Association between Serum Indoxyl Sulfate Levels and Endothelial Function in Non-Dialysis Chronic Kidney Disease

 , ,
, , 

Abstract
:1. Introduction
2. Results
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Participants
5.2. Biochemical Analysis and CKD Stage
5.3. Determination of Serum IS Levels
5.4. Endothelial Function Measurements
5.5. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stevens, P.E.; Levin, A. Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group, M. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Jono, S.; McKee, M.D.; Murry, C.E.; Shioi, A.; Nishizawa, Y.; Mori, K.; Morii, H.; Giachelli, C.M. Phosphate regulation of vascular smooth muscle cell calcification. Circ. Res. 2000, 87, e10–e17. [Google Scholar] [CrossRef] [PubMed]
- Joannides, R.; Bakkali, E.H.; Le Roy, F.; Rivault, O.; Godin, M.; Moore, N.; Fillastre, J.P.; Thuillez, C. Altered flow-dependent vasodilatation of conduit arteries in maintenance haemodialysis. Nephrol. Dial. Transplant. 1997, 12, 2623–2628. [Google Scholar] [CrossRef] [PubMed]
- Thambyrajah, J.; Landray, M.J.; McGlynn, F.J.; Jones, H.J.; Wheeler, D.C.; Townend, J.N. Abnormalities of endothelial function in patients with predialysis renal failure. Heart 2000, 83, 205–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Guldener, C.; Janssen, M.J.; Lambert, J.; Steyn, M.; Donker, A.J.; Stehouwer, C.D. Endothelium-dependent vasodilatation is impaired in peritoneal dialysis patients. Nephrol. Dial. Transplant. 1998, 13, 1782–1786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopel, T.; Kaufman, J.S.; Hamburg, N.; Sampalis, J.S.; Vita, J.A.; Dember, L.M. Endothelium-dependent and -independent vascular function in advanced chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2017, 12, 1588–1594. [Google Scholar] [CrossRef]
- Gokce, N.; Keaney, J.F., Jr.; Hunter, L.M.; Watkins, M.T.; Nedeljkovic, Z.S.; Menzoian, J.O.; Vita, J.A. Predictive value of noninvasively determined endothelial dysfunction for long-term cardiovascular events in patients with peripheral vascular disease. J. Am. Coll. Cardiol. 2003, 41, 1769–1775. [Google Scholar] [CrossRef]
- Hirata, Y.; Sugiyama, S.; Yamamoto, E.; Matsuzawa, Y.; Akiyama, E.; Kusaka, H.; Fujisue, K.; Kurokawa, H.; Matsubara, J.; Sugamura, K.; et al. Endothelial function and cardiovascular events in chronic kidney disease. Int. J. Cardiol. 2014, 173, 481–486. [Google Scholar] [CrossRef]
- Ghiadoni, L.; Cupisti, A.; Huang, Y.; Mattei, P.; Cardinal, H.; Favilla, S.; Rindi, P.; Barsotti, G.; Taddei, S.; Salvetti, A. Endothelial dysfunction and oxidative stress in chronic renal failure. J. Nephrol. 2004, 17, 512–519. [Google Scholar]
- Recio-Mayoral, A.; Banerjee, D.; Streather, C.; Kaski, J.C. Endothelial dysfunction, inflammation and atherosclerosis in chronic kidney disease—A cross-sectional study of predialysis, dialysis and kidney-transplantation patients. Atherosclerosis 2011, 216, 446–451. [Google Scholar] [CrossRef]
- Naghavi, M.; Yen, A.A.; Lin, A.H.; Tanaka, H.; Kleis, S. New indices of endothelial function measured by digital thermal monitoring of vascular reactivity: Data from 6084 patients registry. Int. J. Vasc. Med. 2016, 2016, 1348028. [Google Scholar] [CrossRef] [PubMed]
- Wu, I.W.; Hsu, K.H.; Lee, C.C.; Sun, C.Y.; Hsu, H.J.; Tsai, C.J.; Tzen, C.Y.; Wang, Y.C.; Lin, C.Y.; Wu, M.S. P-cresyl sulphate and indoxyl sulphate predict progression of chronic kidney disease. Nephrol. Dial. Transplant. 2011, 26, 938–947. [Google Scholar] [CrossRef] [PubMed]
- Motojima, M.; Hosokawa, A.; Yamato, H.; Muraki, T.; Yoshioka, T. Uremic toxins of organic anions up-regulate pai-1 expression by induction of nf-kappab and free radical in proximal tubular cells. Kidney Int. 2003, 63, 1671–1680. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, T.; Ise, M.; Seo, H.; Niwa, T. Indoxyl sulfate increases the gene expressions of tgf-beta 1, timp-1 and pro-alpha 1(i) collagen in uremic rat kidneys. Kidney Int. Suppl. 1997, 62, S15–S22. [Google Scholar]
- Lindner, A.; Charra, B.; Sherrard, D.J.; Scribner, B.H. Accelerated atherosclerosis in prolonged maintenance hemodialysis. N. Engl. J. Med. 1974, 290, 697–701. [Google Scholar] [CrossRef]
- Jacobson, S.H.; Egberg, N.; Hylander, B.; Lundahl, J. Correlation between soluble markers of endothelial dysfunction in patients with renal failure. Am. J. Nephrol. 2002, 22, 42–47. [Google Scholar] [CrossRef]
- Ioannou, K.; Stel, V.S.; Dounousi, E.; Jager, K.J.; Papagianni, A.; Pappas, K.; Siamopoulos, K.C.; Zoccali, C.; Tsakiris, D. Inflammation, endothelial dysfunction and increased left ventricular mass in chronic kidney disease (CKD) patients: A longitudinal study. PLoS ONE 2015, 10, e0138461. [Google Scholar] [CrossRef]
- Mallamaci, F.; Tripepi, G.; Cutrupi, S.; Malatino, L.S.; Zoccali, C. Prognostic value of combined use of biomarkers of inflammation, endothelial dysfunction, and myocardiopathy in patients with esrd. Kidney Int. 2005, 67, 2330–2337. [Google Scholar] [CrossRef]
- Chen, T.L.; Lee, M.C.; Ho, C.C.; Hsu, B.G.; Tsai, J.P. Serum adipocyte fatty acid-binding protein level is negatively associated with vascular reactivity index measured by digital thermal monitoring in kidney transplant patients. Metabolites 2019, 9, 159. [Google Scholar] [CrossRef]
- Barreto, F.C.; Barreto, D.V.; Liabeuf, S.; Meert, N.; Glorieux, G.; Temmar, M.; Choukroun, G.; Vanholder, R.; Massy, Z.A.; European Uremic Toxin Work Group. Serum indoxyl sulfate is associated with vascular disease and mortality in chronic kidney disease patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 1551–1558. [Google Scholar] [CrossRef]
- Lin, C.J.; Liu, H.L.; Pan, C.F.; Chuang, C.K.; Jayakumar, T.; Wang, T.J.; Chen, H.H.; Wu, C.J. Indoxyl sulfate predicts cardiovascular disease and renal function deterioration in advanced chronic kidney disease. Arch. Med. Res. 2012, 43, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.S.; Chen, J.; Zou, J.Z.; Zhong, Y.H.; Teng, J.; Ji, J.; Chen, Z.W.; Liu, Z.H.; Shen, B.; Nie, Y.X.; et al. Association of indoxyl sulfate with heart failure among patients on hemodialysis. Clin. J. Am. Soc. Nephrol. 2015, 10, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Tumur, Z.; Niwa, T. Indoxyl sulfate inhibits nitric oxide production and cell viability by inducing oxidative stress in vascular endothelial cells. Am. J. Nephrol. 2009, 29, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Dou, L.; Bertrand, E.; Cerini, C.; Faure, V.; Sampol, J.; Vanholder, R.; Berland, Y.; Brunet, P. The uremic solutes p-cresol and indoxyl sulfate inhibit endothelial proliferation and wound repair. Kidney Int. 2004, 65, 442–451. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Kim, Y.J.; Kang, D.H. Indoxyl sulfate-induced endothelial dysfunction in patients with chronic kidney disease via an induction of oxidative stress. Clin. J. Am. Soc. Nephrol. 2011, 6, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Kawagoe, Y.; Matsuda, T.; Ueda, Y.; Shimada, N.; Ebihara, I.; Koide, H. Oral adsorbent ast-120 decreases carotid intima-media thickness and arterial stiffness in patients with chronic renal failure. Kidney Blood Press. Res. 2004, 27, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Vanholder, R.; Schepers, E.; Pletinck, A.; Nagler, E.V.; Glorieux, G. The uremic toxicity of indoxyl sulfate and p-cresyl sulfate: A systematic review. J. Am. Soc. Nephrol. 2014, 25, 1897–1907. [Google Scholar] [CrossRef] [PubMed]
- Ito, S.; Osaka, M.; Edamatsu, T.; Itoh, Y.; Yoshida, M. Crucial role of aryl hydrocarbon receptor (AhR) in indoxyl sulfate-induced vascular inflammation. J. Atheroscler. Thromb. 2016, 23, 960–975. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, R.B.; Schulz, A.; Wild, P.S.; Sinning, C.R.; Wilde, S.; Eleftheriadis, M.; Herkenhoff, S.; Zeller, T.; Lubos, E.; Lackner, K.J.; et al. Noninvasive vascular function measurement in the community: Cross-sectional relations and comparison of methods. Circ. Cardiovasc. Imaging 2011, 4, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Lesniewski, L.A.; Connell, M.L.; Durrant, J.R.; Folian, B.J.; Anderson, M.C.; Donato, A.J.; Seals, D.R. B6d2f1 mice are a suitable model of oxidative stress-mediated impaired endothelium-dependent dilation with aging. J. Gerontol. Ser. A 2009, 64, 9–20. [Google Scholar] [CrossRef]
- Di Marco, G.S.; Hausberg, M.; Hillebrand, U.; Rustemeyer, P.; Wittkowski, W.; Lang, D.; Pavenstadt, H. Increased inorganic phosphate induces human endothelial cell apoptosis in vitro. Am. J. Physiol. Ren. Physiol. 2008, 294, F1381–F1387. [Google Scholar] [CrossRef] [PubMed]
- Peng, A.; Wu, T.; Zeng, C.; Rakheja, D.; Zhu, J.; Ye, T.; Hutcheson, J.; Vaziri, N.D.; Liu, Z.; Mohan, C.; et al. Adverse effects of simulated hyper- and hypo-phosphatemia on endothelial cell function and viability. PLoS ONE 2011, 6, e23268. [Google Scholar] [CrossRef] [PubMed]
- Evrard, S.; Delanaye, P.; Kamel, S.; Cristol, J.P.; Cavalier, E. SFBC/SN joined working group on vascular calcifications. Vascular calcification: From pathophysiology to biomarkers. Clin. Chim. Acta 2015, 438, 401–414. [Google Scholar] [CrossRef] [PubMed]
- Mundi, S.; Massaro, M.; Scoditti, E.; Carluccio, M.A.; van Hinsbergh, V.W.M.; Iruela-Arispe, M.L.; De Caterina, R. Endothelial permeability, LDL deposition, and cardiovascular risk factors-a review. Cardiovasc. Res. 2018, 114, 35–52. [Google Scholar] [CrossRef] [PubMed]
- Souweine, J.S.; Corbel, A.; Rigothier, C.; Roque, C.D.; Hadjadj, S.; Cristol, J.P.; Combe, C.; Bigot-Corbel, E.; Beauvieux, M.C.; groupe de travail SFBC, SFNDT, SNP. Interest of albuminuria in nephrology, diabetology and as a marker of cardiovascular risk. Ann. Biol. Clin. 2019, 77, 26–35. [Google Scholar]
- National Kidney Foundation. K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am. J. Kidney Dis. 2003, 42, S1–S201. [Google Scholar] [CrossRef]
- Steuer, C.; Schutz, P.; Bernasconi, L.; Huber, A.R. Simultaneous determination of phosphatidylcholine -derived quaternary ammonium compounds by a lc-ms/ms method in human blood plasma, serum and urine samples. J. Chromatogr. B 2016, 1008, 206–211. [Google Scholar] [CrossRef]
- Shu, C.; Chen, X.; Xia, T.; Zhang, F.; Gao, S.; Chen, W. LC-MS/MS method for simultaneous determination of serum p-cresyl sulfate and indoxyl sulfate in patients undergoing peritoneal dialysis. Biomed. Chromatogr. 2016, 30, 1782–1788. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | All Patients (n = 110) | Good Vascular Reactivity (n = 53) | Intermediate Vascular Reactivity (n = 36) | Poor Vascular Reactivity (n = 21) | p Value |
|---|---|---|---|---|---|
| VRI | 1.82 ± 0.72 | 2.44 ± 0.30 | 1.55 ± 0.29 | 0.72 ± 0.26 | < 0.001 * |
| Age (years) | 65.89 ± 7.94 | 64.09 ± 8.40 | 66.31 ± 6.99 | 69.71 ± 7.07 | 0.020 * |
| Female, n (%) | 50 (45.5) | 26 (49.1) | 13 (36.1) | 11 (52.4) | 0.377 |
| Height (cm) | 159.33 ± 9.04 | 160.08 ± 9.23 | 158.71 ± 9.13 | 158.50 ± 8.64 | 0.705 |
| Body weight (kg) | 67.55 ± 14.12 | 67.62 ± 14.30 | 68.06 ± 13.75 | 66.51 ± 14.89 | 0.924 |
| BMI (kg/m2) | 26.51 ± 4.66 | 26.32 ± 4.97 | 26.94 ± 4.45 | 26.25 ± 4.34 | 0.796 |
| Diabetes mellitus, n (%) | 54 (49.1) | 28 (52.8) | 15 (41.7) | 11 (52.4) | 0.554 |
| Hypertension, n (%) | 91 (82.7) | 42 (79.2) | 29 (80.6) | 20 (95.2) | 0.238 |
| Smoking, n (%) | 13 (11.8) | 3 (5.7) | 4 (11.1) | 6 (28.6) | 0.022 * |
| SBP (mmHg) | 145.65 ± 24.24 | 139.94 ± 20.39 | 145.28 ± 20.31 | 160.71 ± 32.78 | 0.003 * |
| DBP (mmHg) | 83.86 ± 11.94 | 81.15 ± 10.17 | 83.61 ± 10.33 | 91.14 ± 15.69 | 0.004 * |
| BUN (mg/dL) | 31.00 (23.00–45.75) | 27.00 (22.50–38.00) | 32.00 (24.25–49.75) | 63.00 (31.00–75.00) | 0.001 * |
| Creatinine (mg/dL) | 1.75 (1.40–2.50) | 1.70 (1.30–2.35) | 1.75 (1.43–2.20) | 3.70 (2.20–5.70) | 0.001 * |
| eGFR (mL/min) | 33.34 ± 15.76 | 37.93 ± 13.96 | 34.51 ± 15.19 | 19.74 ± 13.85 | < 0.001 * |
| CKD stage 3, n (%) | 63 (57.3) | 37 (69.8) | 21 (58.3) | 5 (23.8) | < 0.001 * |
| CKD stage 4, n (%) | 27 (24.5) | 13 (24.5) | 9 (25.0) | 5 (23.8) | |
| CKD stage 5, n (%) | 20 (18.2) | 3 (5.7) | 6 (16.7) | 11 (52.4) | |
| Total cholesterol (mg/dL) | 159.54 ± 47.24 | 158.68 ± 47.71 | 150.75 ± 42.33 | 176.76 ± 51.56 | 0.132 |
| Triglyceride (mg/dL) | 124.50 (93.50–172.00) | 119.00 (94.50–168.50) | 123.00 (89.25–160.25) | 131.00 (99.50–213.50) | 0.396 |
| LDL-C (mg/dL) | 90.38 ± 38.96 | 92.43 ± 42.01 | 82.06 ± 32.69 | 99.48 ± 39.88 | 0.232 |
| Fasting glucose (mg/dL) | 105.00 (98.00–141.00) | 105.00 (99.50–140.50) | 101.00 (97.00–139.00) | 109.00 (96.50–160.50) | 0.635 |
| Albumin (mg/dL) | 4.11 ± 0.39 | 4.16 ± 0.42 | 4.08 ± 0.29 | 4.05 ± 0.46 | 0.512 |
| Globulin (mg/dL) | 2.90 (2.80–3.20) | 2.90 (2.80–3.15) | 3.00 (2.80–3.16) | 2.90 (2.70–3.25) | 0.932 |
| Total calcium (mg/dL) | 8.88 (8.60–9.25) | 8.88 (8.72–9.28) | 8.90 (8.51–9.31) | 8.80 (8.46–9.06) | 0.231 |
| Phosphorus (mg/dL) | 3.89 ± 0.95 | 3.68 ± 0.64 | 3.91 ± 0.94 | 4.38 ± 1.39 | 0.016 * |
| Indoxyl sulfate (μg/mL) | 1.33 (0.53–4.58) | 0.70 (0.32–1.49) | 1.56 (0.54–4.02) | 16.32 (10.63–26.44) | < 0.001 * |
| ARB use, n (%) | 57 (51.8) | 28 (52.8) | 18 (50.0) | 11 (52.4) | 0.965 |
| β-blocker use, n (%) | 35 (31.8) | 13 (24.5) | 11 (30.6) | 11 (52.4) | 0.067 |
| α-blocker use, n (%) | 20 (18.2) | 7 (13.2) | 7 (19.4) | 6 (28.6) | 0.295 |
| CCB use, n (%) | 46 (41.8) | 20 (37.7) | 13 (36.1) | 13 (61.9) | 0.115 |
| Statin use, n (%) | 55 (50.0) | 29 (54.7) | 15 (41.7) | 11 (52.4) | 0.468 |
| Fibrate use, n (%) | 9 (8.2) | 5 (9.4) | 3 (8.3) | 1 (4.8) | 0.803 |
| Variables | Vascular Reactivity Index | ||||
|---|---|---|---|---|---|
| Univariate | Multivariate | ||||
| r | p Value | Standardized Beta | Adjusted R2 Change | p Value | |
| Female | 0.085 | 0.379 | − | − | − |
| Diabetes mellitus | −0019 | 0.847 | − | − | − |
| Hypertension | −0.070 | 0.466 | − | − | − |
| Smoking | −0.207 | 0.030 * | − | − | − |
| Age (years) | −0.264 | 0.005 * | − | − | − |
| Height (cm) | 0.018 | 0.853 | − | − | − |
| Body weight (kg) | −0.007 | 0.945 | − | − | − |
| Body mass index (kg/m2) | −0.016 | 0.868 | − | − | − |
| Systolic blood pressure | −0.243 | 0.011 * | − | − | − |
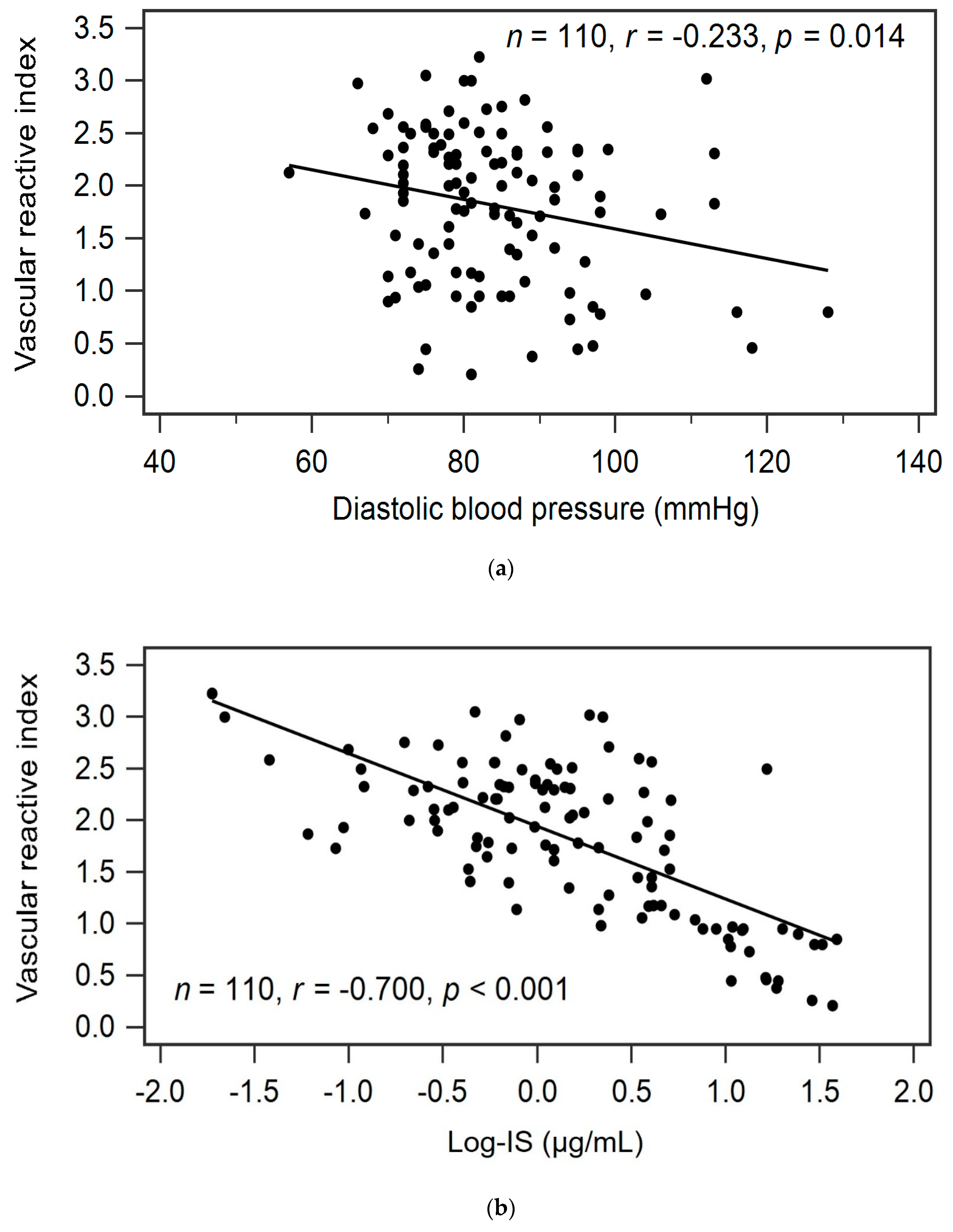
| Diastolic blood pressure | −0.233 | 0.014 * | −0.142 | 0.016 | 0.040 * |
| Total cholesterol (mg/dL) | 0.017 | 0.857 | − | − | − |
| Log-Triglyceride (mg/dL) | −0.106 | 0.271 | − | − | − |
| LDL-C (mg/dL) | 0.067 | 0.486 | − | − | − |
| Log-Glucose (mg/dL) | 0.002 | 0.983 | − | − | − |
| Log-BUN (mg/dL) | −0.337 | < 0.001 * | − | − | − |
| Log-Creatinine (mg/dL) | −0.386 | < 0.001 * | − | − | − |
| eGFR (mL/min) | 0.350 | < 0.001 * | − | − | − |
| Albumin (mg/dL) | 0.097 | 0.311 | − | − | − |
| Log-Globulin (mg/dL) | 0.054 | 0.579 | − | − | − |
| Log-Calcium (mg/dL) | 0.126 | 0.190 | − | − | − |
| Phosphorus (mg/dL) | −0.228 | 0.017 * | − | − | − |
| Log-IS (μg/mL) | −0.700 | < 0.001 * | −0.681 | 0.485 | < 0.001 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.-H.; Lai, Y.-H.; Kuo, C.-H.; Lin, Y.-L.; Tsai, J.-P.; Hsu, B.-G. Association between Serum Indoxyl Sulfate Levels and Endothelial Function in Non-Dialysis Chronic Kidney Disease. Toxins 2019, 11, 589. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11100589
Wang C-H, Lai Y-H, Kuo C-H, Lin Y-L, Tsai J-P, Hsu B-G. Association between Serum Indoxyl Sulfate Levels and Endothelial Function in Non-Dialysis Chronic Kidney Disease. Toxins. 2019; 11(10):589. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11100589
Chicago/Turabian StyleWang, Chih-Hsien, Yu-Hsien Lai, Chiu-Huang Kuo, Yu-Li Lin, Jen-Pi Tsai, and Bang-Gee Hsu. 2019. "Association between Serum Indoxyl Sulfate Levels and Endothelial Function in Non-Dialysis Chronic Kidney Disease" Toxins 11, no. 10: 589. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11100589