Monoclonal Antibody Combinations Prevent Serotype A and Serotype B Inhalational Botulism in a Guinea Pig Model

 and
and
Abstract
:1. Introduction
2. Results
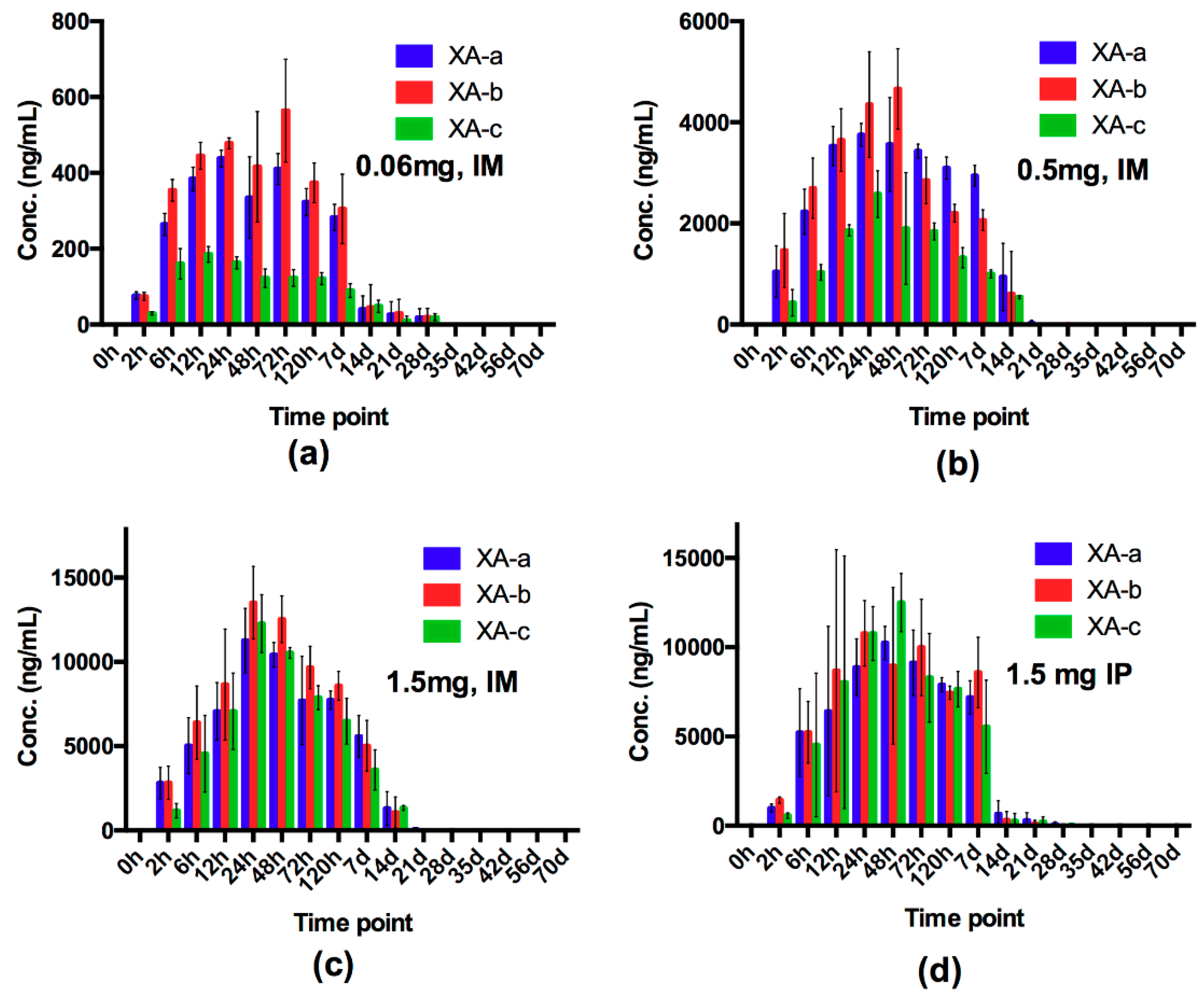
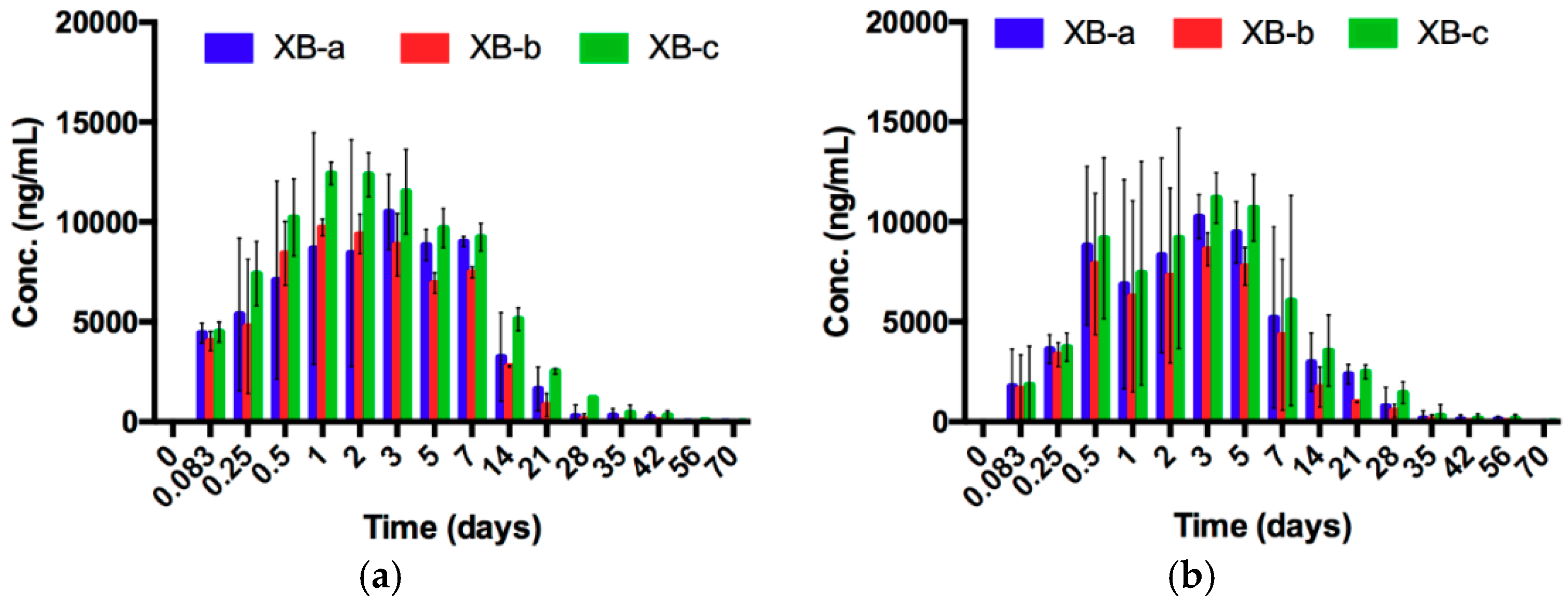
2.1. Evaluation of Dose and Route of Administration on Individual mAb Pharmacokinetics and NTM-1631 and NTM-1632 Neutralizing Antibody Concentration (NAC) in Guinea Pigs
2.2. NTM-1631 and NTM-1632 Protect Guinea Pigs against Lethal Aerosol Challenge with BoNT/A and BoNT/B
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Monoclonal Antibodies
5.2. Challenge Material
5.3. Control Samples
5.4. Pharmacokinetics
5.5. Animal Challenge Studies
5.6. Aerosol Exposure System
5.7. Measurement of BoNT Challenge Concentrations
5.8. Measurement of Neutralizing Antibody Concentration
5.9. Statistical Methods
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Gill, M.D. Bacterial toxins: A table of lethal amounts. Microbiol. Rev. 1982, 46, 86–94. [Google Scholar]
- Schechter, R.; Arnon, S.S. Extreme potency of botulinum toxin. Lancet 2000, 355, 237–238. [Google Scholar] [CrossRef]
- Rossetto, O.; Pirazzini, M.; Montecucco, C. Botulinum neurotoxins: Genetic, structural and mechanistic insights. Nat. Rev. Microbiol. 2014, 12, 535. [Google Scholar] [CrossRef] [PubMed]
- Pirazzini, M.; Rossetto, O.; Eleopra, R.; Montecucco, C. Botulinum Neurotoxins: Biology, Pharmacology, and Toxicology. Pharm. Rev. 2017, 69, 200–235. [Google Scholar] [PubMed]
- Montecucco, C.; Rossetto, O.; Schiavo, G. Presynaptic receptor arrays for clostridial neurotoxins. Trends Microbiol. 2004, 12, 442–446. [Google Scholar] [CrossRef]
- Dong, M.; Yeh, F.; Tepp, W.H.; Dean, C.; Johnson, E.A.; Janz, R.; Chapman, E.R. SV2 is the protein receptor for botulinum neurotoxin A. Science 2006, 312, 592–596. [Google Scholar] [CrossRef]
- Fischer, A.; Montal, M. Single molecule detection of intermediates during botulinum neurotoxin translocation across membranes. Proc. Natl. Acad. Sci. USA 2007, 104, 10447–10452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, K.-H.; Guo, Z.; Krez, N.; Matsui, T.; Perry, K.; Weisemann, J.; Rummel, A.; Bowen, M.E.; Jin, R. A viral-fusion-peptide-like molecular switch drives membrane insertion of botulinum neurotoxin A1. Nat. Commun. 2018, 9, 5367. [Google Scholar] [CrossRef] [PubMed]
- Fischer, A.; Montal, M. Molecular dissection of botulinum neurotoxin reveals interdomain chaperone function. Toxicon Off. J. Int. Soc. Toxinol. 2013, 75, 101–107. [Google Scholar] [Green Version]
- Pantano, S.; Montecucco, C. The blockade of the neurotransmitter release apparatus by botulinum neurotoxins. Cell. Mol. Life Sci. 2014, 71, 793–811. [Google Scholar]
- Lacy, D.B.; Stevens, R.C. Sequence homology and structural analysis of the Clostridial neurotxins. J. Mol. Biol. 1999, 291, 1091–1104. [Google Scholar] [CrossRef] [PubMed]
- Moller, V.; Scheibel, I. Preliminary report on the isolation of an apparently new type of CI. botulinum. Acta Pathol. Microbiol. Scand. 1960, 48, 80. [Google Scholar] [CrossRef]
- Gimenez, D.; Ciccarelli, A. Another type of Clostridium botulinum. Zent. Fur Bakteriol. Parasitenkd. Infekt. Und Hyg. Abt. I (Orig.) 1970, 215, 221–224. [Google Scholar]
- Botulism in the United States, 1899–1998. Handbook for Epidemiologists, Clinicians,and Laboratory Workers; U.S. Department of Health and Human Services, P.H.S., Centers for Disease Control: Atlanta, Georgia, 1998. Available online: https://www.cdc.gov/botulism/resources.html (accessed on 3 April 2019).
- Dembek, Z.F.; Smith, L.A.; Rusnak, J.M. Botulism: Cause, effects, diagnosis, clinical and laboratory identification, and treatment modalities. Disaster Med. Public Health Prep. 2007, 1, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Sobel, J. Botulism. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2005, 41, 1167–1173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chertow, D.S.; Tan, E.T.; Maslanka, S.E.; Schulte, J.; Bresnitz, E.A.; Weisman, R.S.; Bernstein, J.; Marcus, S.M.; Kumar, S.; Malecki, J. Botulism in 4 adults following cosmetic injections with an unlicensed, highly concentrated botulinum preparation. JAMA 2006, 296, 2476–2479. [Google Scholar] [CrossRef] [PubMed]
- Bai, L.; Peng, X.; Liu, Y.; Sun, Y.; Wang, X.; Wang, X.; Lin, G.; Zhang, P.; Wan, K.; Qiu, Z. Clinical analysis of 86 botulism cases caused by cosmetic injection of botulinum toxin (BoNT). Medicine 2018, 97, e10659. [Google Scholar] [CrossRef]
- Park, J.-B.; Simpson, L.L. Inhalational poisoning by botulinum toxin and inhalation vaccination with its heavy-chain component. Infect. Immun. 2003, 71, 1147–1154. [Google Scholar] [CrossRef]
- Sanford, D.C.; Barnewall, R.E.; Vassar, M.L.; Niemuth, N.; Metcalfe, K.; House, R.V.; Henderson, I.; Shearer, J.D. Inhalational botulism in rhesus macaques exposed to botulinum neurotoxin complex serotypes A1 and B1. Clin. Vaccine Immunol. 2010, 17, 1293–1304. [Google Scholar] [CrossRef]
- Holzer, V. Botulism from inhalation [in German]. Med. Klin 1962, 57, 1735–1738. [Google Scholar]
- Arnon, S.S.; Schechter, R.; Inglesby, T.V.; Henderson, D.A.; Bartlett, J.G.; Ascher, M.S.; Eitzen, E.; Fine, A.D.; Hauer, J.; Layton, M.; et al. Botulinum toxin as a biological weapon: Medical and public health management. JAMA 2001, 285, 1059–1070. [Google Scholar] [CrossRef]
- Hibbs, R.G.; Weber, J.T.; Corwin, A.; Allos, B.M.; Abd el Rehim, M.S.; Sharkawy, S.E.; Sarn, J.E.; McKee, K.T., Jr. Experience with the use of an investigational F(ab’)2 heptavalent botulism immune globulin of equine origin during an outbreak of type E botulism in Egypt. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 1996, 23, 337–340. [Google Scholar] [CrossRef]
- Jalava, K.; Selby, K.; Pihlajasaari, A.; Kolho, E.; Dahlsten, E.; Forss, N.; Backlund, T.; Korkeala, H.; Honkanen-Buzalski, T.; Hulkko, T.; et al. Two cases of food-borne botulism in Finland caused by conserved olives, October 2011. Euro Surveill. Bull. Eur. Sur Les Mal. Transm. = Eur. Commun. Dis. Bull. 2011, 16, 20034. [Google Scholar] [CrossRef]
- Pingeon, J.M.; Vanbockstael, C.; Popoff, M.R.; King, L.A.; Deschamps, B.; Pradel, G.; Dupont, H.; Spanjaard, A.; Houdard, A.; Mazuet, C.; et al. Two outbreaks of botulism associated with consumption of green olive paste, France, September 2011. Euro Surveill. Bull. Eur. Sur Les Mal. Transm. = Eur. Commun. Dis. Bull. 2011, 16, 20035. [Google Scholar] [CrossRef]
- Gupta, A.; Sumner, C.; Castor, M.; Maslanka, S.; Sobel, J. Adult botulism type F in the United States, 1981–2002. Neurology 2005, 65, 1694–1700. [Google Scholar] [CrossRef] [PubMed]
- Froude, J.W.; Stiles, B.; Pelat, T.; Thullier, P. Antibodies for biodefense. mAbs 2011, 3, 517–527. [Google Scholar] [CrossRef] [Green Version]
- Bozheyeva, G.; Kunakbayev, Y.; Yeleukenov, D. Former Soviet Biological Weapons Facilities in Kazakhstan: Past, Present, and Future; Center for Nonproliferation Studies, Monterey Institute of International Studies: Monterey, CA, USA, 1999; pp. 1–20, Occasional paper No. 1, 1999. [Google Scholar]
- United Nations Security Council. Tenth Report of the Executive Committee of the Special Commision Established by the Secretary-General Pursuant to Paragraph 9(b)(I) of Security Council Resolution 687 (1991), and Paragraph 3 of Resolution 699 (1991) on the Activities of the Special Commision; United Nations Security Council: New York, NY, USA, 1995; S/1995/1038. [Google Scholar]
- Lim, E.C.; Seet, R.C. Use of botulinum toxin in the neurology clinic. Nat. Reviews. Neurol. 2010, 6, 624–636. [Google Scholar] [CrossRef] [PubMed]
- Coleman, K.; Zilinskas, R.A. Fake botox, real threat. Sci. Am. 2010, 302, 84–89. [Google Scholar] [CrossRef]
- Siegel, L.S. Human immune response to botulinum pentavalent (ABCDE) toxoid determined by a neutralization test and by an enzyme-linked immunosorbent assay. J. Clin. Microbiol. 1988, 26, 2351–2356. [Google Scholar]
- CDC. Notice of CDC’s discontinuation of investigational pentavalent (ABCDE) botulinum toxoid vaccine for workers at risk for occupational exposure to botulinum toxins. Mmwr. Morb. Mortal. Wkly. Rep. 2011, 60, 1454. [Google Scholar]
- Webb, R.P.; Smith, L.A. What next for botulism vaccine development? Expert Rev. Vaccines 2013, 12, 481–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webb, R.P.; Smith, T.J.; Smith, L.A.; Wright, P.M.; Guernieri, R.L.; Brown, J.L.; Skerry, J.C. Recombinant botulinum neurotoxin Hc subunit (BoNT Hc) and catalytically inactive Clostridium botulinum holoproteins (ciBoNT HPs) as vaccine candidates for the prevention of botulism. Toxins 2017, 9, 269. [Google Scholar] [CrossRef] [PubMed]
- Hart, M.K.; Saviolakis, G.A.; Welkos, S.L.; House, R.V. Advanced Development of the rF1V and rBV A/B Vaccines: Progress and Challenges. Adv. Prev. Med. 2012, 2012, 731604. [Google Scholar] [CrossRef] [PubMed]
- Arnon, S.S.; Schechter, R.; Maslanka, S.E.; Jewell, N.P.; Hatheway, C.L. Human botulism immune globulin for the treatment of infant botulism. N. Engl. J. Med. 2006, 354, 462–471. [Google Scholar] [CrossRef] [PubMed]
- Kodihalli, S.; Emanuel, A.; Takla, T.; Hua, Y.; Hobbs, C.; LeClaire, R.; O’Donnell, D.C. Therapeutic efficacy of equine botulism antitoxin in Rhesus macaques. PLoS ONE 2017, 12, e0186892. [Google Scholar] [CrossRef]
- Yu, P.A.; Lin, N.H.; Mahon, B.E.; Sobel, J.; Yu, Y.; Mody, R.K.; Gu, W.; Clements, J.; Kim, H.-J.; Rao, A.K. Safety and improved clinical outcomes in patients treated with new equine-derived heptavalent botulinum antitoxin. Clin. Infect. Dis. 2017, 66, S57–S64. [Google Scholar] [CrossRef]
- Payne, J.R.; Khouri, J.M.; Jewell, N.P.; Arnon, S.S. Efficacy of Human Botulism Immune Globulin for the Treatment of Infant Botulism: The First 12 Years Post Licensure. J. Pediatrics 2018, 193, 172–177. [Google Scholar] [CrossRef]
- Cangene Corporation. BAT® [Botulism Antitoxin Heptavalent (A, B, C, D, E, F, G)-(Equine)] Sterile Solution for Injection. Available online: https://www.fda.gov/downloads/.../UCM345147.pdf (accessed on 11 October 2017).
- Fan, Y.; Garcia-Rodriguez, C.; Lou, J.; Wen, W.; Conrad, F.; Zhai, W.; Smith, T.J.; Smith, L.A.; Marks, J.D. A three monoclonal antibody combination potently neutralizes multiple botulinum neurotoxin serotype F subtypes. PLoS ONE 2017, 12, e0174187. [Google Scholar] [CrossRef]
- Garcia-Rodriguez, C.; Razai, A.; Geren, I.N.; Lou, J.; Conrad, F.; Wen, W.H.; Farr-Jones, S.; Smith, T.J.; Brown, J.L.; Skerry, J.C.; et al. A Three Monoclonal Antibody Combination Potently Neutralizes Multiple Botulinum Neurotoxin Serotype E Subtypes. Toxins 2018, 10, 105. [Google Scholar] [CrossRef]
- Meng, Q.; Garcia-Rodriguez, C.; Manzanarez, G.; Silberg, M.; Conrad, F.; Bettencourt, J.; Pan, X.; Breece, T.; To, R.; Li, M. Engineered domain-based assays to identify individual antibodies in oligoclonal combinations targeting the same protein. Anal. Biochem. 2012, 430, 141–150. [Google Scholar] [CrossRef]
- Meng, Q.; Li, M.; Silberg, M.A.; Conrad, F.; Bettencourt, J.; To, R.; Huang, C.; Ma, J.; Meyer, K.; Shimizu, R.; et al. Domain-based assays of individual antibody concentrations in an oligoclonal combination targeting a single protein. Anal. Biochem. 2012, 421, 351–361. [Google Scholar] [CrossRef]
- Nowakowski, A.; Wang, C.; Powers, D.; Amersdorfer, P.; Smith, T.; Montgomery, V.; Sheridan, R.; Blake, R.; Smith, L.; Marks, J. Potent neutralization of botulinum neurotoxin by recombinant oligoclonal antibody. Proc. Natl. Acad. Sci. USA 2002, 99, 11346–11350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nayak, S.U.; Griffiss, J.M.; McKenzie, R.; Fuchs, E.J.; Jurao, R.A.; An, A.T.; Ahene, A.; Tomic, M.; Hendrix, C.W.; Zenilman, J.M. Safety and pharmacokinetics of XOMA 3AB, a novel mixture of three monoclonal antibodies against botulinum toxin A. Antimicrob. Agents Chemother. 2014, 58, 5047–5053. [Google Scholar] [CrossRef]
- Byrne, M.P.; Smith, L.A. Development of vaccines for prevention of botulism. Biochimie 2000, 82, 955–966. [Google Scholar] [CrossRef] [Green Version]
- Przedpelski, A.; Tepp, W.H.; Kroken, A.R.; Fu, Z.; Kim, J.J.; Johnson, E.A.; Barbieri, J.T. Enhancing the protective immune response against botulism. Infect. Immun. 2013, 81, 2638–2644. [Google Scholar] [CrossRef] [PubMed]
- Reames, H.; Kadull, P.; Housewright, R.; Wilson, J. Studies on Botulinum Toxoids, Types A and B. III. Immunization of Man. J. Immunol. 1947, 55, 309–324. [Google Scholar]
- Fiock, M.A.; Devine, L.F.; Gearinger, N.F.; Duff, J.T.; Wright, G.G.; Kadull, P.J. Studies on Immunity to Toxins of Clostridium Botulinum: VIII. Immunological Response of Man to Purified Bivalent AB Botulinum Toxoid. J. Immunol. 1962, 88, 277–283. [Google Scholar]
- Ellis, R.J. Immunobiologic Agents and Drugs Available from the Centers for Disease Control: Descriptions, Recommendations, Adverse Reactions, and Serologic Response; U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control: Atlanta, GA, USA, 1982.
- Lou, J.; Wen, W.; Conrad, F.; Meng, Q.; Dong, J.; Sun, Z.; Garcia-Rodriguez, C.; Farr-Jones, S.; Cheng, L.W.; Henderson, T.D. A Single Tri-Epitopic Antibody Virtually Recapitulates the Potency of a Combination of Three Monoclonal Antibodies in Neutralization of Botulinum Neurotoxin Serotype A. Toxins 2018, 10, 84. [Google Scholar] [CrossRef] [PubMed]
- Kaplon, H.; Reichert, J.M. Antibodies to Watch in 2018. mAbs 2018, 10, 183–203. [Google Scholar] [CrossRef]
- Fagan, R.P.; Neil, K.P.; Sasich, R.; Luquez, C.; Asaad, H.; Maslanka, S.; Khalil, W. Initial recovery and rebound of type f intestinal colonization botulism after administration of investigational heptavalent botulinum antitoxin. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2011, 53, e125–e128. [Google Scholar] [CrossRef]
- Harding, F.A.; Stickler, M.M.; Razo, J.; DuBridge, R. The immunogenicity of humanized and fully human antibodies: Residual immunogenicity resides in the CDR regions. mAbs 2010, 2, 256–265. [Google Scholar] [CrossRef]
- Hansel, T.T.; Kropshofer, H.; Singer, T.; Mitchell, J.A.; George, A.J. The safety and side effects of monoclonal antibodies. Nat. Rev. Drug Discov. 2010, 9, 325. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.J.; Lou, J.; Geren, I.N.; Forsyth, C.M.; Tsai, R.; Laporte, S.L.; Tepp, W.H.; Bradshaw, M.; Johnson, E.A.; Smith, L.A.; et al. Sequence variation within botulinum neurotoxin serotypes impacts antibody binding and neutralization. Infect. Immun. 2005, 73, 5450–5457. [Google Scholar] [CrossRef] [PubMed]
- Cardella, M.A. Botulism: Proceedings of a Symposium; Cincinnati, O.H., Lewis, K.H., Cassel, K., Eds.; U.S. Department of Health, Education, Welfare, Public Service: Cincinnati, OH, USA, 1964; pp. 113–130.
- Gelzleichter, T.R.; Myers, M.A.; Menton, R.G.; Niemuth, N.A.; Matthews, M.C.; Langford, M.J. Protection against botulinum toxins provided by passive immunization with botulinum human immune globulin: Evaluation using an inhalation model. J. Appl. Toxicol. 1999, 19, S35–S38. [Google Scholar] [CrossRef]
- Guyton, A.C. Measurement of the respiratory volumes of laboratory animals. Am. J. Physiol. 1947, 150, 70–77. [Google Scholar] [CrossRef]
- Finney, D.J. Probit Analysis, 3rd ed.; Cambridge University Press: Cambridge, UK, 1971. [Google Scholar]
- Hatheway, C.; Dang, C. Immunogenicity of the neurotoxins of Clostridium botulinum. Ther. Botulinum Toxin 1994, 25, 93–107. [Google Scholar]
- Khouri, J.M.; Motter, R.N.; Arnon, S.S. Safety and immunogenicity of investigational recombinant botulinum vaccine, rBV A/B, in volunteers with pre-existing botulinum toxoid immunity. Vaccine 2018, 36, 2041–2048. [Google Scholar] [CrossRef]
- Arnon, S.S. Creation and development of the public service orphan drug Human Botulism Immune Globulin. Pediatrics 2007, 119, 785–789. [Google Scholar] [CrossRef]
- Shearer, J.D.; Vassar, M.L.; Swiderski, W.; Metcalfe, K.; Niemuth, N.; Henderson, I. Botulinum neurotoxin neutralizing activity of immune globulin (IG) purified from clinical volunteers vaccinated with recombinant botulinum vaccine (rBV A/B). Vaccine 2010, 28, 7313–7318. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Study 1 | Study 2 | |||
|---|---|---|---|---|---|
| BoNT/A1 | BoNT/B1 | BoNT/A1 | BoNT/B1 | ||
| Guinea Pig LD50 delivered | Target | 10 | 10 | 100 | 100 |
| Actual | 55 | 8 | 93 | 116 | |
| Inhaled Dose (MIPLD50/animal) | Actual | 8.73 × 103 | 1.52 × 103 | 1.47 × 104 | 2.33 × 104 |
| Total accumulated tidal volume (TATV) (L) | Actual | 2.32 | 2.38 | 2.43 | 2.40 |
| Impinger Concentration (MIPLD50/mL) * | Actual | 1.39 × 104 | 2.34 × 103 | 2.26 × 104 | 3.54 × 104 |
| Nebulizer Suspension Concentration (MIPLD50/mL) * | Actual | 1.04 × 106 | 4.67 × 105 | 2.00 × 106 | 4.77 × 106 |
| Aerosol Conc. (MIPLD50/L) * | Actual | 3.76 × 103 | 6.39 × 102 | 6.07 × 103 | 9.69 × 103 |
| Mass median aerodynamic diameter (µm) | Actual | 1.16 | 1.05 | 1.15 | 1.12 |
| Exposure Time (min) | Actual | 12.00 | 12.00 | 12.00 | 12.00 |
| # Animals/Exposure | Actual | 20 | 20 | 20 | 20 |
| Mean Animal Weight (g) | Actual | 417 | 431 | 441 | 435 |
| Treatment Group | Study | Geometric Mean NAC (U/mL) | 95% Confidence Bounds |
|---|---|---|---|
| 1-PBS | 1 | NM | NA |
| 2 | NM | NA | |
| 2-BoNT/A1 | 1 | 7.7 | (4.5, 13.1) |
| 2 | 9.7 | (1.1, 83) | |
| 1-PBS | 1 | NM | NA |
| 2 | NM | NA | |
| 2-BoNT/B1 | 1 | 21.6 | (9.9, 47.3) |
| 2 | 19.5 | (5.7, 65.6) |
| Treatment | mAb Dose (mg) | BoNT Challenge Serotype | Average Time to Death (h) | Average Weight Gain after 14 Days (g) | Mortality (Number Dead/Total Number Animals) |
|---|---|---|---|---|---|
| First Challenge Experiment | |||||
| PBS | 0 | BoNT/A1 (55 LD50) | 15 | N/A | 10/10 |
| NTM-1631 | 1.5 | N/A | 164.67 | 0/10 | |
| PBS | 0 | BoNT/B1 (8 LD50) | 24 | N/A | 10/10 |
| NTM-1632 | 1.5 | N/A | 178.88 | 0/10 | |
| Second Challenge Experiment | |||||
| PBS | 0 | BoNT/A1 (93 LD50) | 13 | N/A | 10/10 |
| NTM-1631 | 1.5 | N/A | 100.74 | 0/10 | |
| PBS | 0 | BoNT/B1 (116 LD50) | 14 | N/A | 10/10 |
| NTM-1632 | 1.5 | N/A | 97.17 | 0/10 | |
| Treatment Group | mAb Concentration (mg) | Number of Animals Per Group * | Challenge Material |
|---|---|---|---|
| PBS | 0 | 13 | BoNT/A1 |
| NTM-1631 | 1.5 | 13 | BoNT/A1 |
| PBS | 0 | 13 | BoNT/B1 |
| NTM-1632 | 1.5 | 13 | BoNT/B1 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomic, M.T.; Espinoza, Y.; Martinez, Z.; Pham, K.; Cobb, R.R.; Snow, D.M.; Earnhart, C.G.; Pals, T.; Syar, E.S.; Niemuth, N.; et al. Monoclonal Antibody Combinations Prevent Serotype A and Serotype B Inhalational Botulism in a Guinea Pig Model. Toxins 2019, 11, 208. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11040208
Tomic MT, Espinoza Y, Martinez Z, Pham K, Cobb RR, Snow DM, Earnhart CG, Pals T, Syar ES, Niemuth N, et al. Monoclonal Antibody Combinations Prevent Serotype A and Serotype B Inhalational Botulism in a Guinea Pig Model. Toxins. 2019; 11(4):208. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11040208
Chicago/Turabian StyleTomic, Milan T., Yero Espinoza, Zachary Martinez, Khanh Pham, Ronald R. Cobb, Doris M. Snow, Christopher G. Earnhart, Traci Pals, Emily S. Syar, Nancy Niemuth, and et al. 2019. "Monoclonal Antibody Combinations Prevent Serotype A and Serotype B Inhalational Botulism in a Guinea Pig Model" Toxins 11, no. 4: 208. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11040208