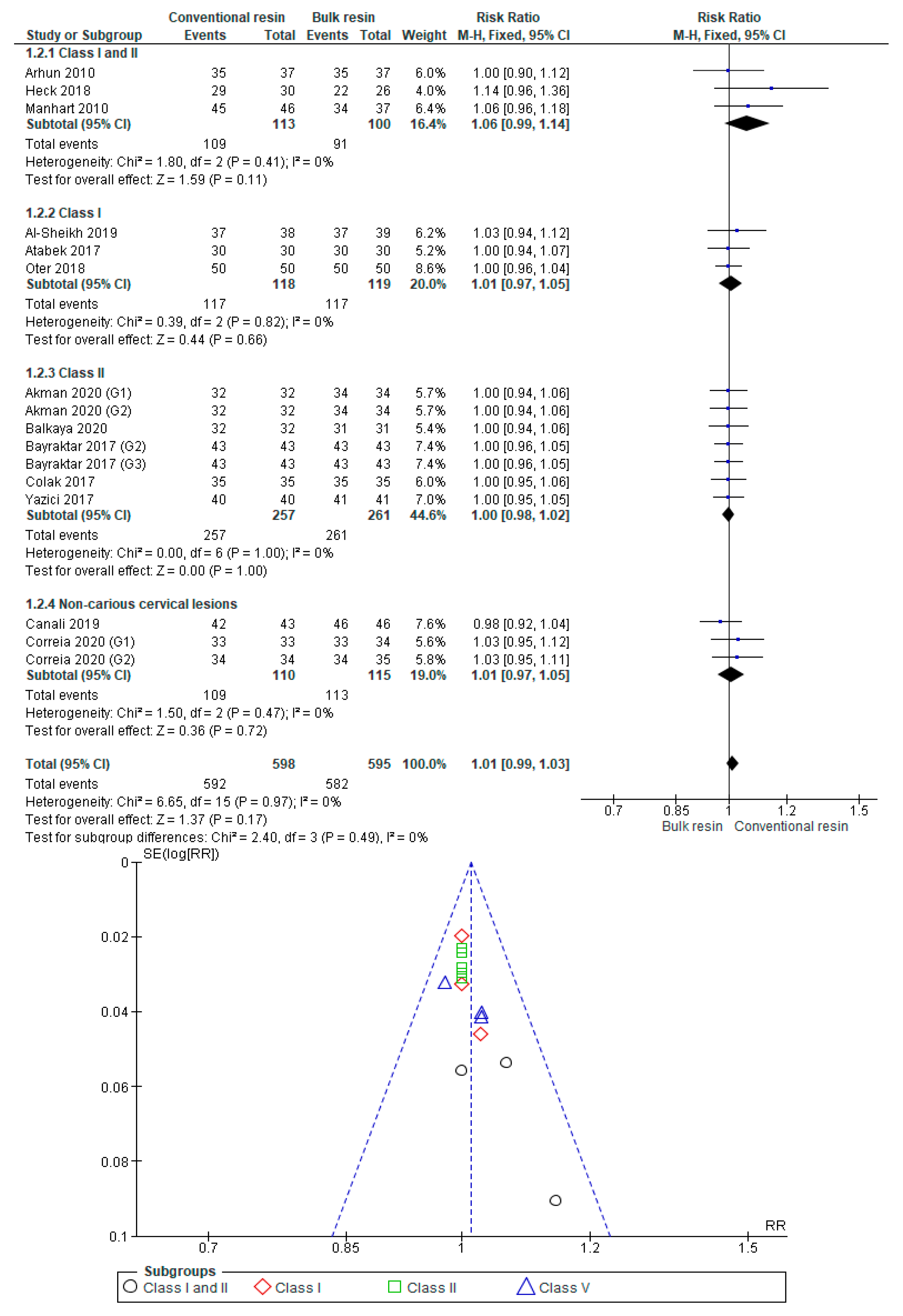
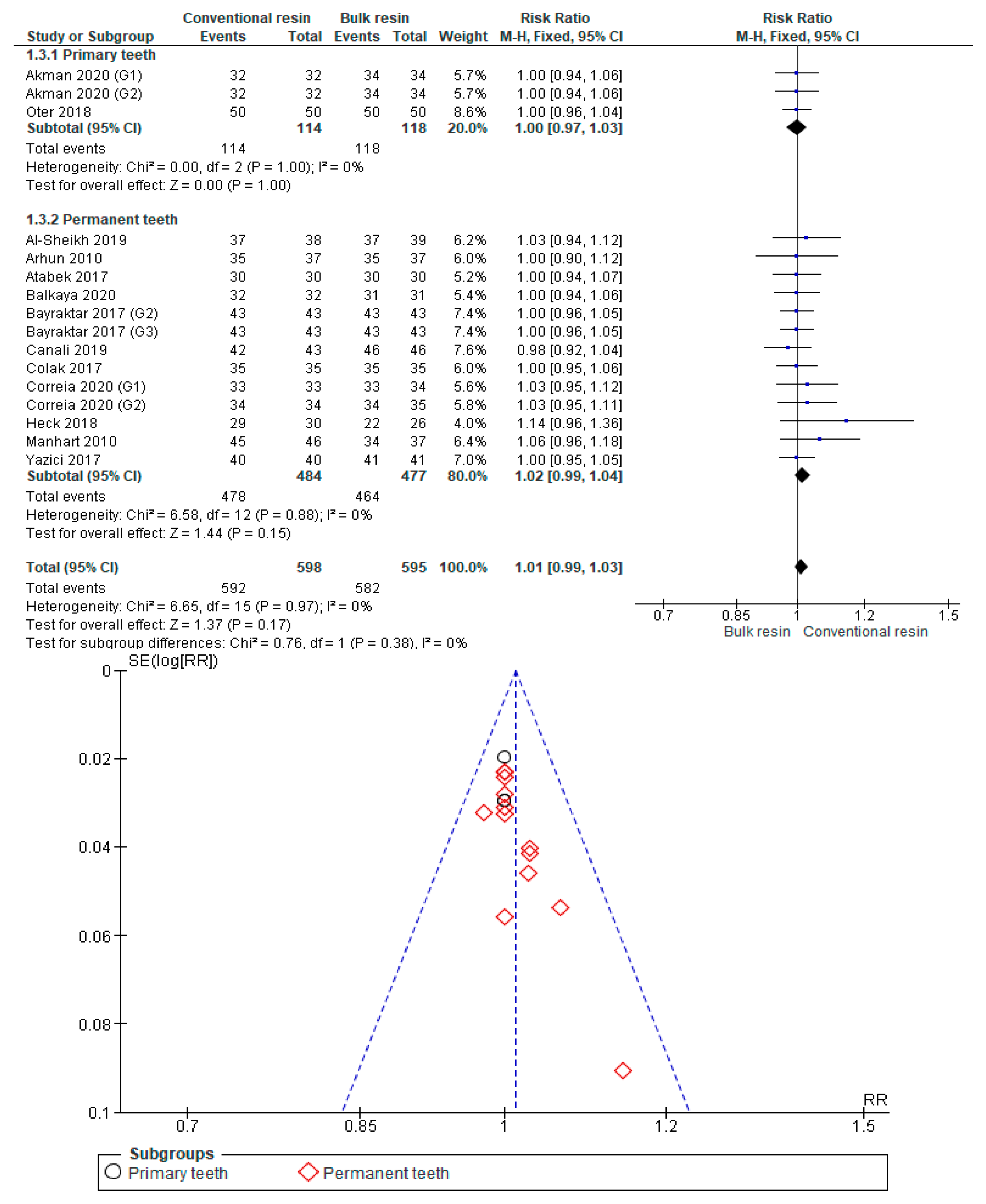
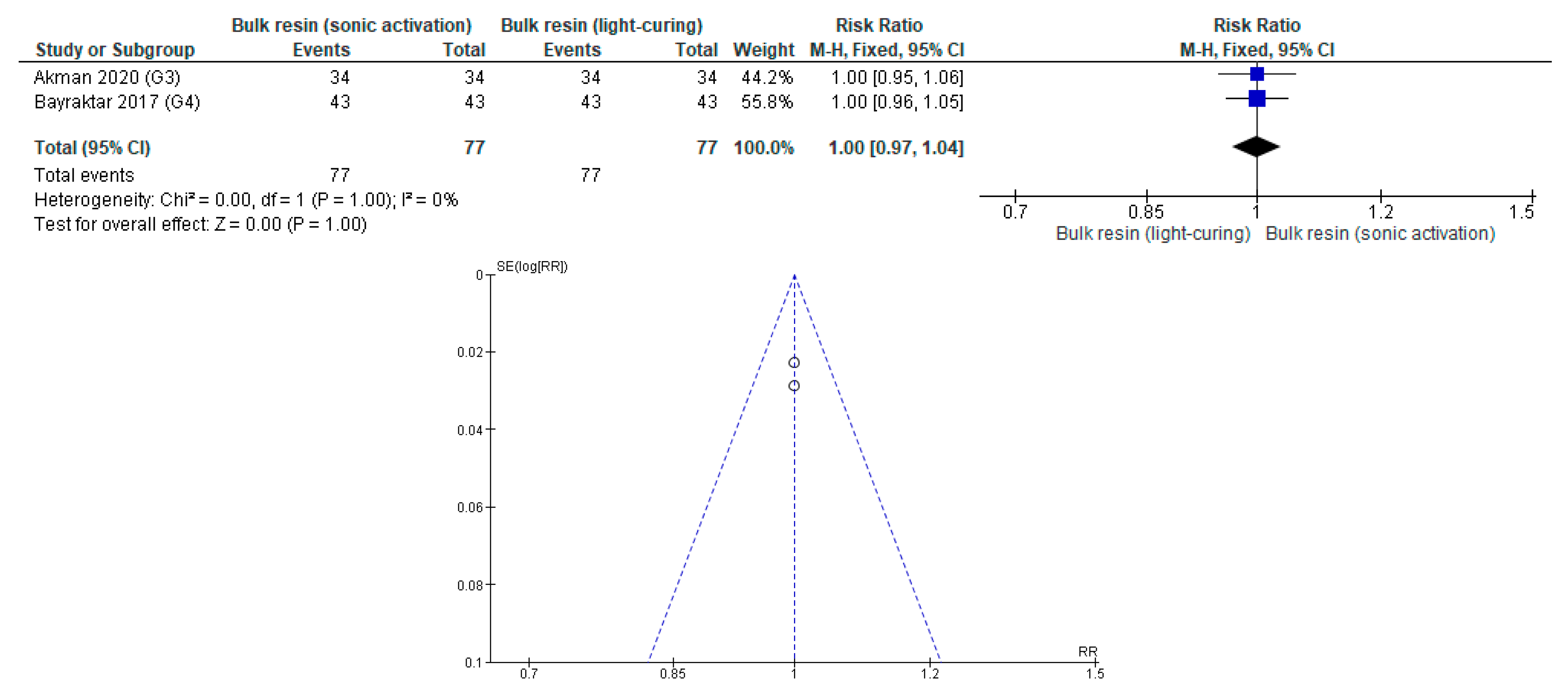
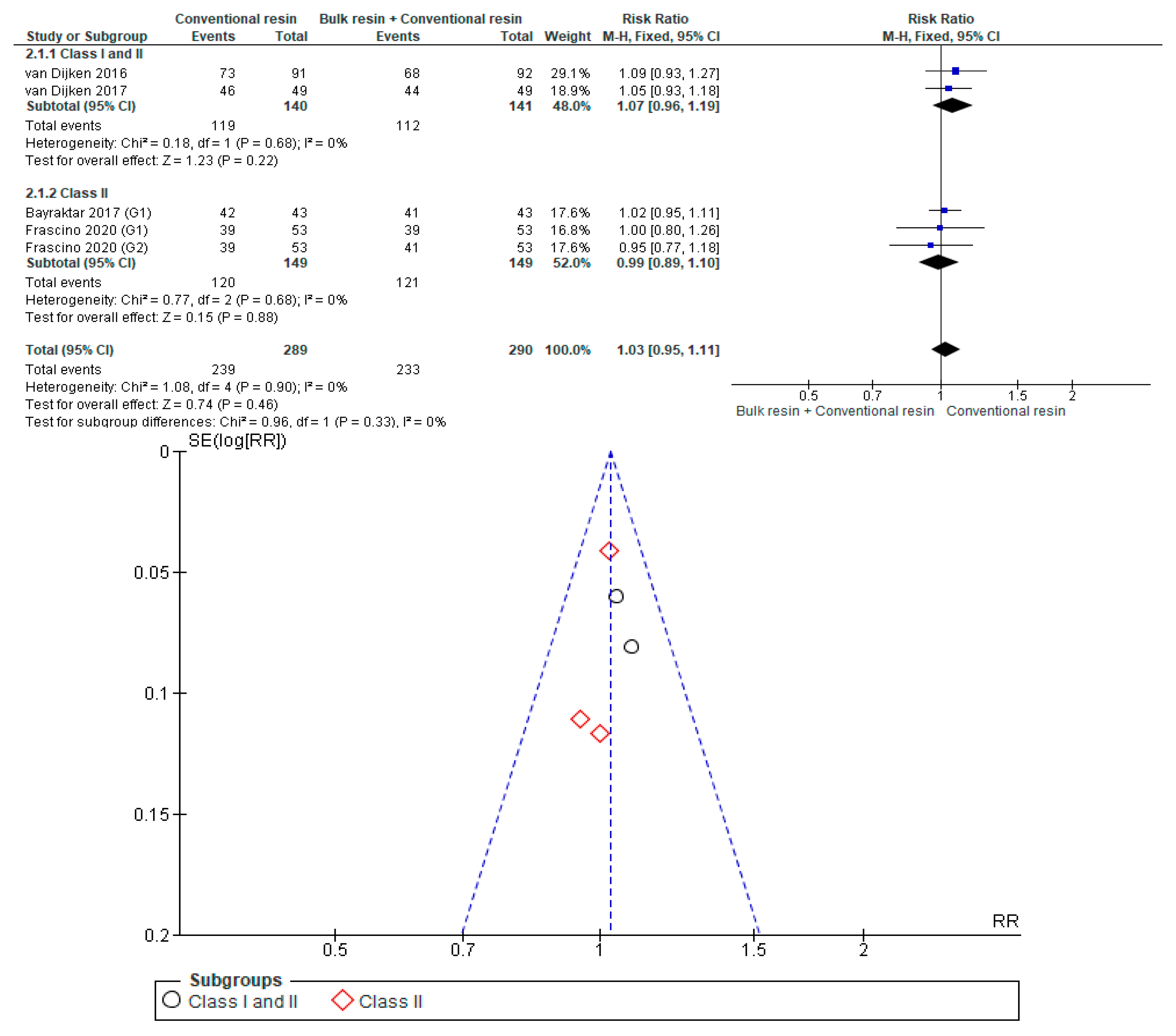
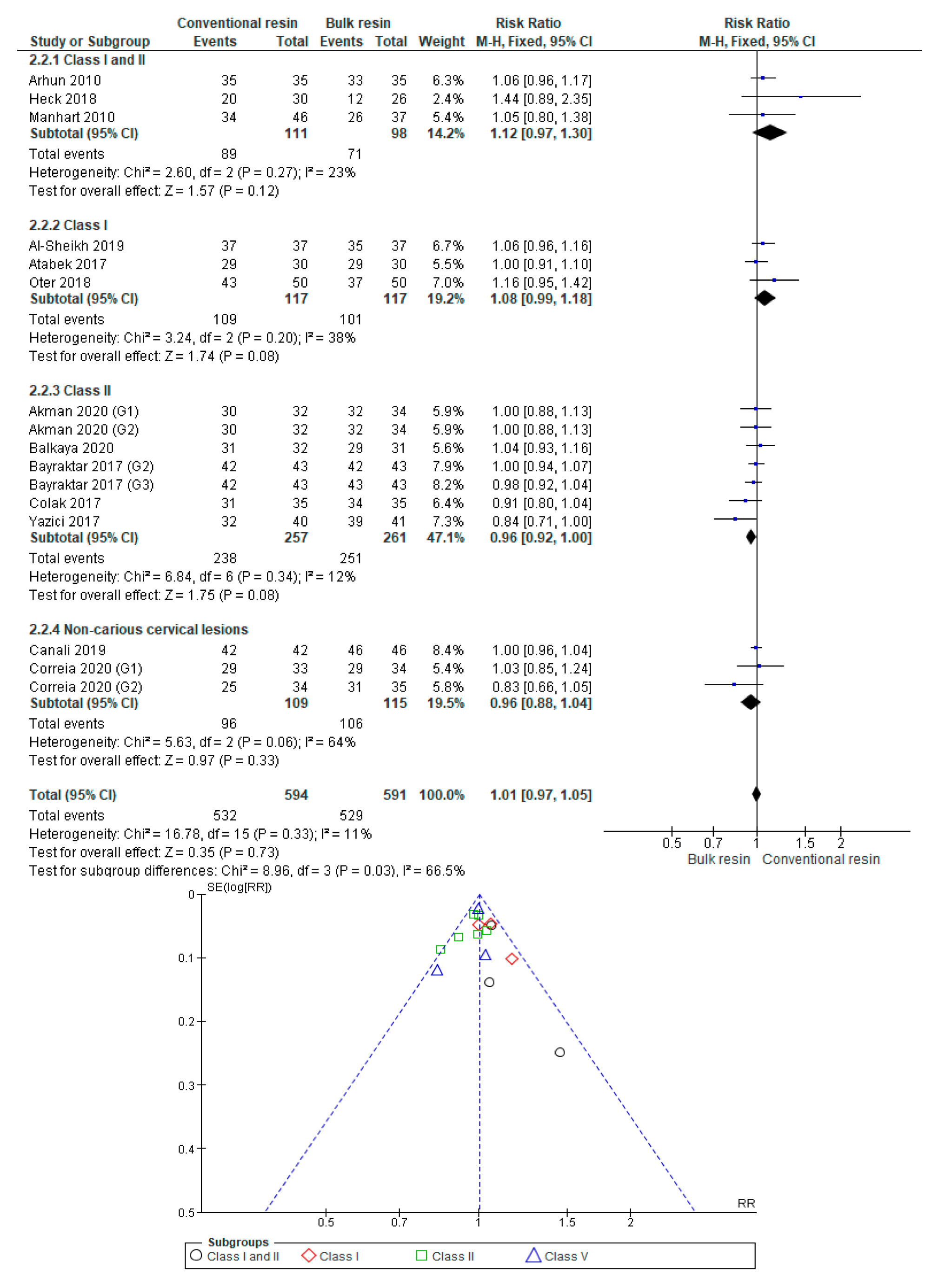
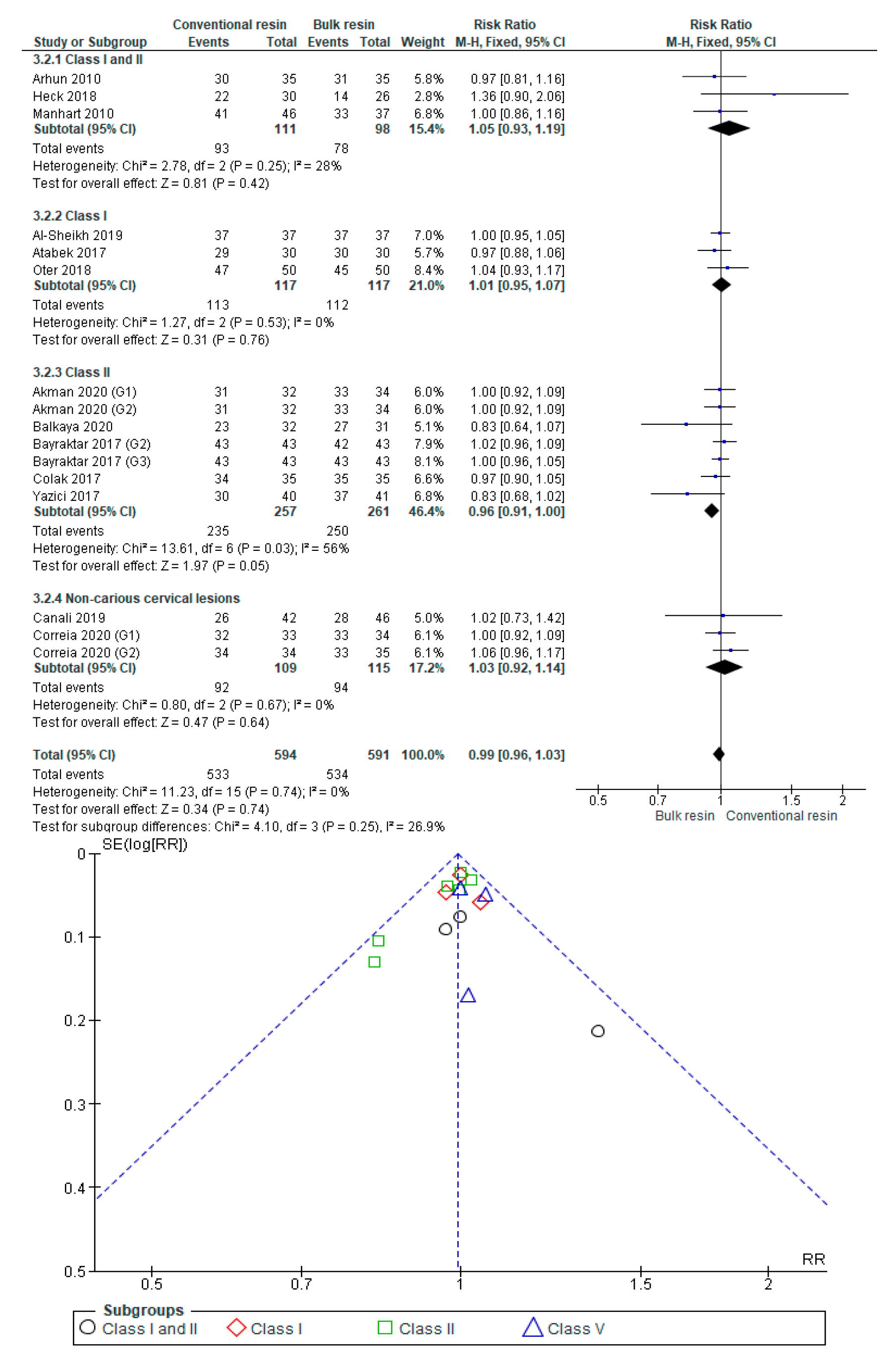
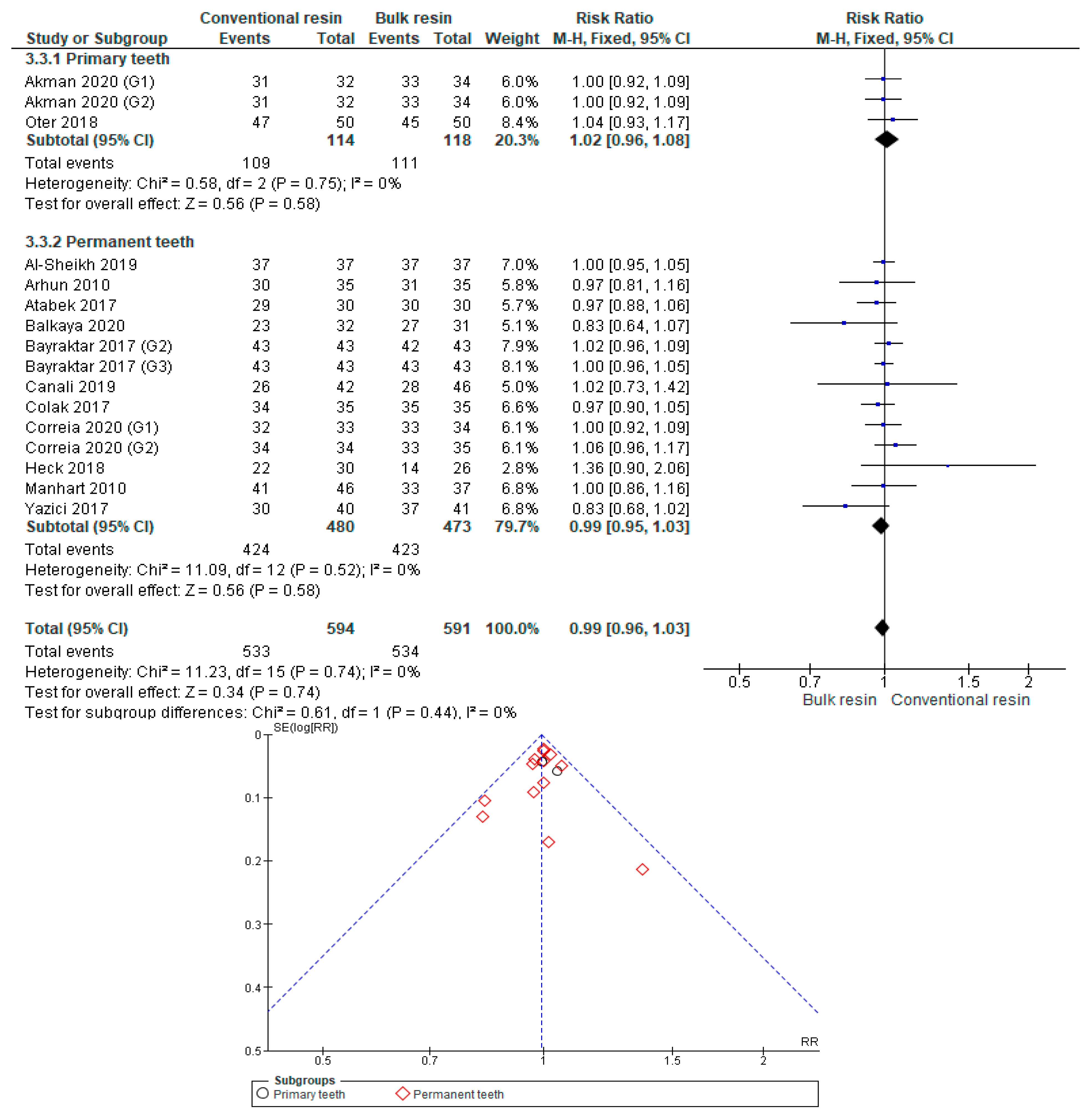
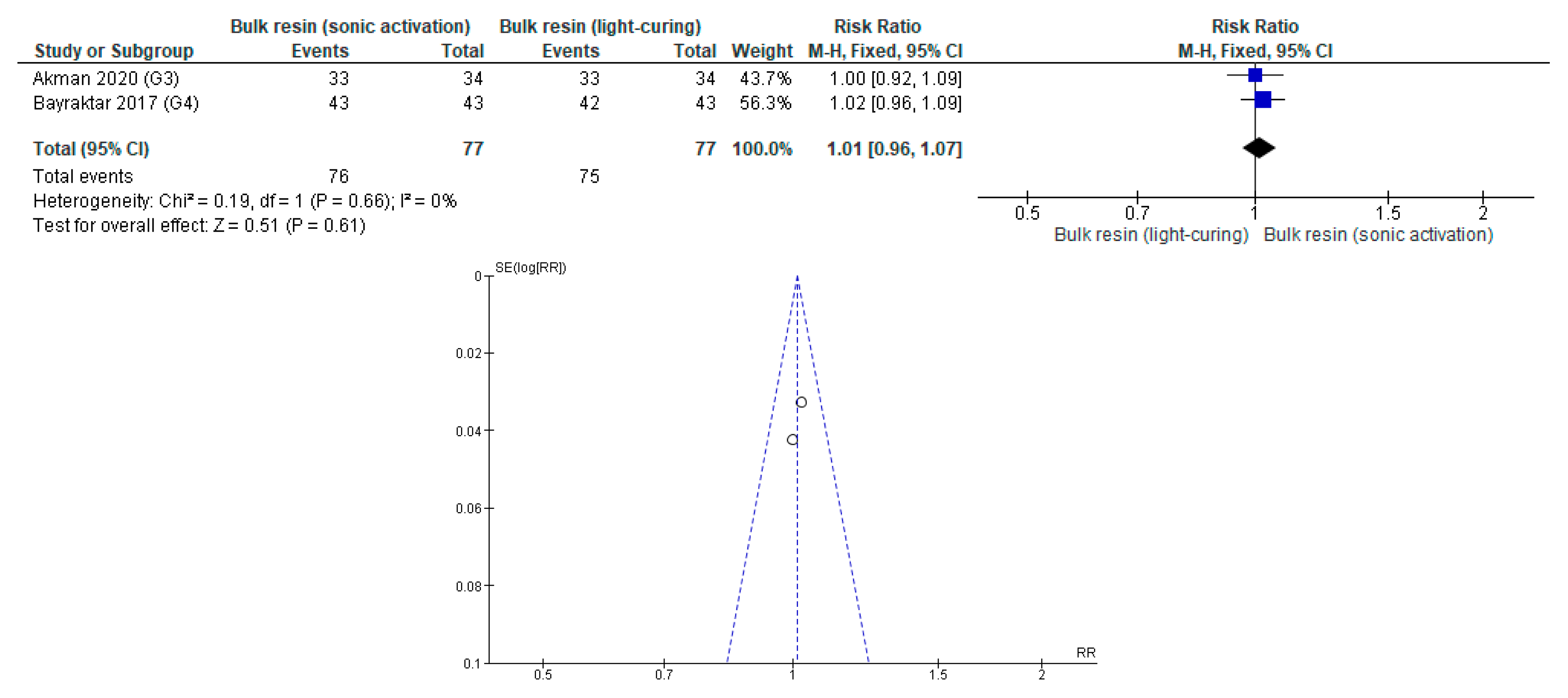
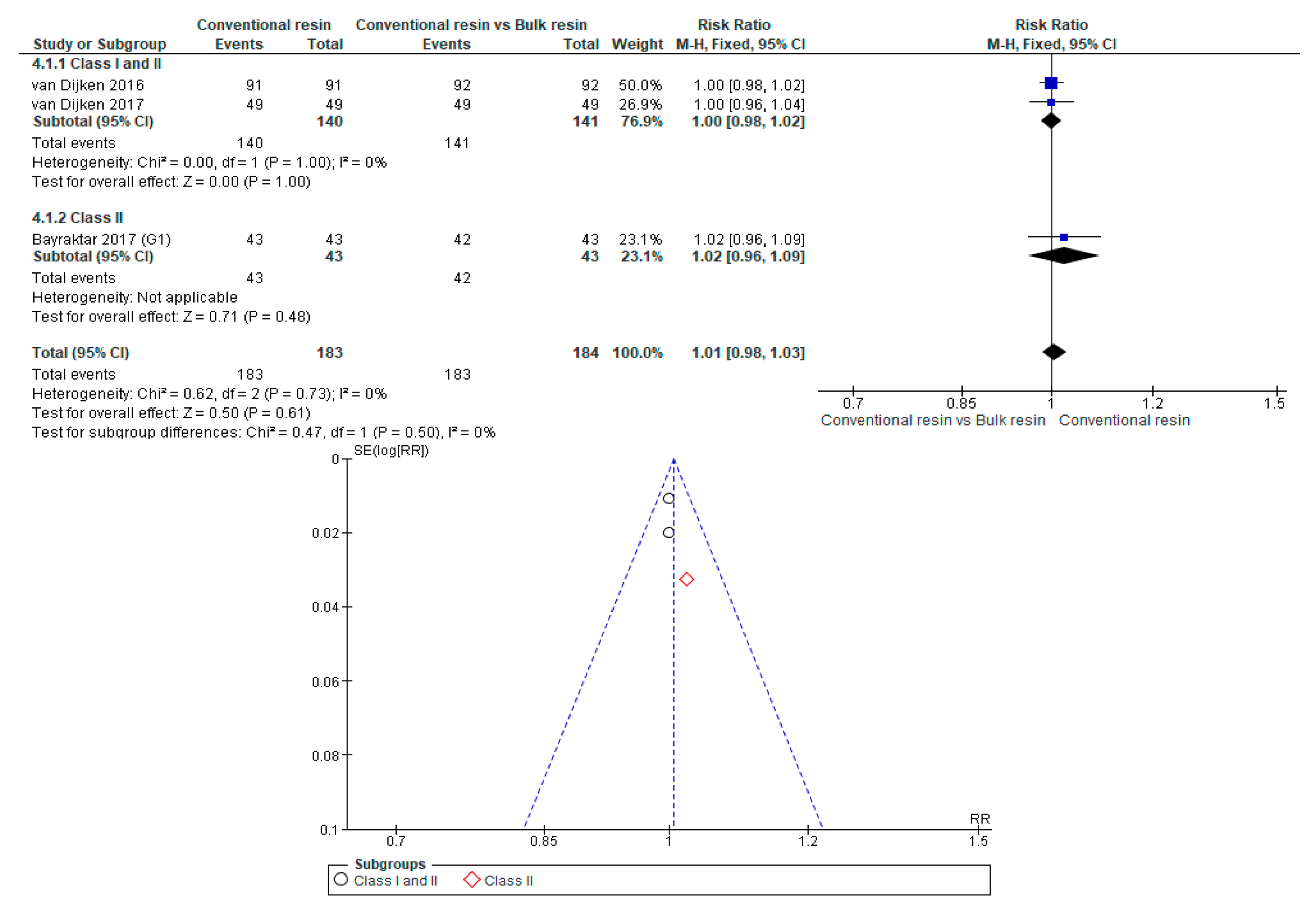
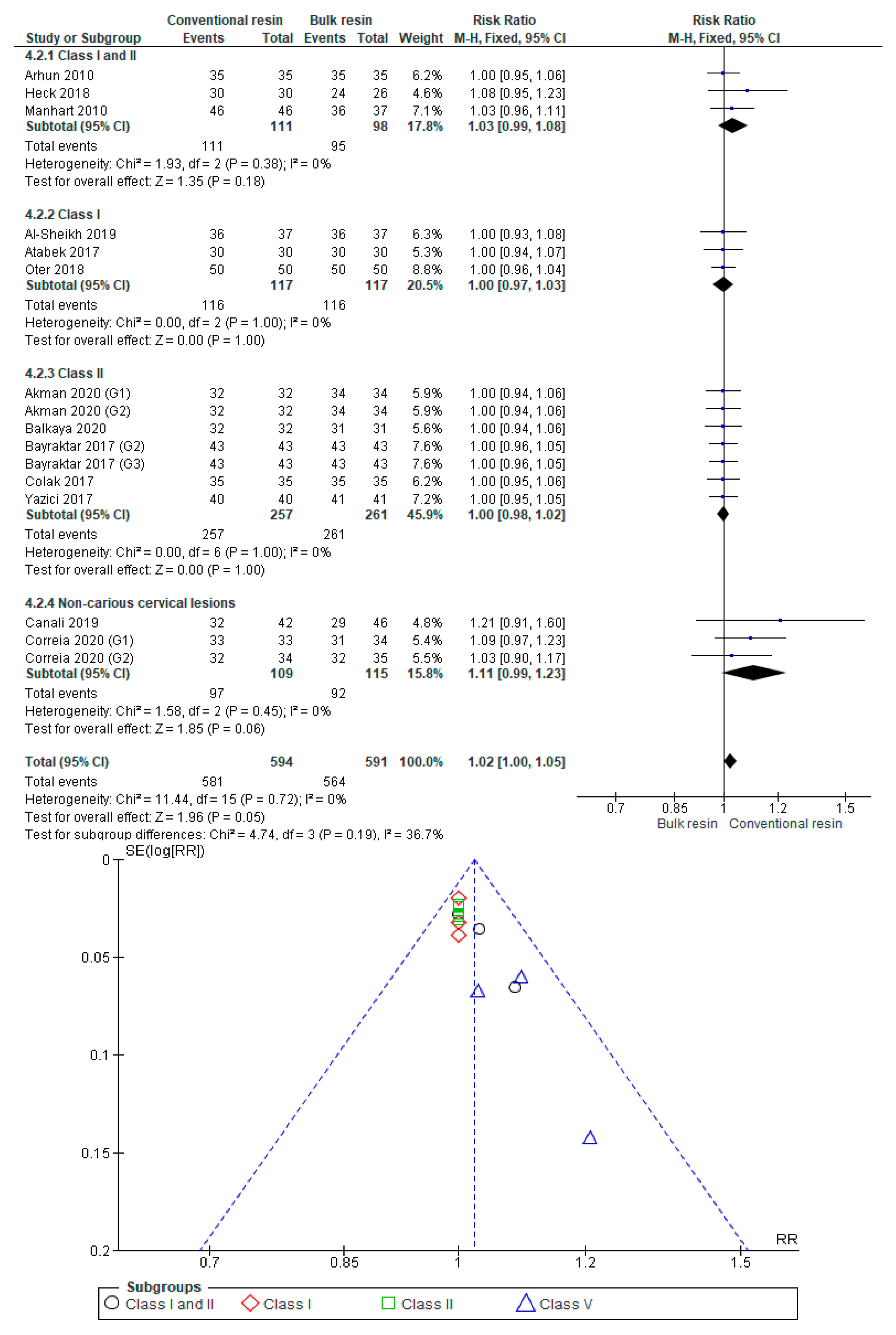
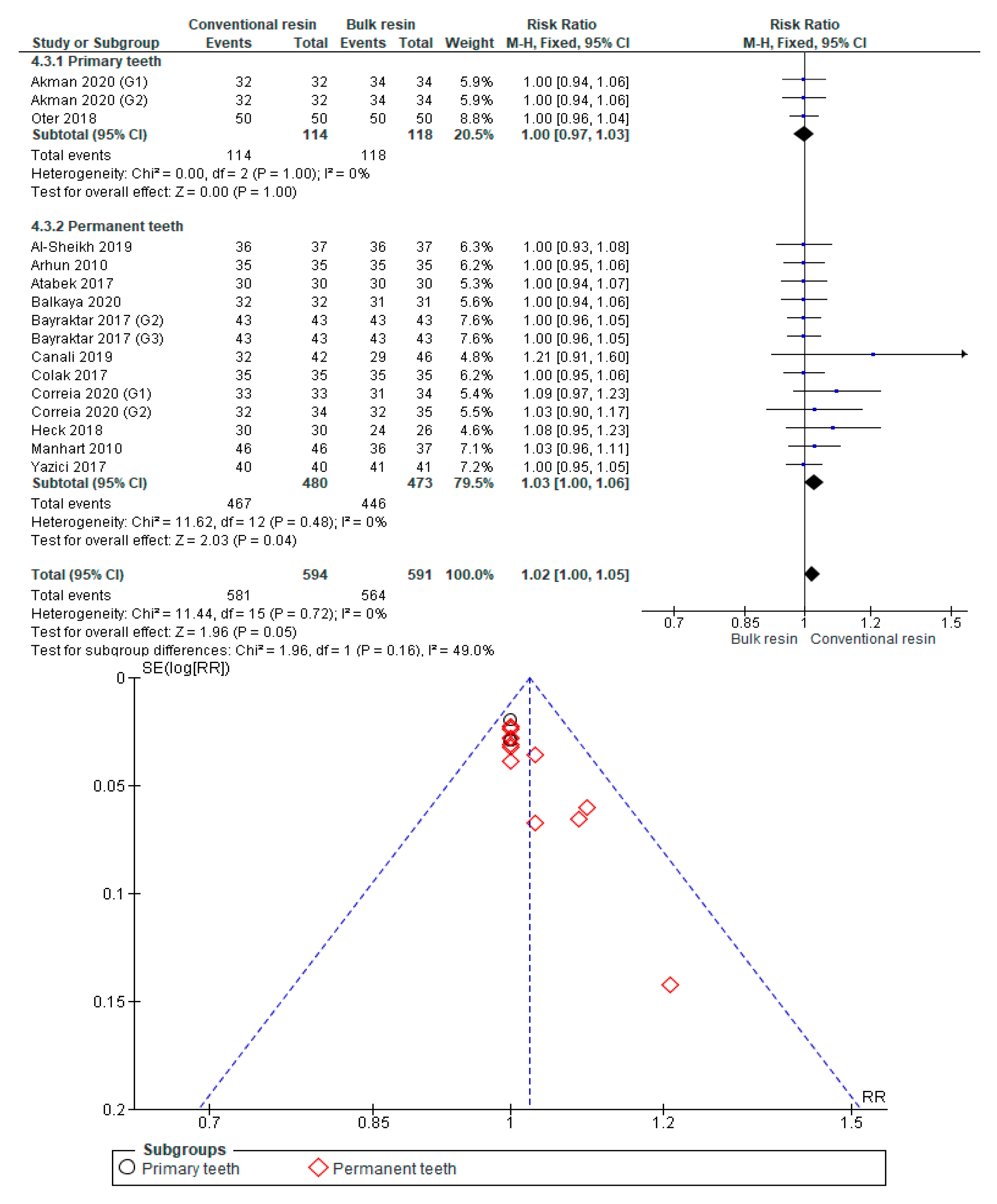
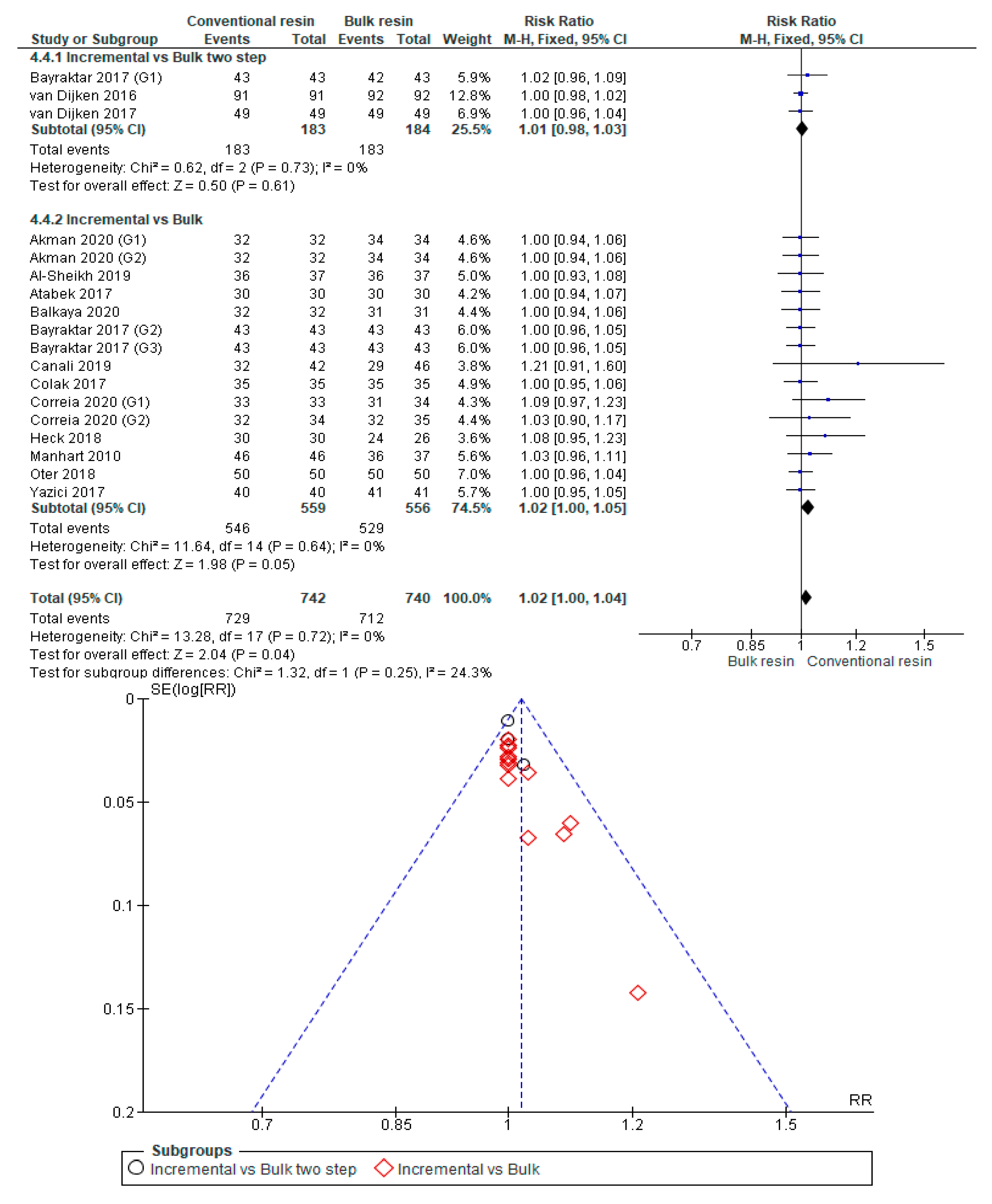
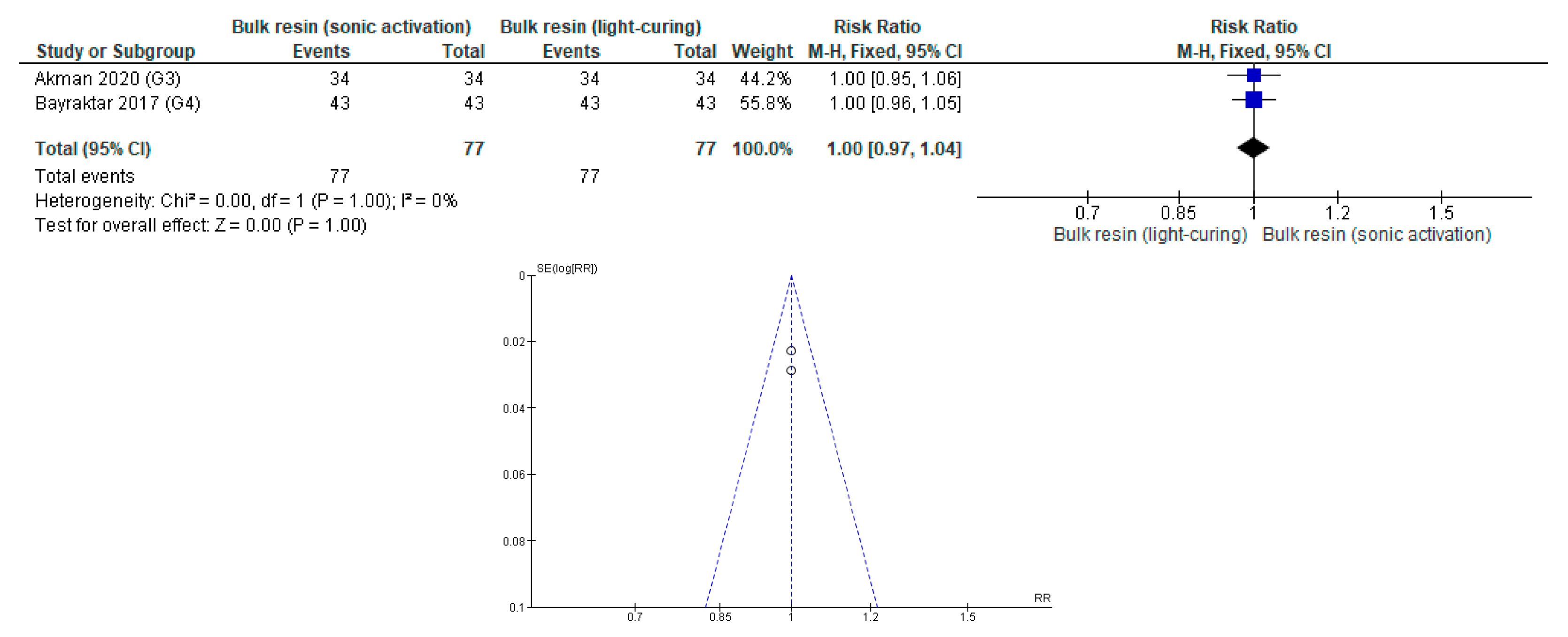
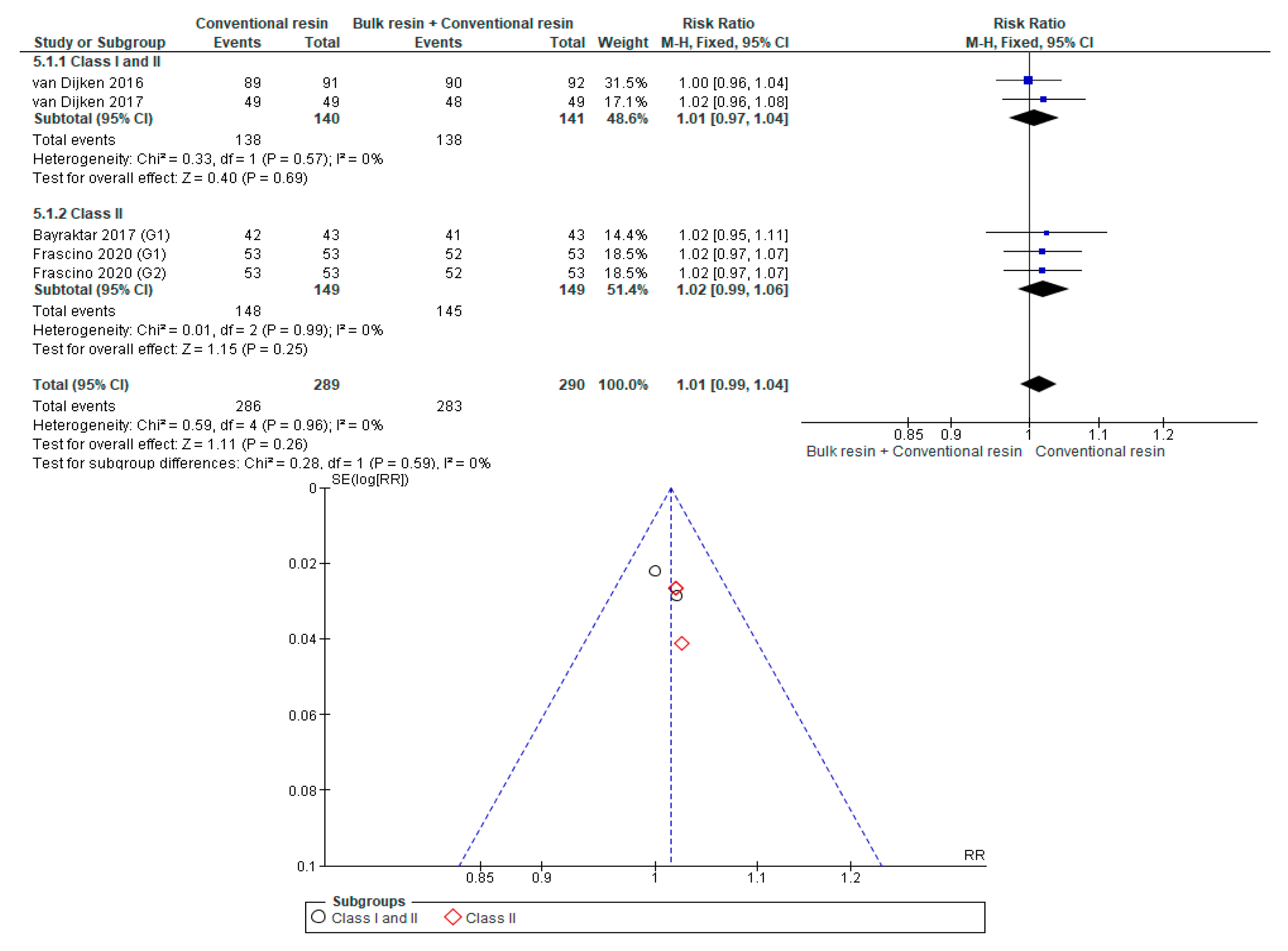
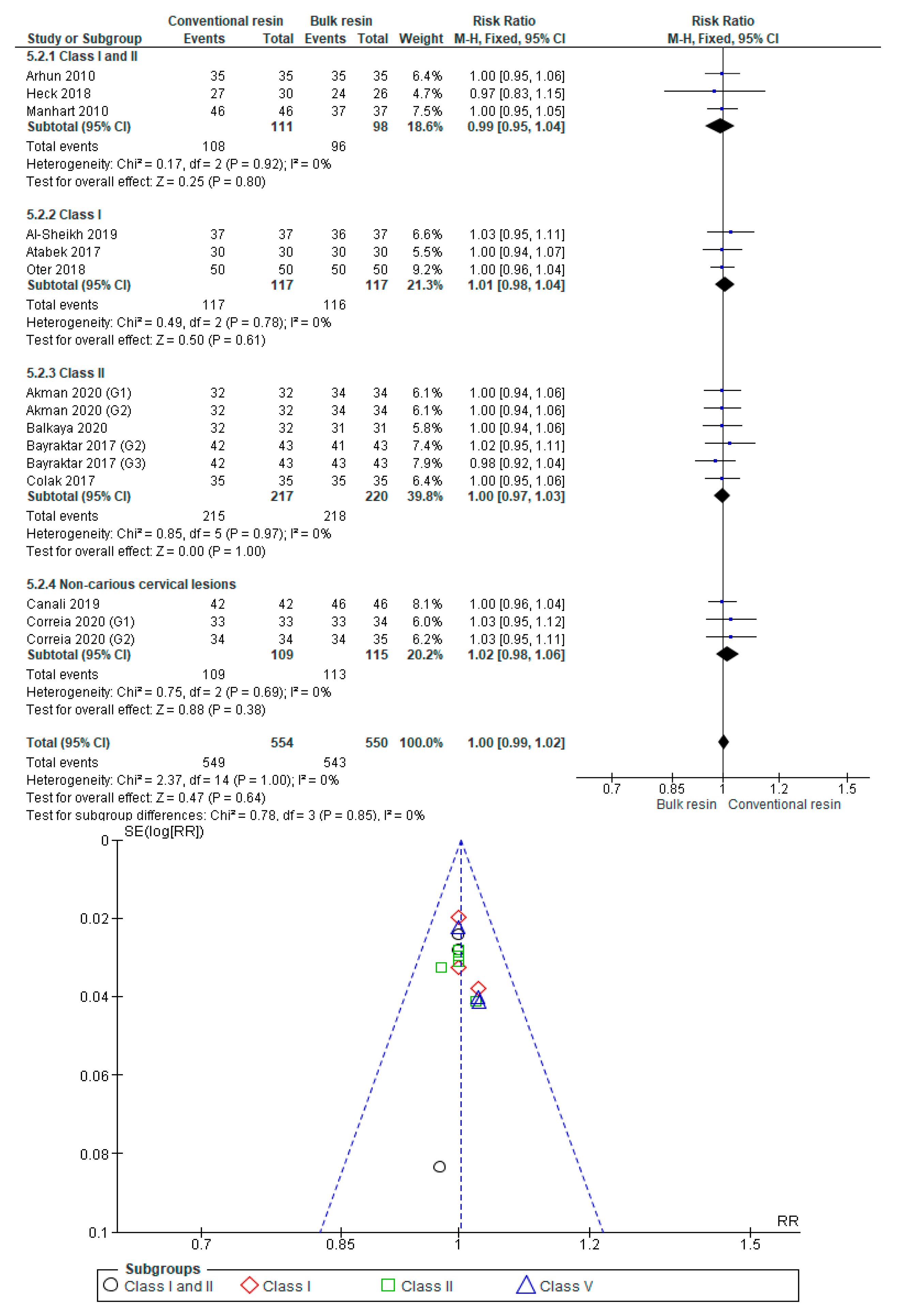
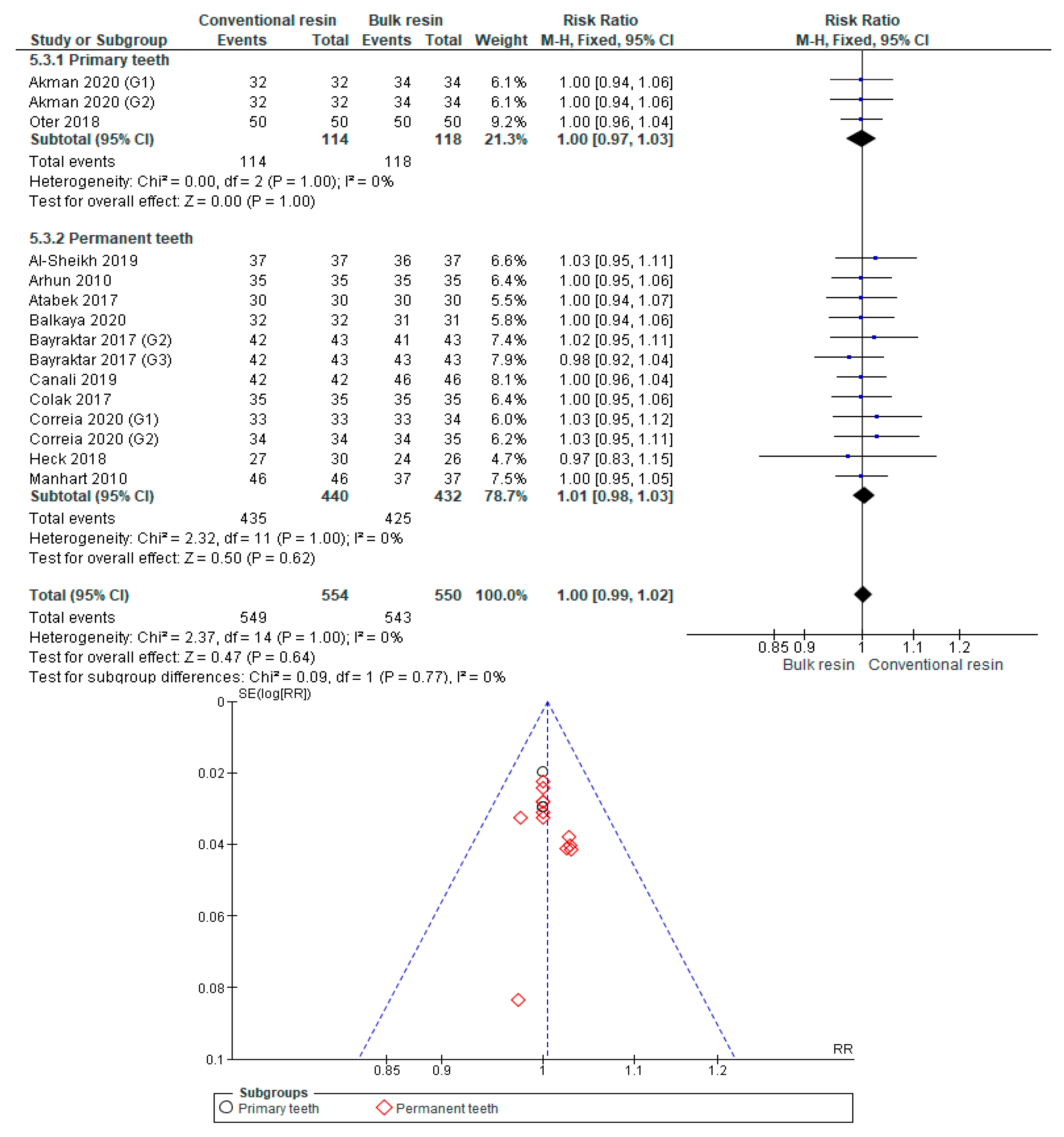
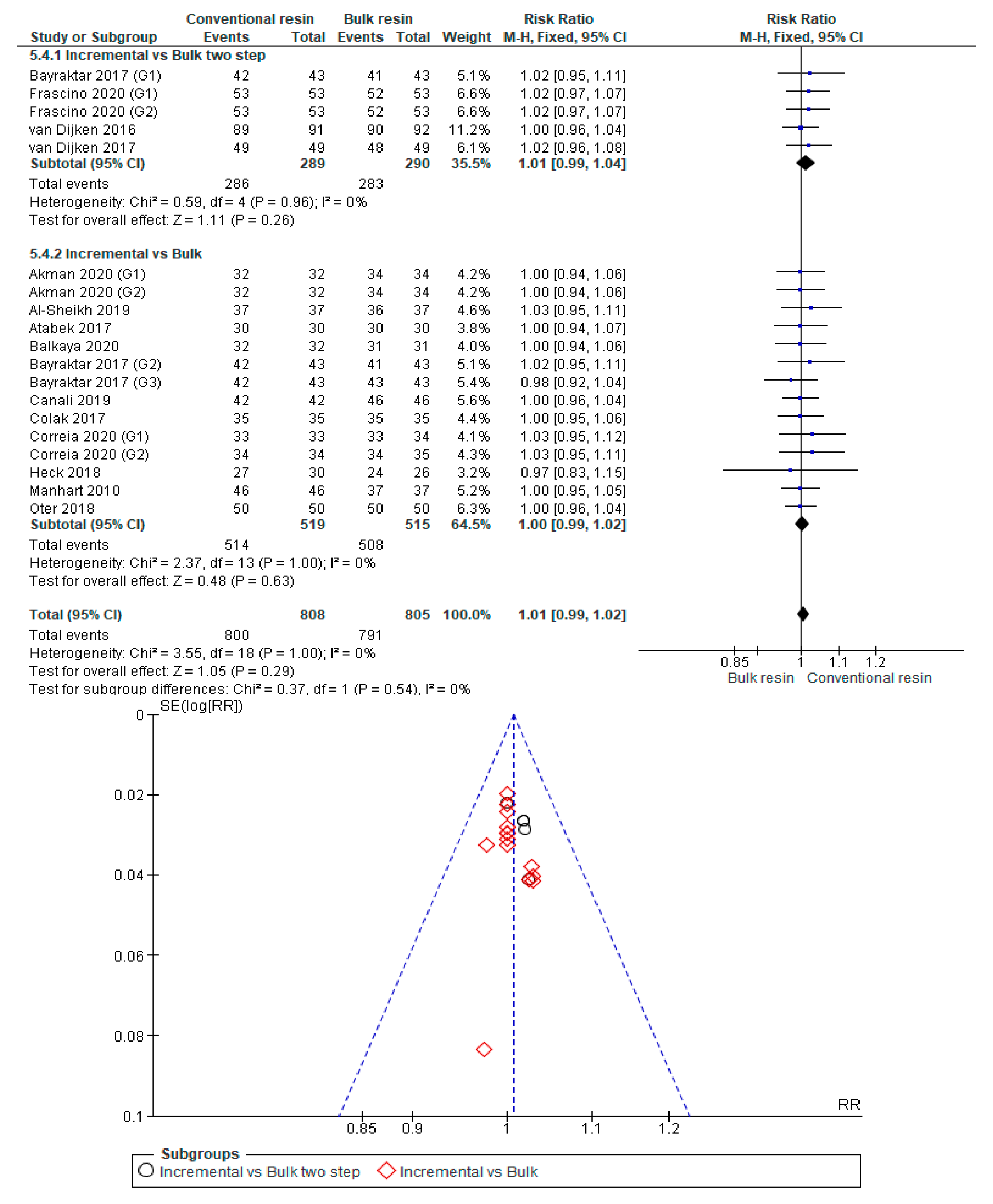
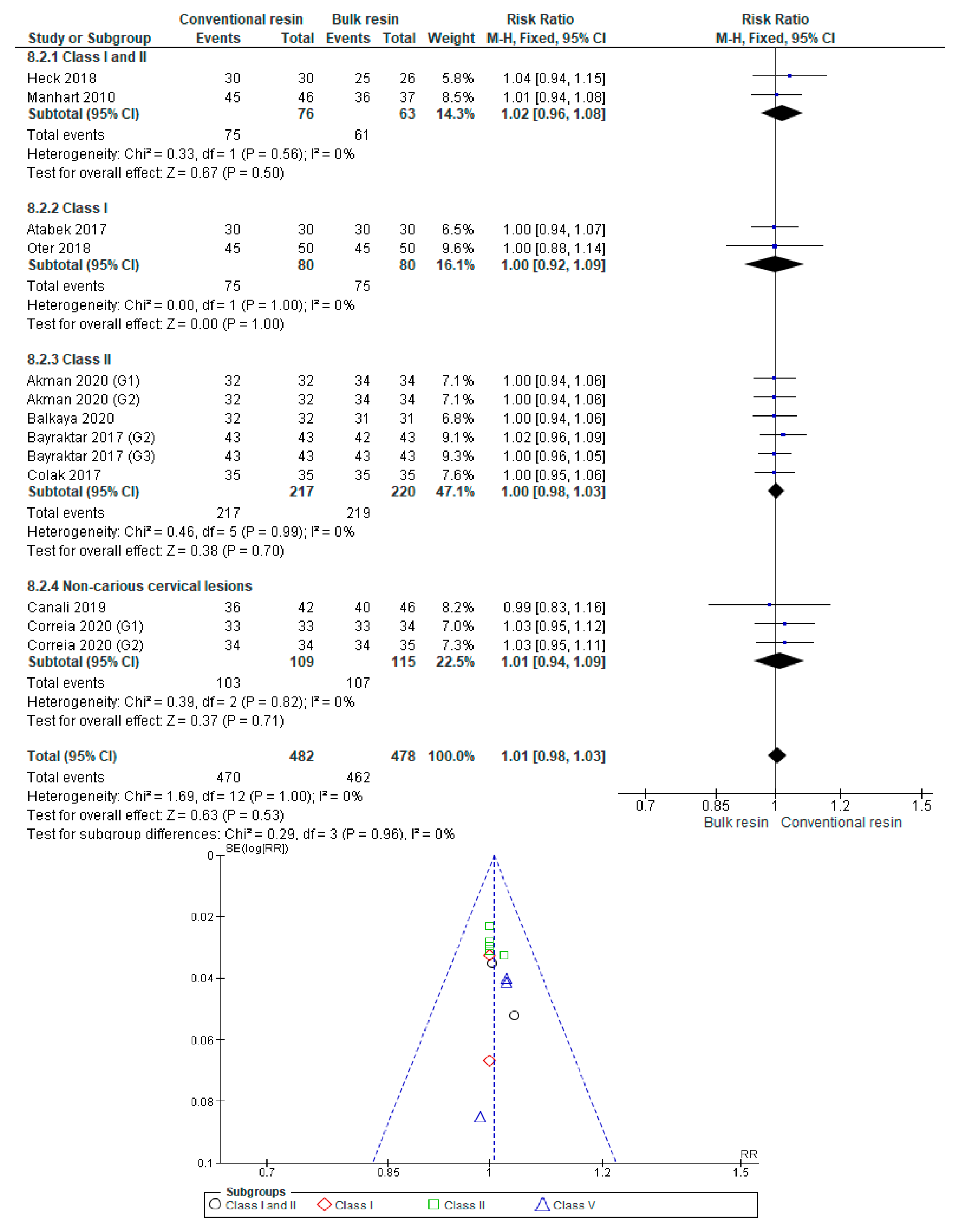
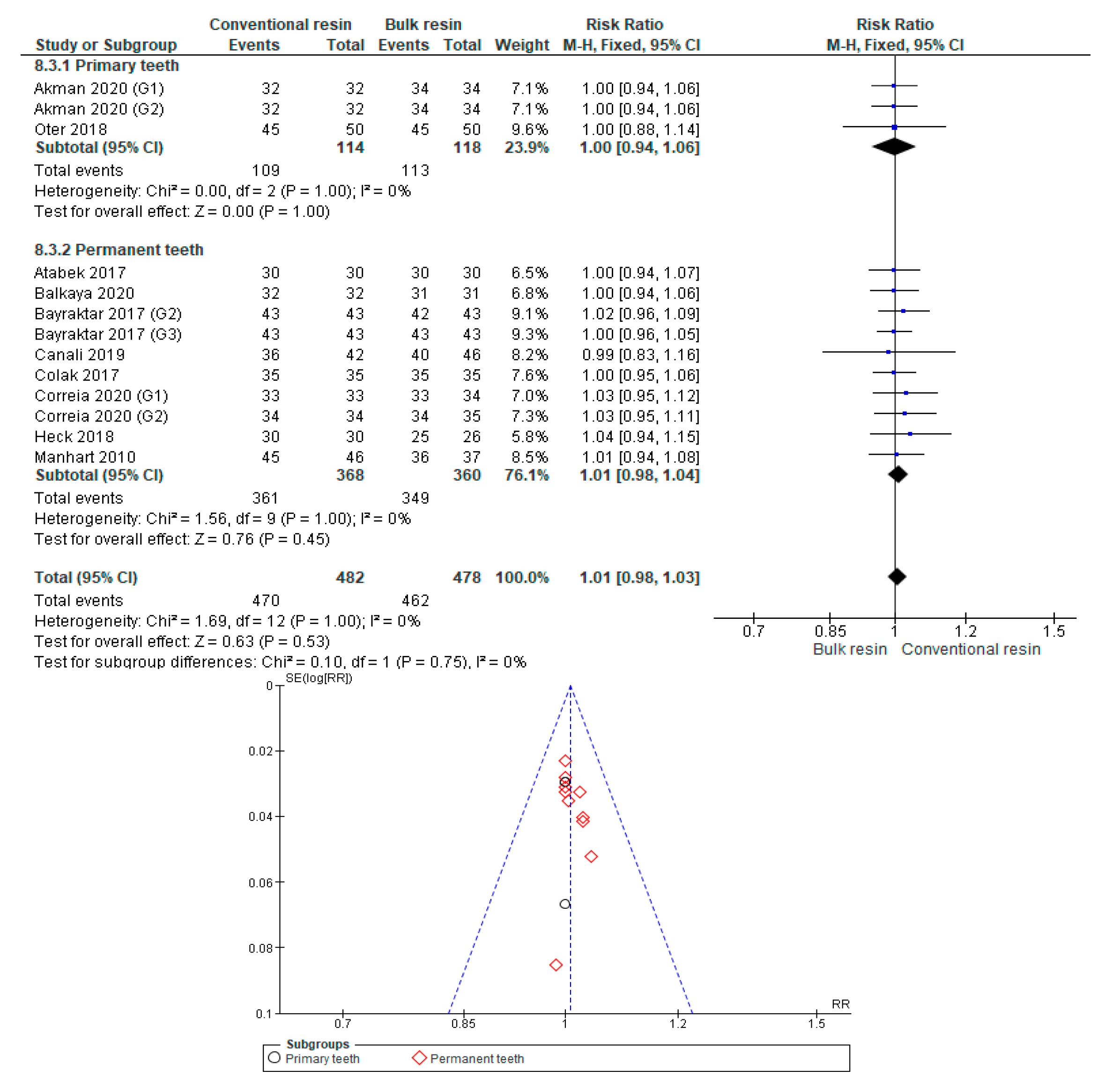
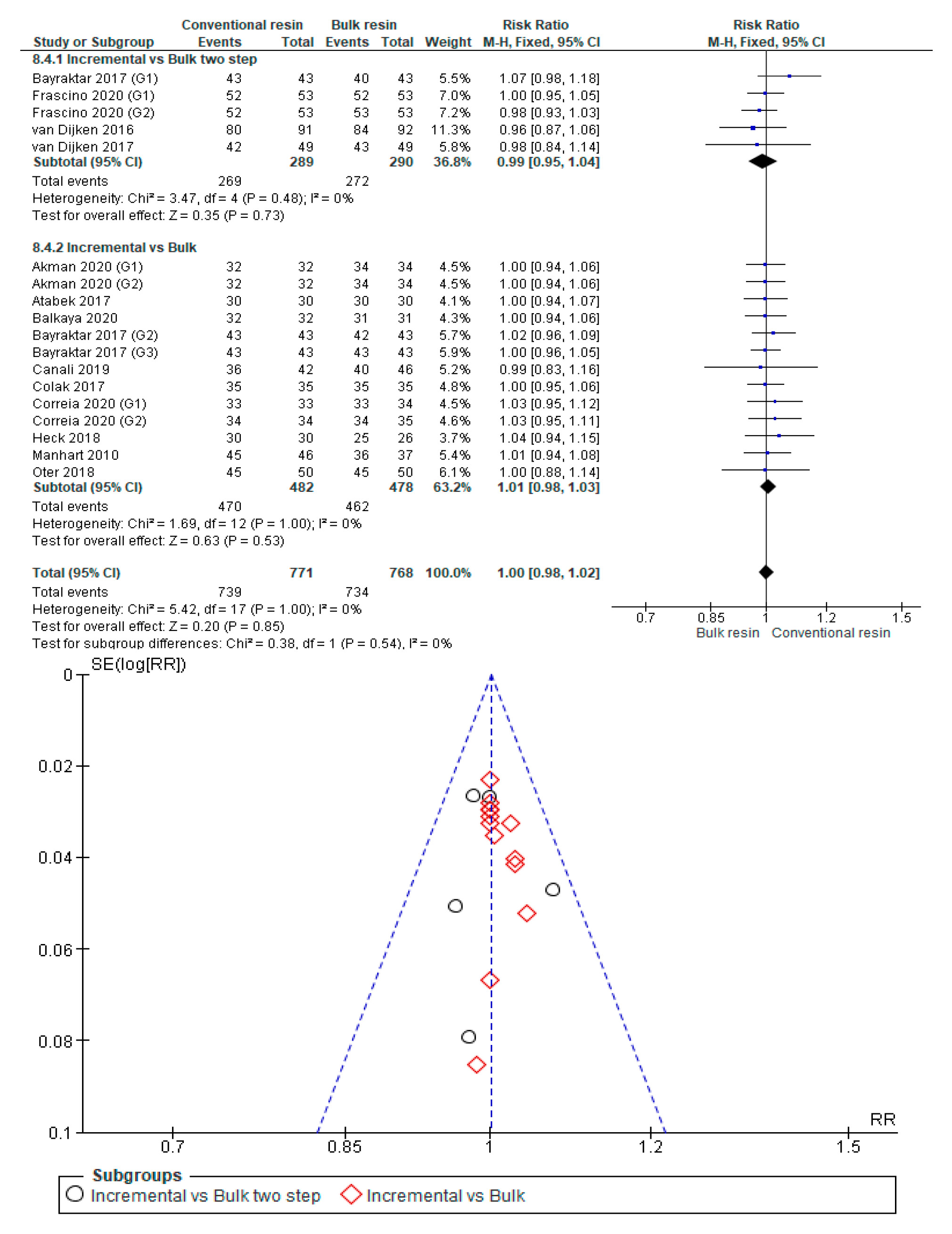
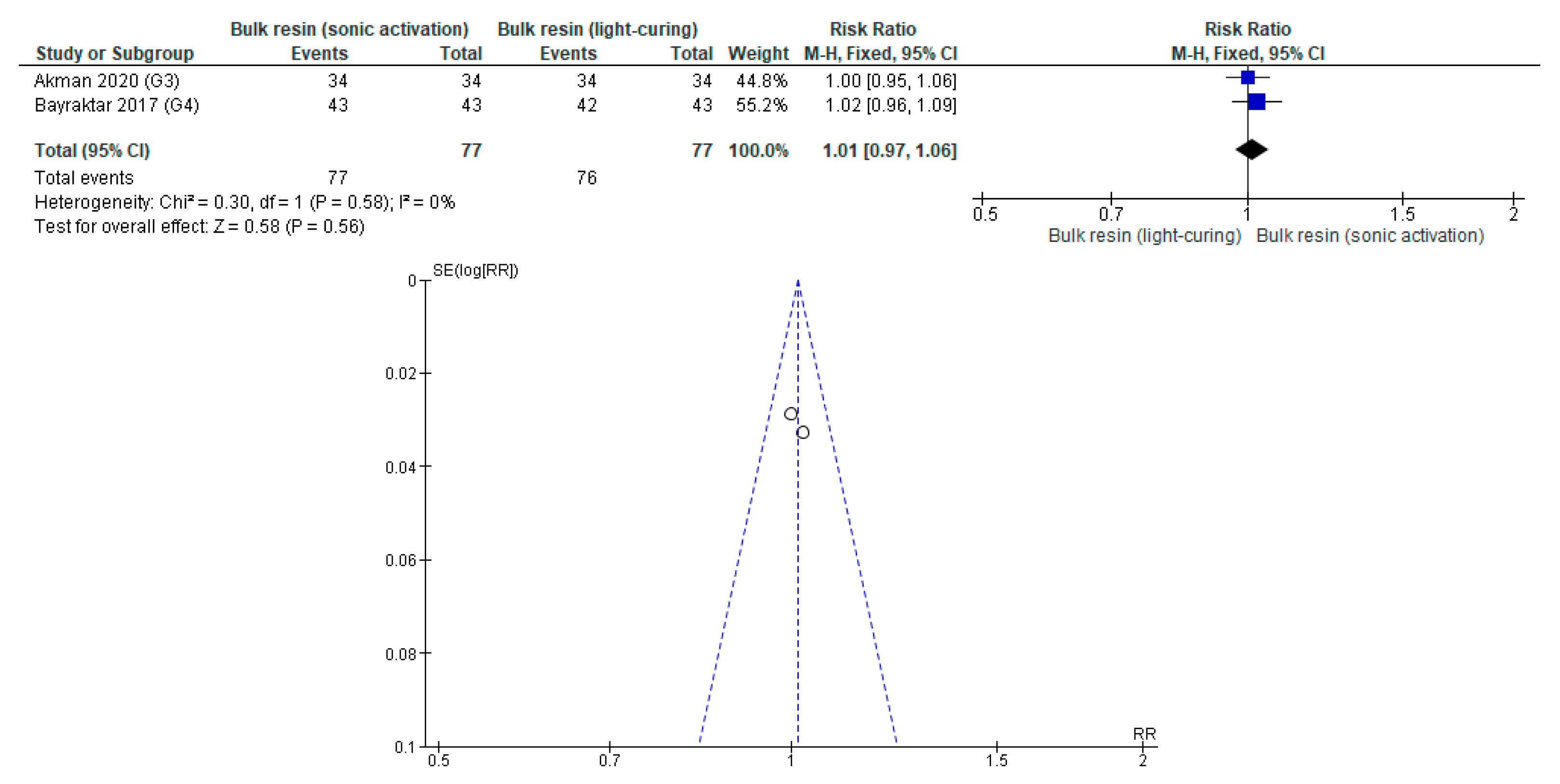
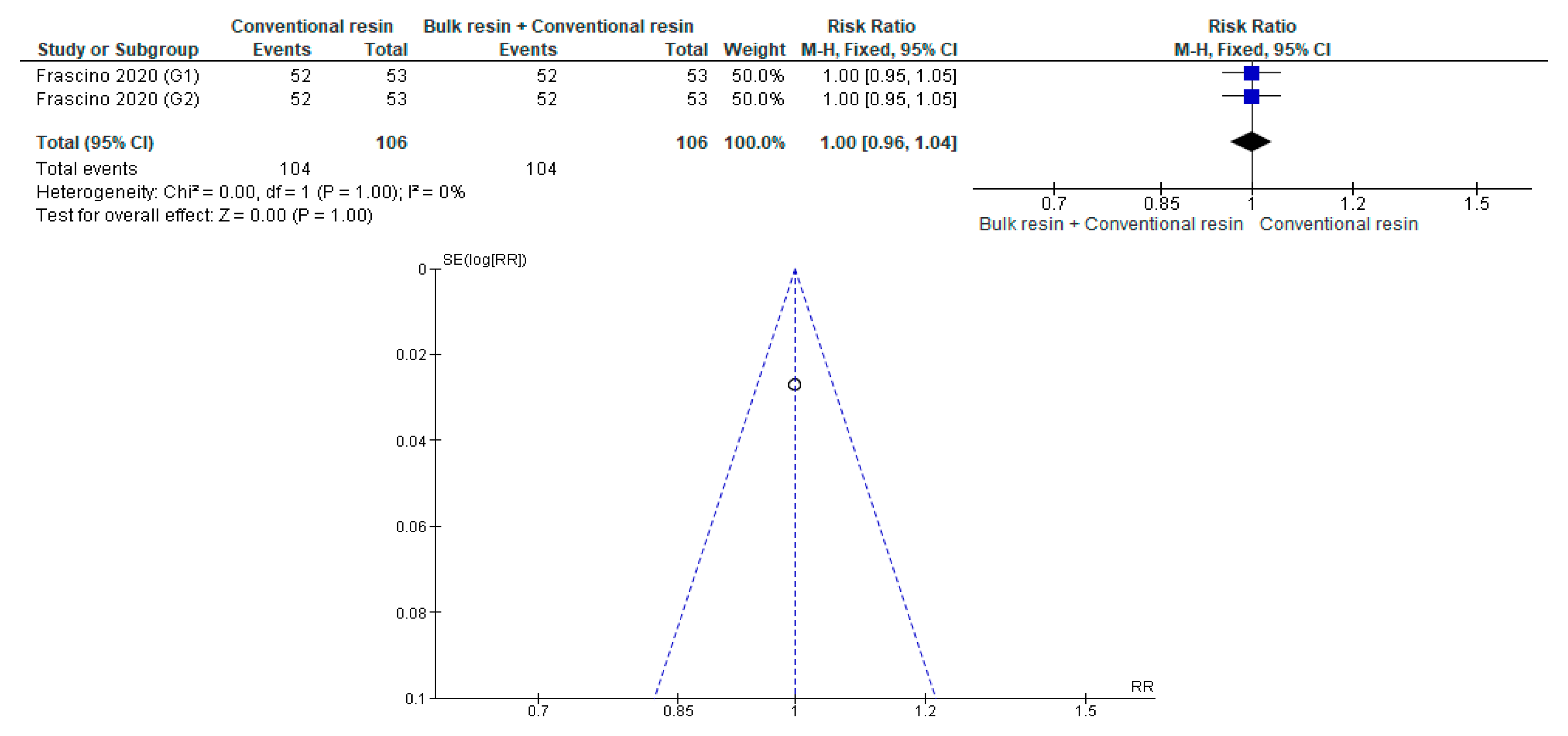
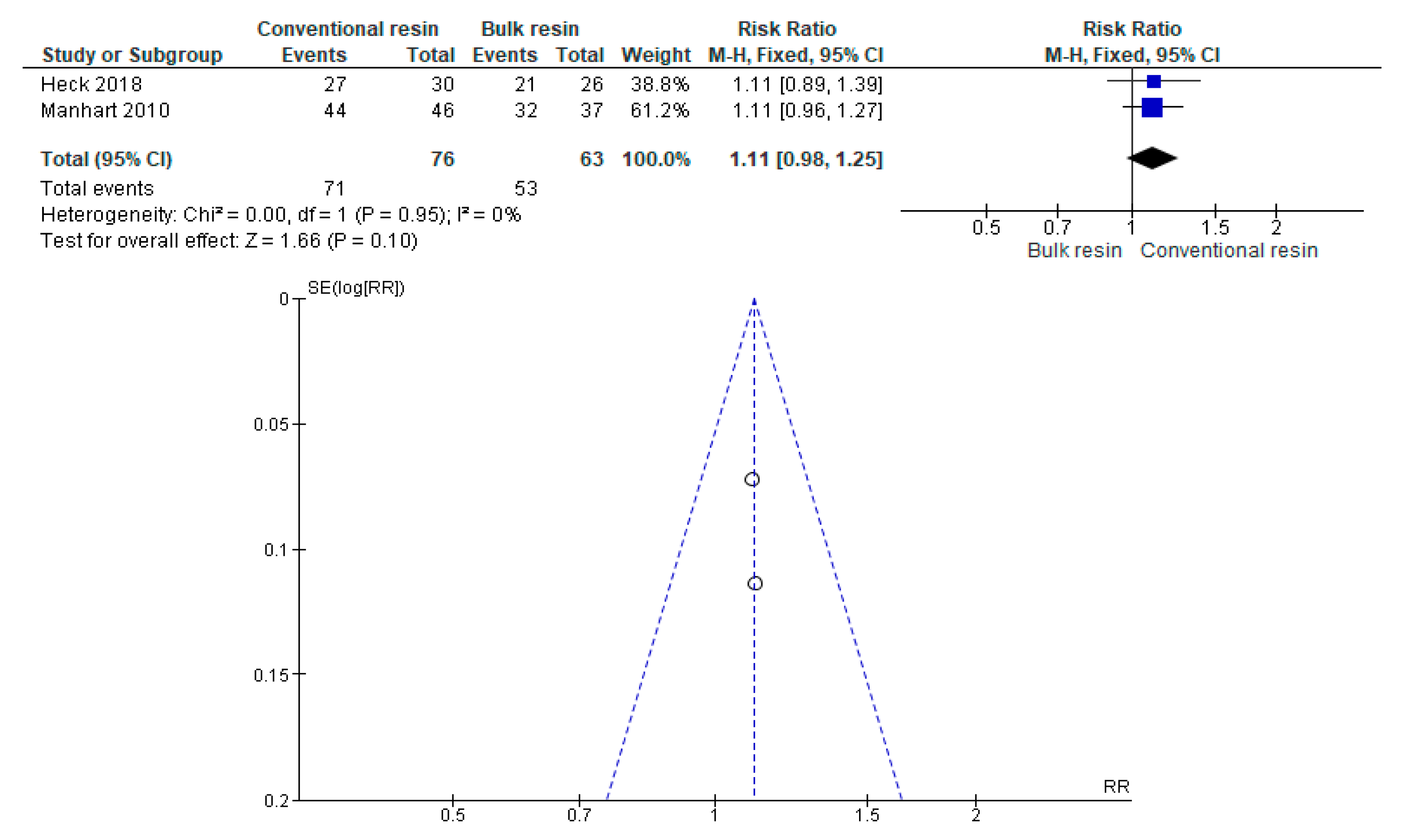
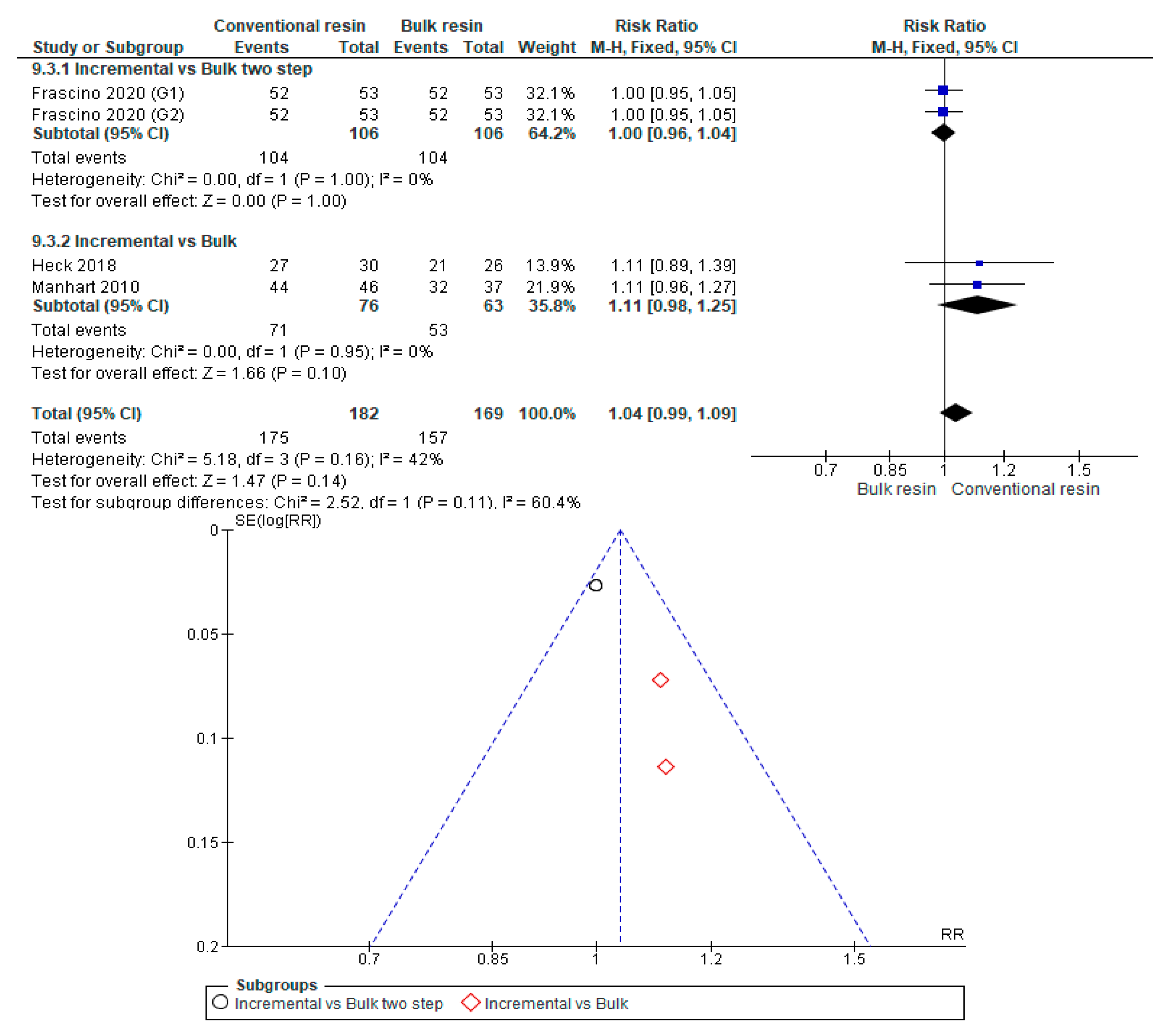
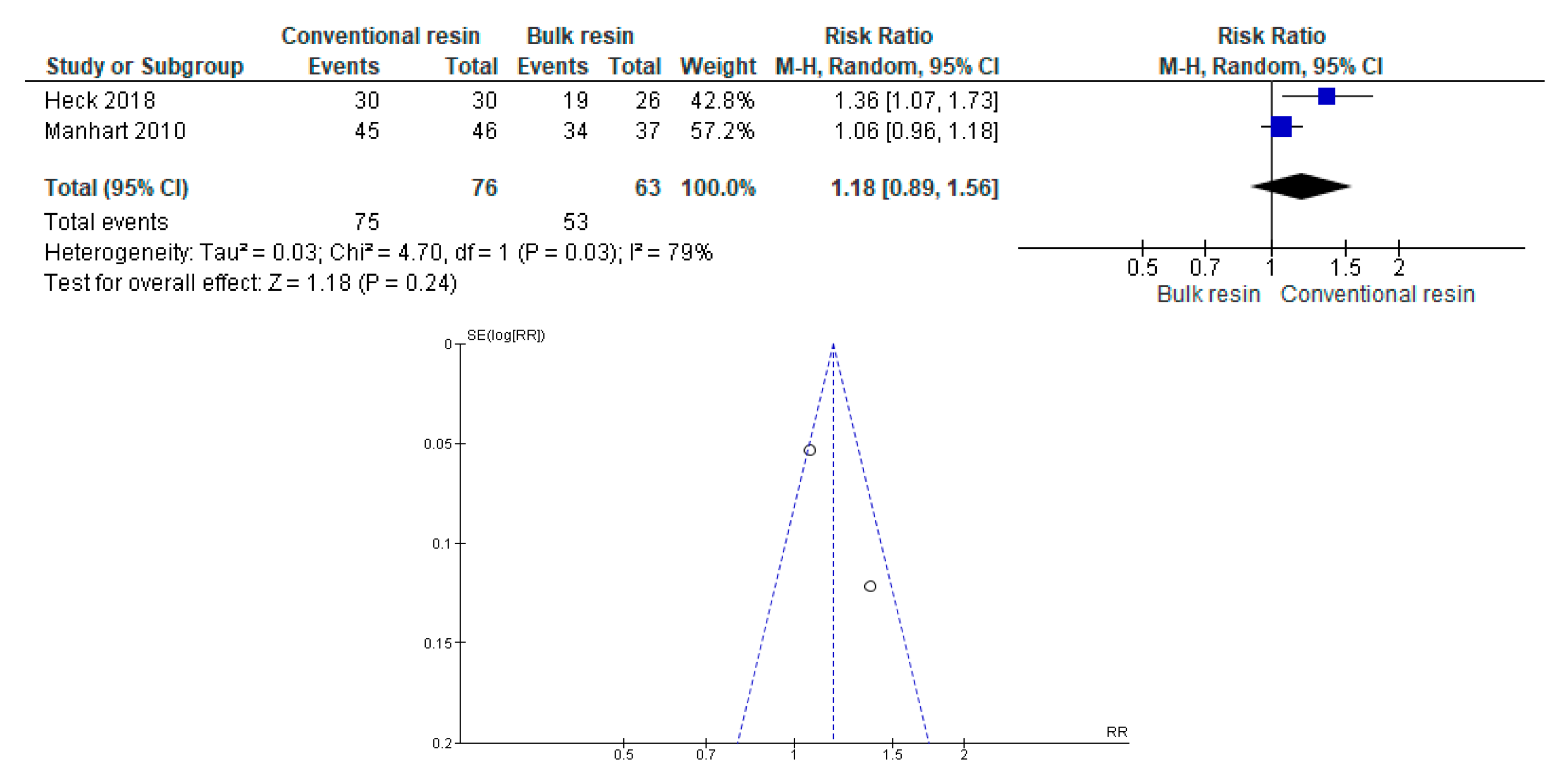
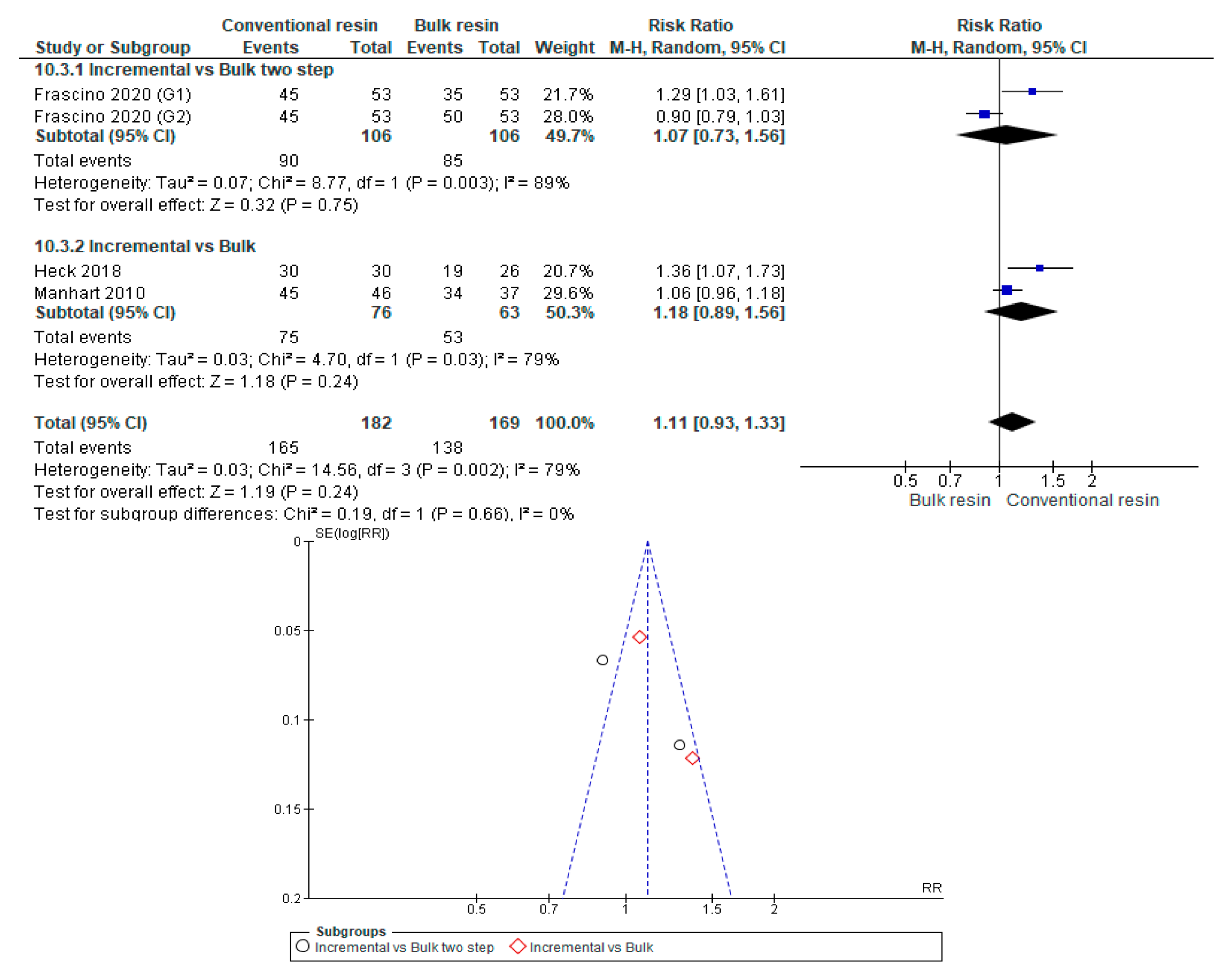
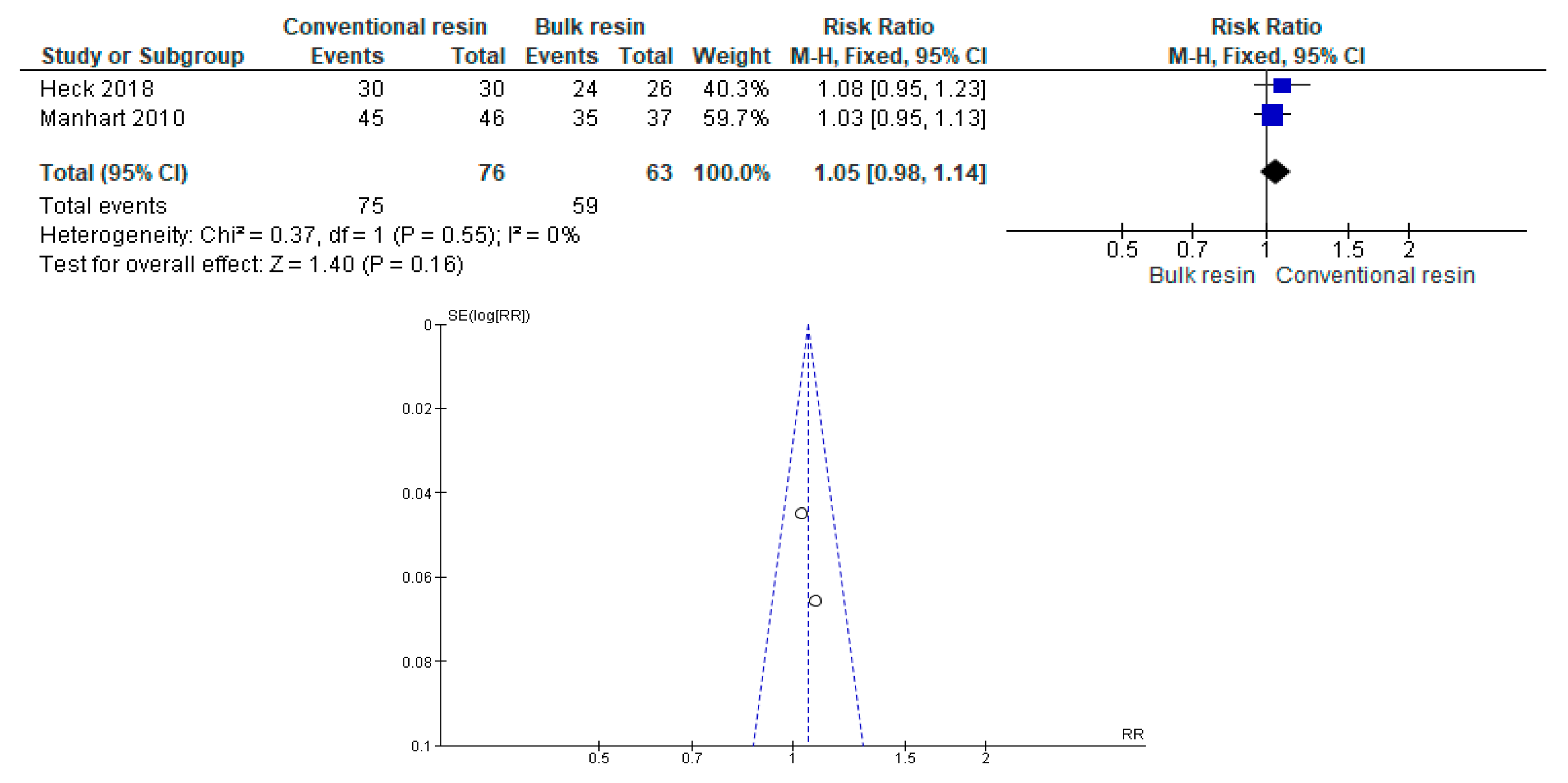
3.4. Synthesis of Results (Meta-Analysis)
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
Appendix A.1. Absence of Fractures





Appendix A.2. Absence of Discoloration or Marginal Staining





Appendix A.3. Adequate Marginal Adaptation





Appendix A.4. Absence of Post-Operative Sensitivity





Appendix A.5. Absence of Secondary Caries





Appendix A.6. Adequate Color Stability and Translucency





Appendix A.7. Proper Surface Texture




Appendix A.8. Proper Anatomical Form





Appendix A.9. Adequate Tooth Integrity/No Wear



Appendix A.10. Adequate Restoration Integrity



Appendix A.11. Proper Occlusion

References
- Yadav, R.; Kumar, M. Dental restorative composite materials: A review. J. Oral Biosci. 2019, 61, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Chesterman, J.; Jowett, A.; Gallacher, A.; Nixon, P. Bulk-fill resin-based composite restorative materials: A review. Br. Dent. J. 2017, 222, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Fugolin, A.P.P.; Pfeifer, C.S. New Resins for Dental Composites. J. Dent. Res. 2017, 96, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Barszczewska-Rybarek, I.M.; Chrószcz, M.W.; Chladek, G. Novel urethane-dimethacrylate monomers and compositions for use as matrices in dental restorative materials. Int. J. Mol. Sci. 2020, 21, 2644. [Google Scholar] [CrossRef] [Green Version]
- Ilie, N.; Hilton, T.J.; Heintze, S.D.; Hickel, R.; Watts, D.C.; Silikas, N.; Stansbury, J.W.; Cadenaro, M.; Ferracane, J.L. Academy of Dental Materials guidance—Resin composites: Part I—Mechanical properties. Dent. Mater. 2017, 33, 880–894. [Google Scholar] [CrossRef]
- Sokolowski, G.; Szczesio, A.; Bociong, K.; Kaluzinska, K.; Lapinska, B.; Sokolowski, J.; Domarecka, M.; Lukomska-Szymanska, M. Dental resin cements-The influence of water sorption on contraction stress changes and hydroscopic expansion. Materials (Basel) 2018, 11, 973. [Google Scholar] [CrossRef] [Green Version]
- Ferracane, J.L. Resin composite—State of the art. Dent. Mater. 2011, 27, 29–38. [Google Scholar] [CrossRef]
- Leprince, J.G.; Palin, W.M.; Vanacker, J.; Sabbagh, J.; Devaux, J.; Leloup, G. Physico-mechanical characteristics of commercially available bulk-fill composites. J. Dent. 2014, 42, 993–1000. [Google Scholar] [CrossRef]
- van Ende, A.; de Munck, J.; Lise, D.P.; van Meerbeek, B. Bulk-fill composites: A review of the current literature. J. Adhes. Dent. 2017, 19, 95–109. [Google Scholar] [CrossRef] [Green Version]
- Corral Núñez, C.; Vildósola Grez, P.; Bersezio Miranda, C.; Alves Dos Campos, E.; Fernández Godoy, E. State of the art of bulk-fill resin-based composites: A review. Rev. Fac. Odontol. 2015, 27, 177–196. [Google Scholar] [CrossRef]
- Lins, R.B.E.; Aristilde, S.; Osório, J.H.; Cordeiro, C.M.B.; Yanikian, C.R.F.; Bicalho, A.A.; Stape, T.H.S.; Soares, C.J.; Martins, L.R.M. Biomechanical behaviour of bulk-fill resin composites in class II restorations. J. Mech. Behav. Biomed. Mater. 2019, 98, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions|Cochrane Training. Available online: https://training.cochrane.org/handbook/current (accessed on 10 June 2020).
- Akman, H.; Tosun, G. Clinical evaluation of bulk-fill resins and glass ionomer restorative materials: A 1-year follow-up randomized clinical trial in children. Niger. J. Clin. Pract. 2020, 23, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Balkaya, H.; Arslan, S. A Two-year Clinical Comparison of Three Different Restorative Materials in Class II Cavities. Oper. Dent. 2020, 45, E32–E42. [Google Scholar] [CrossRef] [PubMed]
- Çolak, H.; Tokay, U.; Uzgur, R.; Hamidi, M.; Ercan, E. A prospective, randomized, double-blind clinical trial of one nano-hybrid and one high-viscosity bulk-fill composite restorative systems in class II cavities: 12 months results. Niger. J. Clin. Pract. 2017, 20, 822–831. [Google Scholar] [CrossRef]
- van Dijken, J.W.V.; Pallesen, U. Bulk-filled posterior resin restorations based on stress-decreasing resin technology: A randomized, controlled 6-year evaluation. Eur. J. Oral Sci. 2017, 125, 303–309. [Google Scholar] [CrossRef]
- Yazici, A.R.; Antonson, S.A.; Kutuk, Z.B.; Ergin, E. Thirty-six-month clinical comparison of bulk fill and nanofill composite restorations. Oper. Dent. 2017, 42, 478–485. [Google Scholar] [CrossRef]
- van Dijken, J.W.V.; Pallesen, U. Posterior bulk-filled resin composite restorations: A 5-year randomized controlled clinical study. J. Dent. 2016, 51, 29–35. [Google Scholar] [CrossRef]
- Arhun, N.; Celik, C.; Yamanel, K. Clinical evaluation of resin-based composites in posterior restorations: Two-year results. Oper. Dent. 2010, 35, 397–404. [Google Scholar] [CrossRef]
- Manhart, J.; Chen, H.-Y.; Hickel, R. Clinical evaluation of the posterior composite Quixfil in class I and II cavities: 4-year follow-up of a randomized controlled trial. J. Adhes. Dent. 2010, 12, 237–243. [Google Scholar] [CrossRef]
- Correia, A.; Jurema, A.; Andrade, M.R.; Borges, A.; Bresciani, E.; Caneppele, T. Clinical Evaluation of Noncarious Cervical Lesions of Different Extensions Restored With Bulk-fill or Conventional Resin Composite: Preliminary Results of a Randomized Clinical Trial. Oper. Dent. 2020, 45, E11–E20. [Google Scholar] [CrossRef] [PubMed]
- Frascino, S.M.B.; Fagundes, T.C.; Silva, U.A.E.; Rahal, V.; Barboza, A.C.S.; Santo, P.H.; Briso, A.L.F. Randomized Prospective Clinical Trial of Class II Restorations Using Low-shrinkage Flowable Resin Composite. Oper. Dent. 2020, 45, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Al-Sheikh, R. Effects of Different Application Techniques on Nanohybrid Composite Restorations Clinical Success. Open Dent. J. 2019, 13, 228–235. [Google Scholar] [CrossRef] [Green Version]
- Canali, G.D.; Ignácio, S.A.; Rached, R.N.; Souza, E.M. One-year clinical evaluation of bulk-fill flowable vs. regular nanofilled composite in non-carious cervical lesions. Clin. Oral Investig. 2019, 23, 889–897. [Google Scholar] [CrossRef] [PubMed]
- Heck, K.; Manhart, J.; Hickel, R.; Diegritz, C. Clinical evaluation of the bulk fill composite QuiXfil in molar class I and II cavities: 10-year results of a RCT. Dent. Mater. 2018, 34, e138–e147. [Google Scholar] [CrossRef]
- Oter, B.; Deniz, K.; Cehreli, S. Preliminary data on clinical performance of bulk-fill restorations in primary molars. Niger. J. Clin. Pract. 2018, 21, 1484–1491. [Google Scholar] [CrossRef]
- Atabek, D.; Aktaş, N.; Sakaryali, D.; Bani, M. Two-year clinical performance of sonic-resin placement system in posterior restorations. Quintessence Int. (Berl) 2017, 48, 743–751. [Google Scholar] [CrossRef]
- Bayraktar, Y.; Ercan, E.; Hamidi, M.M.; Çolak, H. One-year clinical evaluation of different types of bulk-fill composites. J. Investig. Clin. Dent. 2017, 8, e12210. [Google Scholar] [CrossRef]
- Malhotra, N.; Mala, K.; Acharya, S. Resin-based composite as a direct esthetic restorative material. Compend. Contin. Educ. Dent. 2011, 32, 14–38. [Google Scholar]
- Malhotra, N.; Kundabala, M.; Shashirashmi, A. Strategies to overcome polymerization shrinkage--materials and techniques. A review. Dent. Update 2010, 37, 115–125. [Google Scholar] [CrossRef]
- Rees, J.S.; Jagger, D.C.; Williams, D.R.; Brown, G.; Duguid, W. A reappraisal of the incremental packing technique for light cured composite resins. J. Oral Rehabil. 2004, 31, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Moore, B.K.; Platt, J.A.; Borges, G.; Chu, T.M.G.; Katsilieri, I. Depth of cure of dental resin composites: ISO 4049 depth and microhardness of types of materials and shades. Oper. Dent. 2008, 33, 408–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Chang, J.; Ferracane, J.; Lee, I.B. How should composite be layered to reduce shrinkage stress: Incremental or bulk filling? Dent. Mater. 2008, 24, 1501–1505. [Google Scholar] [CrossRef] [PubMed]
- Fronza, B.M.; Rueggeberg, F.A.; Braga, R.R.; Mogilevych, B.; Soares, L.E.S.; Martin, A.A.; Ambrosano, G.; Giannini, M. Monomer conversion, microhardness, internal marginal adaptation, and shrinkage stress of bulk-fill resin composites. Dent. Mater. 2015, 31, 1542–1551. [Google Scholar] [CrossRef] [PubMed]
- El-Safty, S.; Akhtar, R.; Silikas, N.; Watts, D.C. Nanomechanical properties of dental resin-composites. Dent. Mater. 2012, 28, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Lien, W.; Vandewalle, K.S. Physical properties of a new silorane-based restorative system. Dent. Mater. 2010, 26, 337–344. [Google Scholar] [CrossRef]
- Li, X.; Pongprueksa, P.; Van Meerbeek, B.; De Munck, J. Curing profile of bulk-fill resin-based composites. J. Dent. 2015, 43, 664–672. [Google Scholar] [CrossRef]
- El-Damanhoury, H.M.; Platt, J.A. Polymerization shrinkage stress kinetics and related properties of bulk-fill resin composites. Oper. Dent. 2014, 39, 374–382. [Google Scholar] [CrossRef]
- Opdam, N.J.M.; Van De Sande, F.H.; Bronkhorst, E.; Cenci, M.S.; Bottenberg, P.; Pallesen, U.; Gaengler, P.; Lindberg, A.; Huysmans, M.C.D.N.J.M.; Van Dijken, J.W. Longevity of posterior composite restorations: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 943–949. [Google Scholar] [CrossRef]
- Kim, R.J.Y.; Kim, Y.J.; Choi, N.S.; Lee, I.B. Polymerization shrinkage, modulus, and shrinkage stress related to tooth-restoration interfacial debonding in bulk-fill composites. J. Dent. 2015, 43, 430–439. [Google Scholar] [CrossRef]
- Nedeljkovic, I.; Teughels, W.; De Munck, J.; Van Meerbeek, B.; Van Landuyt, K.L. Is secondary caries with composites a material-based problem? Dent. Mater. 2015, 31, e247–e277. [Google Scholar] [CrossRef] [PubMed]
- Sarrett, D.C. Clinical challenges and the relevance of materials testing for posterior composite restorations. Dent. Mater. 2005, 21, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Unemori, M.; Matsuya, Y.; Akashi, A.; Goto, Y.; Akamine, A. Composite resin restoration and postoperative sensitivity: Clinical follow-up in an undergraduate program. J. Dent. 2001, 29, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Costa, T.R.F.; Rezende, M.; Sakamoto, A.; Bittencourt, B.; Dalzochio, P.; Loguercio, A.D.; Reis, A. Influence of adhesive type and placement technique on postoperative sensitivity in posterior composite restorations. Oper. Dent. 2017, 42, 143–154. [Google Scholar] [CrossRef]
- Lapinska, B.; Konieczka, M.; Zarzycka, B.; Sokolowski, K.; Grzegorczyk, J.; Lukomska-Szymanska, M. Flow Cytometry Analysis of Antibacterial Effects of Universal Dentin Bonding Agents on Streptococcus mutans. Molecules 2019, 24, 532. [Google Scholar] [CrossRef] [Green Version]
- Lukomska-Szymanska, M.; Konieczka, M.; Zarzycka, B.; Lapinska, B.; Grzegorczyk, J.; Sokolowski, J. Antibacterial activity of commercial dentine bonding systems against E. faecalis-flow cytometry study. Materials (Basel) 2017, 10, 481. [Google Scholar] [CrossRef] [Green Version]
- Wawrzynkiewicz, A.; Rozpedek-Kaminska, W.; Galita, G.; Lukomska-Szymanska, M.; Lapinska, B.; Sokolowski, J.; Majsterek, I. The Cytotoxicity and Genotoxicity of Three Dental Universal Adhesives-An In Vitro Study. Int. J. Mol. Sci. 2020, 21, 3950. [Google Scholar] [CrossRef]
- Zecin-Deren, A.; Sokolowski, J.; Szczesio-Wlodarczyk, A.; Piwonski, I.; Lukomska-Szymanska, M.; Lapinska, B. Multi-Layer Application of Self-Etch and Universal Adhesives and the Effect on Dentin Bond Strength. Molecules 2019, 24, 345. [Google Scholar] [CrossRef] [Green Version]
- Zecin-Deren, A.; Lukomska-Szymanska, M.; Szczesio-Wlodarczyk, A.; Piwonski, I.; Sokolowski, J.; Lapinska, B. The Influence of Application Protocol of Simplified and Universal Adhesives on the Dentin Bonding Performance. Appl. Sci. 2020, 10, 124. [Google Scholar] [CrossRef] [Green Version]
- Reis, A.; Dourado Loguercio, A.; Schroeder, M.; Luque-Martinez, I.; Masterson, D.; Cople Maia, L. Does the adhesive strategy influence the post-operative sensitivity in adult patients with posterior resin composite restorations?: A systematic review and meta-analysis. Dent. Mater. 2015, 31, 1052–1067. [Google Scholar] [CrossRef]
- Schenkel, A.B.; Peltz, I.; Veitz-Keenan, A. Dental cavity liners for Class I and Class II resin-based composite restorations. Cochrane Database Syst. Rev. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Veloso, S.R.M.; Lemos, C.A.A.; de Moraes, S.L.D.; do Egito Vasconcelos, B.C.; Pellizzer, E.P.; de Melo Monteiro, G.Q. Clinical performance of bulk-fill and conventional resin composite restorations in posterior teeth: A systematic review and meta-analysis. Clin. Oral Investig. 2019, 23, 221–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cidreira Boaro, L.C.; Pereira Lopes, D.; de Souza, A.S.C.; Lie Nakano, E.; Ayala Perez, M.D.; Pfeifer, C.S.; Gonçalves, F. Clinical performance and chemical-physical properties of bulk fill composites resin—A systematic review and meta-analysis. Dent. Mater. 2019, 35, e249–e264. [Google Scholar] [CrossRef] [PubMed]
- Nayyer, M.; Zahid, S.; Hassan, S.H.; Mian, S.A.; Mehmood, S.; Khan, H.A.; Kaleem, M.; Zafar, M.S.; Khan, A.S. Comparative abrasive wear resistance and surface analysis of dental resin-based materials. Eur. J. Dent. 2018, 12, 57–66. [Google Scholar] [CrossRef]
- Azam, M.T.; Khan, A.S.; Muzzafar, D.; Faryal, R.; Siddiqi, S.A.; Ahmad, R.; Chauhdry, A.A.; Rehman, I.U. Structural, surface, in vitro bacterial adhesion and biofilm formation analysis of three dental restorative composites. Materials (Basel) 2015, 8, 3221–3237. [Google Scholar] [CrossRef]
- Chladek, G.; Basa, K.; Żmudzki, J.; Malara, P.; Nowak, A.J.; Kasperski, J. Influence of aging solutions on wear resistance and hardness of selected resin-based dental composites. Acta Bioeng. Biomech. 2016, 18, 43–52. [Google Scholar] [CrossRef]
- Bayne, S.C.; Schmalz, G. Reprinting the classic article on USPHS evaluation methods for measuring the clinical research performance of restorative materials. Clin. Oral Investig. 2005, 9, 1–6. [Google Scholar] [CrossRef]
- Hickel, R.; Roulet, J.F.; Bayne, S.; Heintze, S.D.; Mjör, I.A.; Peters, M.; Rousson, V.; Randall, R.; Schmalz, G.; Tyas, M.; et al. Recommendations for conducting controlled clinical studies of dental restorative materials. Clin. Oral Investig. 2007, 11, 5–33. [Google Scholar] [CrossRef]
- Göstemeyer, G.; Blunck, U.; Paris, S.; Schwendicke, F. Design and validity of randomized controlled dental restorative trials. Materials (Basel) 2016, 9, 372. [Google Scholar] [CrossRef]
- Opdam, N.J.M.; Collares, K.; Hickel, R.; Bayne, S.C.; Loomans, B.A.; Cenci, M.S.; Lynch, C.D.; Correa, M.B.; Demarco, F.; Schwendicke, F.; et al. Clinical studies in restorative dentistry: New directions and new demands. Dent. Mater. 2018, 34, 1–12. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Author(s) | Year | Country | Type of Study | Number of Patients (Men/Women) | Number of Teeth Restored | Average Age (Range) | Follow-up | Groups | Patients Per Group | Teeth Per Group | Restoration Type | Tooth Type | Evaluation Criteria | Engraving Method | Adhesive | Resin | Placement Technique |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Akman et al. [14] | 2020 | Turkey | RCT parallel double-blind | 30 | 160 | (6–10) | 1 year | Glass ionomer | 30 | 40 | Class II | Primary Molar | Modified US Public Health Service | Etching and rinsing - 20% polyacrylic acid (Cavity Conditioner, GC Corp., Japan) | ----------- | Equia Fil (GC Corporation, Japan) | Injected |
| Bulk Resin | 30 | 40 | Self-etch | Clearfil SE Bond (Kuraray, Tokyo Japan) | SonicFill (Kerr Corporation, USA) | Bulk with sonic activation | |||||||||||
| Bulk Resin | 30 | 40 | X-tra fil (Voco, Germany) | Bulk | |||||||||||||
| Conventional Resin | 30 | 40 | Filtek Z550 (3M ESPE, USA) | Incremental | |||||||||||||
| Balkaya et al. [15] | 2020 | Turkey | RCT split mouth double-blind | 54 (23/31) | 109 | 22 (20–32) | 4 years | Conventional Resin | 54 | 37 | Class II | Premolar and Molar | Modified US Public Health Service | Self-etch | Single Bond Universal adhesive (3M ESPE, Neuss, Germany) | Charisma Smart Composite (Heraeus Kulzer, Hanau, Germany) | Incremental |
| Bulk Resin | 54 | 38 | Filtek Bulk Fill Posterior Restorative (3M ESPE, St. Paul, MN, USA) | Bulk | |||||||||||||
| Glass ionomer | 54 | 34 | ---------- | Equia Forte Fil (GC, Tokyo, Japan) | Injected | ||||||||||||
| Correia et al. [22] | 2020 | Brazil | RCT parallel double-blind | 77 (34/43) | 140 | (21–80) | 1 year | Conventional Resin—1.5 mm OGD | 28 | 35 | NCCL | Canine and Premolar | Modified US Public Health Service | Self-etch | Clearfil SE Bond (Kuraray America, Inc, New York, NY, USA) | Filtek Z350 XT (3M ESPE, St Paul, MN, USA) | Incremental |
| Bulk Resin—1.5 mm OGD | 27 | 35 | Filtek Bulk Fill Posterior (3M ESPE) | Bulk | |||||||||||||
| Conventional Resin—3 mm OGD | 27 | 35 | Filtek Z350 XT (3M ESPE, St Paul, MN, USA) | Incremental | |||||||||||||
| Bulk Resin—3 mm OGD | 29 | 35 | Filtek Bulk Fill Posterior (3M ESPE) | Bulk | |||||||||||||
| Frascino et al. [23] | 2020 | Brazil | RCT split mouth | 53 | 159 | 48.3 ± 10 | 1 year | Conventional Resin | 53 | 53 | Class II | Premolar and Molar | Modified US Public Health Service | Etching and rinsing—35% phosphoric acid gel (Ultra-Etch, Ultradent) | Peak Universal (Ultradent, South Jordan, UT, USA) | Amelogen Plus (Ultradent, South Jordan, UT, USA) | Incremental |
| Bulk Resin + Conventional Resin | 53 | 53 | Adper Single Bond 2 (3M ESPE, St Paul, MN, USA) | Filtek Bulk Fill Flow (3M ESPE, St Paul, MN, USA) + Filtek Z350XT (3M ESPE, St Paul, MN, USA) | Two-step Bulk (4 mm + 2 mm) | ||||||||||||
| Bulk Resin + Conventional Resin | 53 | 53 | XP Bond (Dentsply, Milford, DE, USA) | SureFil SDR (Dentsply, Milford, DE, USA) + TPH3 (Dentsply, Milford, DE, USA) | Two-step Bulk (4 mm + 2 mm) | ||||||||||||
| Al-Sheikh [24] | 2019 | Saudi Arabia | RCT split mouth | 40 | 80 | (20–40) | 6 months | Conventional Resin | 40 | 40 | Class I | Molar | Modified US Public Health Service | Etching and rinsing—Tetric NEtch (Ivoclar Vivadent, Schaan, Liechtenstein) | Tetric NBond Total-Etch (Ivoclar Vivadent, Schaan, Liechtenstein) | Tetric EvoCeram (Ivoclar Vivadent, Schaan, Liechtenstein) | Incremental |
| Bulk Resin | 40 | 40 | Tetric EvoCeram bulk-fill (Ivoclar Vivadent, Schaan, Liechtenstein) | Bulk | |||||||||||||
| Canali et al. [25] | 2019 | Brazil | RCT split mouth double-blind | 22 (5/17) | 89 | 41.1 ± 12.7 (21–69) | 1 year | Conventional resin | 22 | 43 | NCCL | Incisor, canine, premolar and molar | Modified US Public Health Service | Self-etch | Scotchbond Universal Adhesive (3M ESPE, St. Paul, MN) | Filtek Supreme Ultra Universal (3M ESPE, St. Paul, MN) | Incremental |
| Bulk resin | 22 | 46 | Filtek Bulk Fill Flowable (3M ESPE, St. Paul, MN) | Bulk | |||||||||||||
| Heck et al. [26] | 2018 | Germany | RCT split mouth | 46 | 96 | (>18) | 10 years | Conventional resin | 46 | 50 | Class I and II | Molar | Modified US Public Health Service | Etching and rising—37% phosphoric acid | Syntac classic (Ivoclar Vivadent, Schaan, Liechtenstein) | Tetric Ceram (Ivoclar Vivadent, Schaan, Liechtenstein) | Incremental |
| Bulk resin | 46 | 46 | Self-etch | Xeno III (Dentsply De Trey, Konstanz, Germany) | QuiXfil (Dentsply De Trey, Konstanz, Germany) | Bulk | |||||||||||
| Oter et al. [27] | 2018 | Turkey | RCT split mouth single-blind | 80 | 160 | 7.41 ± 1.8 | 1 year | Conventional resin | 80 | 80 | Class I | PrimaryMolar | Modified US Public Health Service | Etching and rising | Single Bond Universal Adhesive (3M, Neuss, Germany) | Filtek Z250 (3M ESPE, St Paul, USA) | Incremental |
| Bulk resin | 80 | 80 | Filtek Bulk-Fill Restorative (3M ESPE, St Paul, USA). | Bulk | |||||||||||||
| Atabek et al. [28] | 2017 | Turkey | RCT split mouth | 30 | 60 | (7–16) | 2 years | Conventional resin | 30 | 30 | Class I | Molar | Modified US Public Health Service | Self-etch | OptiBond All-In-One (Kawo Sonic Fill System; Kerr, Orange, USA) | Herculite Ultra (Kerr, Orange, USA) | Incremental |
| Bulk resin | 30 | 30 | SonicFill (Kawo Sonic Fill System; Kerr, Orange, USA) | Bulk with sonic activation | |||||||||||||
| Bayraktar et al. [29] | 2017 | Turkey | RCT split mouth | 50 | 200 | 25.8 ± 7.49 (18–45) | 1 year | Conventional resin | 50 | 50 | Class II | Premolar and Molar | Modified US Public Health Service | Self-etch | Clearfil SE Bond (Kuraray, Okayama, Japan) | Clearfil Photo Posterior (Kuraray, Okayama, Japan) | Incremental |
| Bulk Resin + Conventional Resin | 50 | 50 | Single Bond Universal (3M ESPE, St Paul, USA) | Filtek Bulk-Fill Flowable (3M ESPE, St Paul, USA) + Filtek P60 (3M ESPE, St Paul, USA) | Two-step Bulk (2–4 mm + 2 mm) | ||||||||||||
| Bulk resin | 50 | 50 | Adhe SE Bond (Ivoclar Vivadent, Schaan, Liechtenstein) | Tetric EvoCeram Bulk-Fill (Ivoclar Vivadent, Schaan, Liechtenstein) | Bulk | ||||||||||||
| Bulk resin | 50 | 50 | OptiBond All-In-One (Kawo Sonic Fill System; Kerr, Orange, USA) | SonicFill (Kawo Sonic Fill System; Kerr, Orange, USA) | Bulk with sonic activation | ||||||||||||
| Colak et al. [16] | 2017 | Turkey | RCT split mouth double–blind | 34 (24/10) | 74 | 33.74 ± 6.8 (23–56) | 1 year | Conventional resin | 34 | 37 | Class II | Premolar and Molar | Modified US Public Health Service | Self-etch | AdheSE Bond (Ivoclar Vivadent, Schaan, Liechtenstein) | Tetric EvoCeram (Ivoclar Vivadent, Schaan, Liechtenstein) | Incremental |
| Bulk resin | 34 | 37 | Tetric EvoCeram bulk-fill (Ivoclar Vivadent, Schaan, Liechtenstein) | Bulk | |||||||||||||
| van Dijken et al. [17] | 2017 | Sweden | RCT split mouth double blind | 38 (22/16) | 106 | 55.3 (32–87) | 6 years | Conventional resin | 38 | 53 | Class I and II | Premolar and Molar | Modified US Public Health Service | Self-etch | XenoV (Dentsply Sirona, Konstanz, Germany) | Ceram X mono (DentsplySirona, Konstanz, Germany) | Incremental |
| Bulk Resin + Conventional Resin | 38 | 53 | SDR flowable (DentsplySirona, Konstanz, Germany) + Ceram X mono (DentsplySirona, Konstanz, Germany) | Two-step Bulk (4 mm + 2 mm) | |||||||||||||
| Yazici et al. [18] | 2017 | Turkey | RCT split mouth double-blind | 50 (24/26) | 104 | (24–55) | 3 years | Conventional resin | 50 | 52 | Class II | Premolar and Molar | Modified US Public Health Service | Etching and rising | Adper Single Bond 2 (3M ESPE, St Paul, USA) | Filtek Ultimate (3M ESPE, St Paul, USA) | Incremental |
| Bulk resin | 50 | 52 | Excite F (Ivoclar Vivadent, Schaan, Liechtenstein) | Tetric EvoCeram Bulk Fill (Ivoclar Vivadent, Schaan, Liechtenstein) | Bulk | ||||||||||||
| van Dijken et al. [19] | 2016 | Sweden and Denmark | RCT split mouth double-blind | 86 (44/42) | 200 | 52.4 (20–86) | 5 years | Conventional resin | 86 | 100 | Class I and II | Premolar and Molar | Modified US Public Health Service | Self-etch | XenoV (Dentsply/DeTrey, Konstanz, Germany) | Ceram X mono (Dentsply/DeTrey, Konstanz, Germany) | Incremental |
| Bulk Resin + Conventional Resin | 86 | 100 | SDR flowable (Dentsply/DeTrey, Konstanz, Germany) + Ceram X mono (Dentsply/DeTrey, Konstanz, Germany) | Two-step Bulk (4 mm + 2 mm) | |||||||||||||
| Arhun et al. [20] | 2010 | Turkey | RCT split mouth | 31(10/21) | 82 | 36 (16–60) | 2 years | Conventional resin | 31 | 41 | Class I and II | Premolar and Molar | Modified US Public Health Service | Self-etch | Futurabond NR (Voco GmbH, Cuxhaven, Germany) | Grandio (Voco GmbH, Cuxhaven, Germany) | Incremental |
| Bulk resin | 31 | 41 | Xeno III (Dentsply Caulk, Milford, DE, USA) | QuiXfil (Dentsply Caulk, Milford, DE, USA) | Incremental | ||||||||||||
| Manhart et al. [21] | 2010 | Germany | RCT split mouth | 43 | 96 | 44.3 (19–67) | 4 years | Conventional resin | 43 | 50 | Class I and II | Molar | Modified US Public Health Service | Etching and rising - 37% phosphoric acid | Syntac classic (Ivoclar Vivadent, Schaan, Liechtenstein) | Tetric Ceram (Ivoclar Vivadent, Schaan, Liechtenstein) | Incremental |
| Bulk resin | 43 | 46 | Self-etch | Xeno III (Dentsply De Trey, Konstanz, Germany) | QuiXfil (Dentsply De Trey, Konstanz, Germany) | Bulk |
| Author(s) | Clinical Parameters | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Absence of Fractures | Absence of Discoloration or Marginal Staining | Adequate Marginal Adaptation | Absence of Post-Operative Sensitivity | Absence of Secondary Caries | Adequate Color, Stability, and Translucency | Proper Surface Texture | Proper Anatomical Form | Adequate Tooth Integrity/No Wear | Adequate Restoration Integrity | Proper Occlusion | Absence of Inflammation | Adequate Point of Contact | |
| Akman et al. (2020) [14] | 28/34 | 30/34 | 28/34 | 34/34 | 34/34 | 34/34 | NR | 34/34 | NR | NR | NR | NR | NR |
| 34/34 | 32/34 | 33/34 | 34/34 | 34/34 | 34/34 | NR | 34/34 | NR | NR | NR | NR | NR | |
| 34/34 | 32/34 | 33/34 | 34/34 | 34/34 | 34/34 | NR | 34/34 | NR | NR | NR | NR | NR | |
| 32/32 | 30/32 | 31/32 | 32/32 | 32/32 | 32/32 | NR | 32/32 | NR | NR | NR | NR | NR | |
| Balkaya et al. (2020) [15] | 32/32 | 31/32 | 23/32 | 32/32 | 32/32 | 32/32 | 30/32 | 32/32 | NR | NR | NR | NR | 32/32 |
| 31/31 | 29/31 | 27/31 | 31/31 | 31/31 | 31/31 | 31/31 | 31/31 | NR | NR | NR | NR | 31/31 | |
| 15/21 | 20/21 | 10/21 | 21/21 | 21/21 | 5/21 | 11/21 | 15/21 | NR | NR | NR | NR | 14/21 | |
| Correia et al. (2020) [22] | 33/33 | 29/33 | 32/33 | 33/33 | 33/33 | NR | 32/33 | 33/33 | NR | NR | NR | NR | NR |
| 33/34 | 29/34 | 33/34 | 31/34 | 33/34 | NR | 32/34 | 33/34 | NR | NR | NR | NR | NR | |
| 34/34 | 25/34 | 34/34 | 32/34 | 34/34 | NR | 32/34 | 34/34 | NR | NR | NR | NR | NR | |
| 34/35 | 31/35 | 33/35 | 32/35 | 34/35 | NR | 33/35 | 34/35 | NR | NR | NR | NR | NR | |
| Frascino et al. (2020) [23] | 50/53 | 39/53 | 38/53 | NR | 53/53 | 45/53 | 51/53 | 52/53 | 52/53 | 45/53 | NR | NR | NR |
| 52/53 | 39/53 | 39/53 | NR | 52/53 | 49/53 | 50/53 | 52/53 | 52/53 | 35/53 | NR | NR | NR | |
| 51/53 | 41/53 | 44/53 | NR | 52/53 | 51/53 | 49/53 | 53/53 | 52/53 | 50/53 | NR | NR | NR | |
| Al-Sheikh (2019) [24] | 37/38 | 37/37 | 37/37 | 36/37 | 37/37 | 37/37 | 37/37 | NR | NR | NR | NR | 37/37 | NR |
| 37/39 | 35/37 | 37/37 | 36/37 | 36/37 | 37/37 | 36/37 | NR | NR | NR | NR | 37/37 | NR | |
| Canali et al. (2019) [25] | 42/43 | 42/42 | 26/42 | 32/42 | 42/42 | NR | 30/42 | 36/42 | NR | NR | NR | NR | NR |
| 46/46 | 46/46 | 28/46 | 29/46 | 46/46 | NR | 43/46 | 40/46 | NR | NR | NR | NR | NR | |
| Heck et al. (2018) [26] | 29/30 | 20/30 | 22/30 | 30/30 | 27/30 | 30/30 | 29/30 | 30/30 | 27/30 | 30/30 | 30/30 | NR | NR |
| 22/26 | 12/26 | 14/26 | 24/26 | 24/26 | 25/26 | 24/26 | 25/26 | 21/26 | 19/26 | 24/26 | NR | NR | |
| Oter et al. (2018) [27] | 50/50 | 43/50 | 47/50 | 50/50 | 50/50 | 45/50 | 48/50 | 45/50 | NR | NR | NR | NR | NR |
| 50/50 | 37/50 | 45/50 | 50/50 | 50/50 | 44/50 | 49/50 | 45/50 | NR | NR | NR | NR | NR | |
| Atabek et al. (2017) [28] | 30/30 | 29/30 | 29/30 | 30/30 | 30/30 | 28/30 | 28/30 | 30/30 | NR | NR | NR | NR | NR |
| 30/30 | 29/30 | 30/30 | 30/30 | 30/30 | 29/30 | 29/30 | 30/30 | NR | NR | NR | NR | NR | |
| Bayraktar et al. (2017) [29] | 43/43 | 42/43 | 43/43 | 43/43 | 42/43 | 43/43 | NR | 43/43 | NR | NR | NR | NR | NR |
| 42/43 | 41/43 | 40/43 | 42/43 | 41/43 | 42/43 | NR | 40/43 | NR | NR | NR | NR | NR | |
| 43/43 | 42/43 | 42/43 | 43/43 | 41/43 | 43/43 | NR | 42/43 | NR | NR | NR | NR | NR | |
| 43/43 | 43/43 | 43/43 | 43/43 | 43/43 | 43/43 | NR | 43/43 | NR | NR | NR | NR | NR | |
| Colak et al. (2017) [16] | 35/35 | 31/35 | 34/35 | 35/35 | 35/35 | 35/35 | NR | 35/35 | NR | NR | NR | NR | NR |
| 35/35 | 34/35 | 35/35 | 35/35 | 35/35 | 34/35 | NR | 35/35 | NR | NR | NR | NR | NR | |
| van Dijken et al. (2017) [17] | 46/49 | 46/49 | 36/49 | 49/49 | 49/49 | 6/49 | 46/49 | 42/49 | NR | NR | NR | NR | NR |
| 46/49 | 44/49 | 39/49 | 49/49 | 48/49 | 2/49 | 45/49 | 43/49 | NR | NR | NR | NR | NR | |
| Yazici et al. (2017) [18] | 40/40 | 32/40 | 30/40 | 40/40 | NR | 38/40 | 38/40 | NR | NR | NR | NR | NR | NR |
| 41/41 | 39/41 | 37/41 | 41/41 | NR | 41/41 | 41/41 | NR | NR | NR | NR | NR | NR | |
| van Dijken et al. (2016) [19] | 86/91 | 73/91 | 79/91 | 91/91 | 89/91 | 36/91 | 85/91 | 80/91 | NR | NR | NR | NR | NR |
| 89/92 | 68/92 | 69/92 | 92/92 | 90/92 | 35/92 | 83/92 | 84/92 | NR | NR | NR | NR | NR | |
| Arhun et al. (2010) [20] | 35/37 | 35/35 | 30/35 | 35/35 | 35/35 | 32/35 | 26/35 | NR | NR | NR | NR | NR | NR |
| 35/37 | 33/35 | 31/35 | 35/35 | 35/35 | 35/35 | 34/35 | NR | NR | NR | NR | NR | NR | |
| Manhart et al. (2010) [21] | 45/46 | 34/46 | 41/46 | 46/46 | 46/46 | 45/46 | 44/46 | 45/46 | 44/46 | 45/46 | 45/46 | NR | NR |
| 34/37 | 26/37 | 33/37 | 36/37 | 37/37 | 37/37 | 35/37 | 36/37 | 32/37 | 34/37 | 35/37 | NR | NR | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arbildo-Vega, H.I.; Lapinska, B.; Panda, S.; Lamas-Lara, C.; Khan, A.S.; Lukomska-Szymanska, M. Clinical Effectiveness of Bulk-Fill and Conventional Resin Composite Restorations: Systematic Review and Meta-Analysis. Polymers 2020, 12, 1786. https://0-doi-org.brum.beds.ac.uk/10.3390/polym12081786
Arbildo-Vega HI, Lapinska B, Panda S, Lamas-Lara C, Khan AS, Lukomska-Szymanska M. Clinical Effectiveness of Bulk-Fill and Conventional Resin Composite Restorations: Systematic Review and Meta-Analysis. Polymers. 2020; 12(8):1786. https://0-doi-org.brum.beds.ac.uk/10.3390/polym12081786
Chicago/Turabian StyleArbildo-Vega, Heber Isac, Barbara Lapinska, Saurav Panda, César Lamas-Lara, Abdul Samad Khan, and Monika Lukomska-Szymanska. 2020. "Clinical Effectiveness of Bulk-Fill and Conventional Resin Composite Restorations: Systematic Review and Meta-Analysis" Polymers 12, no. 8: 1786. https://0-doi-org.brum.beds.ac.uk/10.3390/polym12081786